

Rheumatoid arthritis is a chronic systemic inflammatory disease that causes significant morbidity and mortality. The combined use of methotrexate and biological agents, which directed against tumor necrosis factor (TNF) has achieved significant improvement in clinical, radiographic and functional parameters not seen previously and has revolutionized the therapeutic goal of achieving remission in clinical, structural and functional parameters. The next goal should be to achieve remission without the use of biological drugs and later without medication. Although there is evidence about the efficacy and safety of TNF inhibitors, there is none on remission without the use of biological agents or disease modifying drugs.
La artritis reumatoide es una enfermedad inflamatoria crónica sistémica que ocasiona una significativa morbilidad y mortalidad. El uso combinado de metotrexato y agentes biológicos dirigidos contra el factor de necrosis tumoral (TNF) ha logrado mejorías significativas en parámetros clínicos, radiográficos y funcionales que no se habían visto previamente y que han revolucionado el objetivo terapéutico de conseguir la remisión en parámetros clínicos, estructurales y funcionales. El próximo objetivo debería ser alcanzar la remisión sin el uso de fármacos biológicos y posteriormente sin medicación. Aunque hay evidencia acerca de la eficacia y la seguridad de los inhibidores del TNF, no la hay acerca de remisión sin el empleo de agentes biológicos ni fármacos modificadores de la enfermedad.
Rheumatoid arthritis (RA) is the most prevalent chronic inflammatory joint disease and affects 0.5%–1% of the population of our country. Without proper treatment it causes significant morbidity and mortality. The introduction of biological therapies has significantly improved clinical outcomes and functional imaging of patients. The therapeutic goal in clinical practice is to try to achieve remission or low disease activity.1 Once achieved, it is advisable (if possible) to reduce or remove biological treatment and reduction and removal of disease-modifying drugs (DMARDs).1 The aim of this review is to analyze the possibility of suspending medication in patients with RA in prolonged remission and when the risk of recurrence exists with suspension.
Definition of RemissionAlthough still far from curing the disease, recent years have seen changes in the therapeutic strategies in RA with early use of DMARDs and the introduction of biological therapies, which led to better results in RA treatment, in order to achieve remission or low disease activity level.2
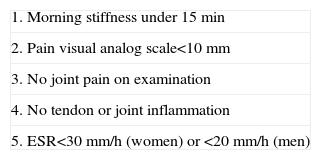
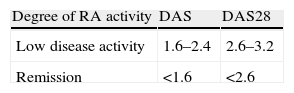
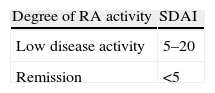
In the 1990s various organizations, such as the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) proposed a number of variables to be assessed at each patient visit and included the quantification of painful (TJC) and swollen joints (SJC), the assessment of pain and disease activity by both the patient and physician through a visual analog scale (VAS), functional capacity of patients and acute phase reactants (ESR and CRP). From these variables, the proposed definitions of remission were: the ACR through the fulfillment of criteria (ACR criteria) (Table 1), and EULAR through an index (DAS) (Table 2). Another index that has been proposed is SDAI (Simplified Disease Activity Index), which has the advantage that it is performed through a calculated arithmetic sum of the SJC in 28 joints (SJC28), and TJC in 28 joints (TJC28), patient and physician VAS and CRP (Table 3).3 Although there are currently no remission criteria universally accepted, these are the indices used. Therefore, both ACR and EULAR are working together to validate criteria that define what remission is, and this collaboration has recently published provisional criteria whose application is intended for clinical4 trials.
Modified ACR Remission Criteria (1995).
| 1. Morning stiffness under 15 min |
| 2. Pain visual analog scale<10mm |
| 3. No joint pain on examination |
| 4. No tendon or joint inflammation |
| 5. ESR<30mm/h (women) or <20mm/h (men) |
ACR: American College of Rheumatology; ESR: Erythrocyte Sedimentation Rate.
aAt least 4 criteria must be present for at least 3 months.
