


IgG4-related disease (IgG4-RD) is a recently recognized clinical condition with multiple aspects not yet elucidated. It is characterized by a fibrous inflammatory process that involves multiple organs and clinical, serological and histopathological findings, which represent a major challenge for the clinician. Classically described as an expansive tumor lesion with storiform fibrosis, lymphoplasmacytic infiltration (IgG4-positive) and elevated serum IgG4. Clinical features are variable, and pancreatic as well as extrapancreatic involvement has been reported, more frequently in Asian men over 50 years and rarely described in black people. We report the case of an Afro-Colombian teenage woman, who had a unilateral ocular protrusion of unknown cause, with histopathologic findings that revealed infiltration of lymphocyte and plasma cells into the lacrimal gland. It was positive for IgG4, ruling out other conditions, and confirming IgG4-related dacryoadenitis.
La enfermedad relacionada con IgG4 (ER-IgG4) es una condición clínica recientemente reconocida, con múltiples aspectos aún no dilucidados. Se caracteriza por el compromiso fibroinflamatorio de múltiples órganos; con hallazgos clínicos, serológicos e histopatológicos que representa un importante reto para el clínico. Clásicamente descrita como una lesión tumoral expansiva con fibrosis estoriforme, infiltración linfoplasmocítica (IgG4 positiva) e IgG4 sérica elevada. Las características clínicas son variables, se describe tanto compromiso pancreático como extrapancreático, es de predominio en varones asiáticos mayores de 50 años, y rara vez es descrita en personas de raza negra. Presentamos el caso de una mujer, adolescente, afro-colombiana, que presenta protrusión ocular unilateral inexplicable, con hallazgos histopatológicos que revelan infiltración de células linfocíticas y plasmáticas en la glándula lacrimal, con positividad para IgG4, descartándose otras condiciones, lo que confirma una dacrioadenitis por enfermedad relacionada con IgG4.
Immunoglobulin (Ig) G4-related disease (IgG4-RD) is an immune-mediated inflammatory condition that mimics autoimmune and infectious disorders and malignancies, with specific organ or multisystemic involvement.1 It is most prevalent in Asian men, between the fifth and sixth decades of life, with orbital involvement being the most widespread extrapancreatic manifestation.2 We report a case of dacryoadenitis in an Afro-Colombian adolescent as an uncommon form of IgG4-RD.
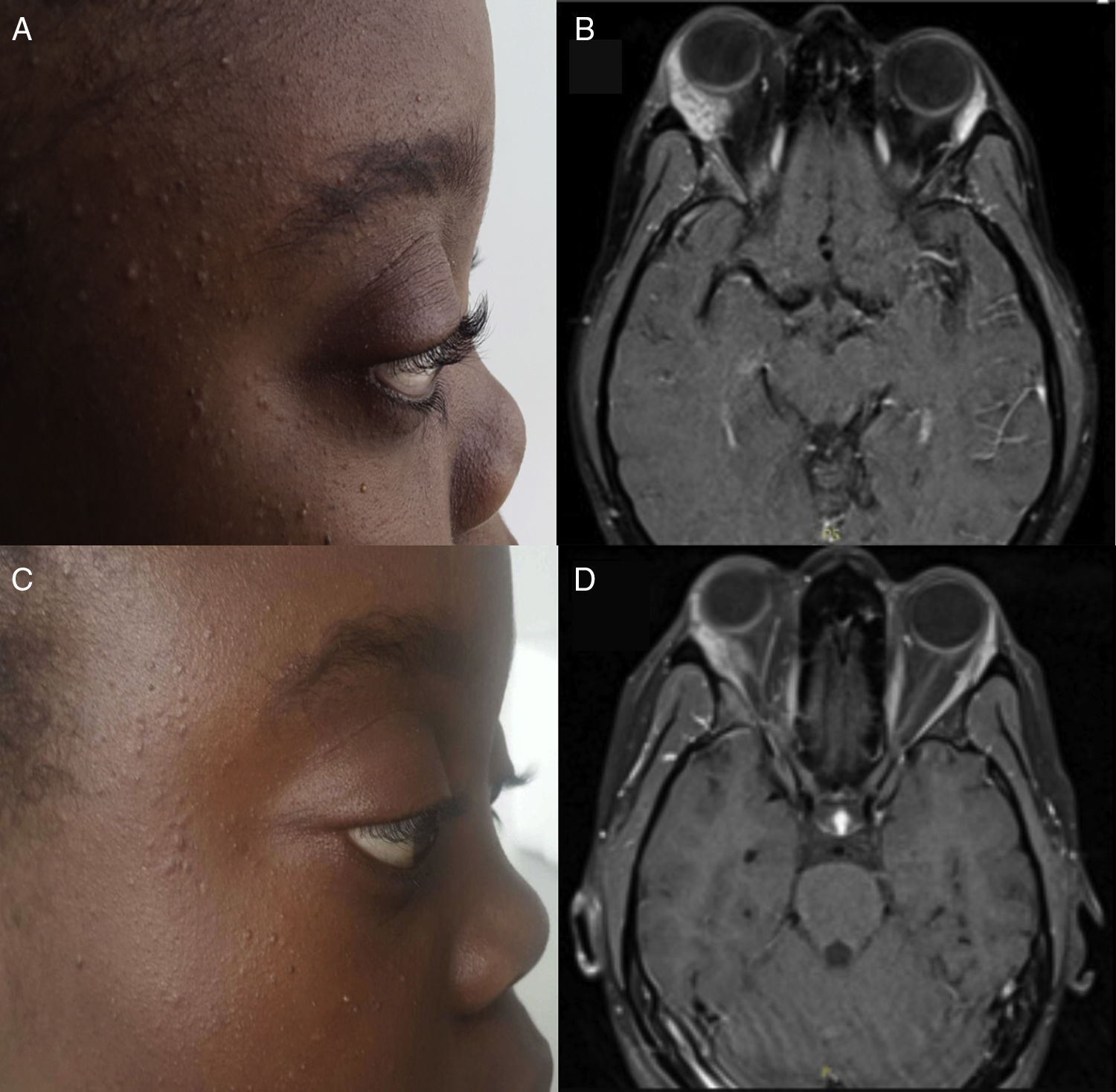
Case DescriptionThe patient was a 13-year-old Afro-Colombian girl. She presented with ocular pain and proptosis in right eye that had begun 7 days earlier (Fig. 1A); she mentioned nothing similar in her history. The ophthalmological study found orbital asymmetry and lowered gaze and proptosis in right eye (exophthalmometry in right eye 22mm, left eye 18mm). Orbital magnetic resonance imaging (MRI) showed an increase in the size of right lacrimal gland causing a mass effect, suggestive of an inflammatory or neoplastic process, with no bone involvement.
 Right proptosis at the onset of the clinical symptoms. (B) T1-weighted postcontrast cross-sectional magnetic resonance image (MRI) at admission. Note the enlargement of right lacrimal gland, with enhancement after the administration of contrast medium. (C) Decrease in proptosis after 1 year of follow-up. (D) T1-weighted postcontrast cross-sectional MRI after 1 year of follow-up. Note the decrease in the size of right lacrimal gland versus baseline MRI.")
(A) Right proptosis at the onset of the clinical symptoms. (B) T1-weighted postcontrast cross-sectional magnetic resonance image (MRI) at admission. Note the enlargement of right lacrimal gland, with enhancement after the administration of contrast medium. (C) Decrease in proptosis after 1 year of follow-up. (D) T1-weighted postcontrast cross-sectional MRI after 1 year of follow-up. Note the decrease in the size of right lacrimal gland versus baseline MRI.
Chest and abdominal computed tomography, an aspirate, bone marrow biopsy and immunophenotype, infectious markers (enzyme-linked immunosorbent assay for human immunodeficiency virus, anti-hepatitis C virus, hepatitis B surface antigen, anti-hepatitis B core antibody), thyroid-stimulating hormone/free thyroxine, C-reactive protein, erythrocyte sedimentation rate, complement (C3–C4), antinuclear antibodies, extractable nuclear antigens, antineutrophil cytoplasmic antibodies and serum immunoglobulin levels were normal or negative; the latter ruled out the presence of paraproteinemia and humoral immunodeficiencies.
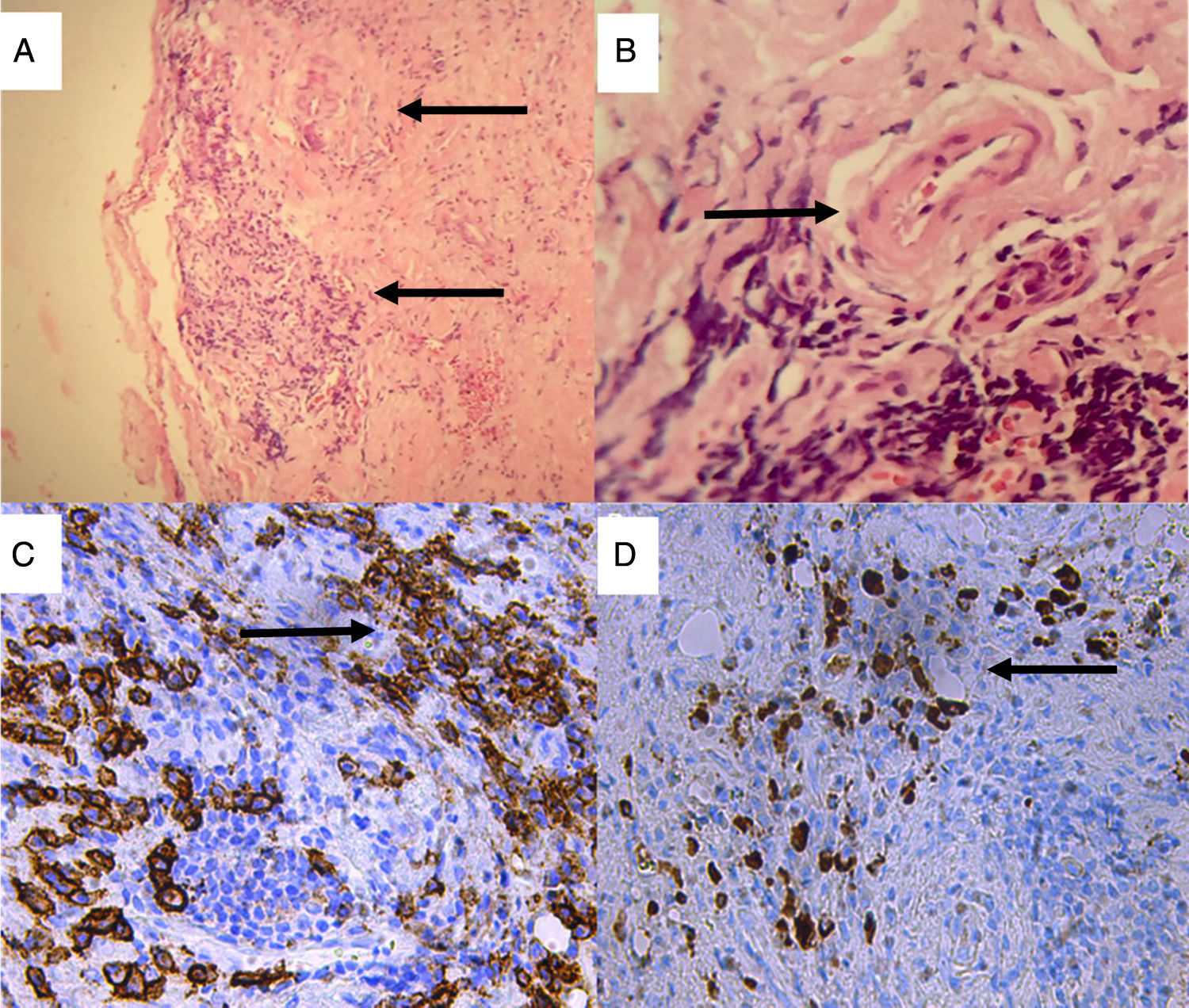
The biopsy of right lacrimal gland revealed storiform fibrosis, stromal sclerosis, obliterative phlebitis and inflammatory infiltrate (Fig. 2A and B). Inflammatory pseudotumor was considered by the pediatricians, and treatment was begun with prednisone at 50mg/day.
![Lacrimal gland biopsy. Hematoxylin–eosin staining: (A) Storiform fibrosis, stromal sclerosis and chronic inflammatory infiltrate (×10); (B) Veins with walls swollen with the infiltration of mononuclear inflammatory cells causing obliteration of the lumen. Immunohistochemical staining (×40). (C) Extensive infiltration of plasma cells expressing CD (cluster of differentiation) 38 (anti-CD38 with 3,3′-diaminobenzidine [DAB] staining, ×40); (D) IgG4-positive plasma cells (anti-IgG4 DAB staining, ×40).](https://static.elsevier.es/multimedia/21735743/0000001400000003/v1_201805120507/S2173574318300194/v1_201805120507/en/main.assets/gr2.jpeg?xkr=ue/ImdikoIMrsJoerZ+w9184xd8ym1IgxXJ6I4p31f1upH6Ra9/FExf9t4wRA9EI6B7mhhKGxAjY9TNLFxD1JZ7jlBWBpl7Ht+2zY/Xaz1QDB/e40CpLkfWuMQecFuQ0+vdKvrvTenO9J37WKm0LFddgfvLPXo3X6Yk2Ur7MLE515IkePShAyjYbDyWw3TobyOuH5ZLGicPSm3EAf8qj01LBLRIzPZd4hos1MkPKEKTR1XPK+kH7vS4oVUbEYhfnhNd9EFXrKDvdeqoSSfME3VWorPqSKXEPyjlcyxLntgE= "Lacrimal gland biopsy. Hematoxylin–eosin staining: (A) Storiform fibrosis, stromal sclerosis and chronic inflammatory infiltrate (×10); (B) Veins with walls swollen with the infiltration of mononuclear inflammatory cells causing obliteration of the lumen. Immunohistochemical staining (×40). (C) Extensive infiltration of plasma cells expressing CD (cluster of differentiation) 38 (anti-CD38 with 3,3′-diaminobenzidine [DAB] staining, ×40); (D) IgG4-positive plasma cells (anti-IgG4 DAB staining, ×40).")
Lacrimal gland biopsy. Hematoxylin–eosin staining: (A) Storiform fibrosis, stromal sclerosis and chronic inflammatory infiltrate (×10); (B) Veins with walls swollen with the infiltration of mononuclear inflammatory cells causing obliteration of the lumen. Immunohistochemical staining (×40). (C) Extensive infiltration of plasma cells expressing CD (cluster of differentiation) 38 (anti-CD38 with 3,3′-diaminobenzidine [DAB] staining, ×40); (D) IgG4-positive plasma cells (anti-IgG4 DAB staining, ×40).
Follow-up MRI performed 9 months later in rheumatology showed a reduction in the size of the lacrimal gland, and serum IgG4 was normal. An immunohistochemical study revealed an extensive infiltrate of IgG4+ plasms cells with an IgG4/IgG ratio>40% consistent with dacryoadenitis associated with IgG4-RD (Fig. 2C and D). Treatment was begun with azathioprine, as a steroid sparing agent, which achieved sustained clinical and radiological improvement (Fig. 1C and D).
DiscussionIgG4-related disease is a fibroinflammatory, multiorgan, immune-mediated condition,1 described in 1961 in the context of pancreatitis associated with hypergammaglobulinemia. It was later associated with high serum IgG4 levels and, in 2003, was recognized as a systemic disease when extrapancreatic manifestations were described.3 IgG4 is the least abundant of the subclasses of IgG. It is a poor activator of the classical complement cascade and its production is induced by interleukin (IL) 10 (T regulatory cells and T helper cells [Th2]). Although the physiological mechanism of IgG4-RD is not clearly elucidated, associations with human leukocyte antigen (HLA) polymorphisms (HLA DRB1*0405, DQB1*0401 or DQβ1-57) have been described, molecular mimicry between Helicobacter pylori and proteins of pancreatic acinar cells,4 just as IgG4 specifies 17 salivary and lacrimal gland antigens (IgG4 complex analysis), which could explain the preferential involvement of these organs5 (Fig. 2).
The diagnosis of IgG4-RD is based on clinical and radiological findings, as well as serological evidence (IgG4≥135mg/dL) and histological manifestations (storiform fibrosis, obliterative phlebitis and tissue infiltration by >10 IgG4+ plasma cells per high-power field with a IgG4:IgG>40%).6 Our patient met all of the criteria except for the serological finding, but IgG4 may not have been detected because she had been taking steroids for 9 months.
Autoimmune pancreatitis is the most common presentation, whether or not it is associated with extrapancreatic involvement. Periorbital tissue is among the regions most frequently involved (in up to 39% of the patients).7 IgG4-related diseases predominantly affect men over 50 years of age. The majority of the patients are Asian, especially Japanese, and the prevalence is estimated to be 6 cases per 100,000 population.8 We found 1 case of dacryoadenitis reported in Latin America, in a study involving biopsy specimens,9 but none in Afro-descendant adolescent women or the pediatric population. This is the second case of dacryoadenitis associated with IgG4-RD in a child reported in the literature, preceded only by that of a 13-year-old white North American girl.10
Oral corticosteroids, with or without azathioprine or mycophenolate mofetil, are the treatment of choice. Our patient received prednisone as monotherapy for 9 months. The addition of azathioprine on the part of the rheumatology department enabled us to reduce the steroid dose, achieving a satisfactory clinical and radiological response.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of InterestThe authors declare they have no conflicts of interest.
Please cite this article as: Díaz-Ramírez GS, Medina-Quintero LF, Salinas-César A, Zea-Vera AF. Dacrioadenitis por enfermedad relacionada con IgG4 en una adolescente afrodescendiente de Colombia. Reumatol Clin. 2018;14:164–167.