Modified from Balsa.3
EULAR Remission Criteria (DAS and DAS28).
| Degree of RA activity | DAS | DAS28 |
| Low disease activity | 1.6–2.4 | 2.6–3.2 |
| Remission | <1.6 | <2.6 |
Modified from Balsa.3
SDAI (Simple Disease Activity Index).
| Degree of RA activity | SDAI |
| Low disease activity | 5–20 |
| Remission | <5 |
Modified from Balsa.3
Remission can be defined as a state in which there is no inflammatory activity and no progression of structural damage. This concept of remission is difficult to achieve in clinical practice, because there the concept does not rule out the subclinical activity detectable by imaging5 techniques. Therefore, many authors propose therapy to achieve a state of low disease activity as an alternative.
Withdrawal of Treatment in Remission of Early Rheumatoid Arthritis PatientsIt is increasingly clear that early treatment with DMARDs in RA results in lower long-term6 radiological damage.7 In RA there seems to be a period called “window of opportunity” in which the appropriate treatment may suppress or even reverse disease activity and lead the patient to an asymptomatic state, slowing joint damage. This window of opportunity presents itself at an early stage of the disease, lasting approximately 12 weeks.6,7 The need for early diagnosis has conditioned the recent publication by ACR and EULAR of diagnostic criteria for RA 9, whose purpose is to achieve an earlier diagnosis of disease.8
Among the studied that have reviewed the possible withdrawal of treatment in patients with early RA we find the following.
A Finnish cohort of early RA (n=70 patients) with a mean duration at the time of inclusion of 8 months was treated with DMARD monotherapy, or in combination in cases of ineffective response. They studied remission without medication and remission in a period of about 15 years.9 Patients were divided into 3 groups according to the pattern of DMARD received. DMARD were suspended only in patients who remained in remission with 1981 ACR criteria for at least 12 months or who for a long time had low disease activity without symptoms. Twenty patients were able to discontinue medication, of which 9 had to restart treatment after a mean 50 months, most of them again reached low levels of activity. One possible explanation might be that patients were in remission after stopping the medication and therefore only patients with true clinical remission should discontinue DMARDs.
The study enrolled 508 BeSt10 patients with early RA of less than 2 years of progression (mean disease duration of 23 weeks) and were assigned to 4 treatment strategies: sequential monotherapy with DMARDs (group 1), combined step-up therapy (group 2), combination therapy with high doses of prednisone (group 3) or with infliximab (group 4). Treatment adjustments were made every 3 months with the aim of reaching a state of low activity according to DAS (DAS<2.4). If the clinical response with monotherapy was adequate for 6 months, medication was discontinued. In the analysis of remission without treatment after 5 years of follow up,11 the authors found that 23% of patients achieved remission without treatment, without differences between groups, but in 46% of these patients DMARDs had to be restarted upon reactivation of the disease, with retreatment being effective in 96%.
Withdrawal of Treatment in the Remission of Established Rheumatoid ArthritisPatients with established RA (more than 2 years of evolution) have sequelae in the form of joint erosions. In these patients, the theory of “the window of opportunity” is no longer achievable to reverse the disease,6,7 so reaching remission without treatment is more complicated.
Various studies have addressed the suspension of treatment with DMARDs in patients with established RA in remission. Among them we highlight the following.
In a Swiss cohort of 304 patients with established RA, predictors of long-term remission were studied after stopping anti-TNF-α therapy in patients who were in remission (DAS28<2.6) for at least 6 months with a stable dose of both the biologic and prednisone (<5mg) and without NSAID.12 Twenty (6.9%) patients met criteria for stopping biological therapy with a mean time of 11.3 years, and a mean of 19.4 months in remission with anti-TNF-α. At one year, 16 (71%) patients required re-treatment with anti-TNF-α for recurrence after a mean 14.7 weeks. Baseline differences in patients who relapsed compared to those who remained in remission were the least time in treatment with anti-TNF-α (35 months vs 56 months) and a shorter time in remission before stopping anti-TNF (14.5 months vs 35 months). However, the sample size was small.
In a Japanese multicenter study of induction of remission in RA treated with infliximab (RRR study),13 those subjects who achieved a low level of activity (DAS28<3.2) for more than 24 months were invited to stay on infliximab. One hundred and two patients, of which 83 were in clinical remission, with a mean disease duration of 5.9 years, agreed to suspend infliximab and participate in the study. At one year, 56 (55%) patients remained on a low level of activity, 44 of them in remission, while the disease recurred in 46 patients. In these, retreatment with infliximab was effective in 32 of them reaching a low level of activity within 6 months. Patients who achieved remission had lower duration of illness (4.8 vs 7.8 years) and less radiographic progression.
In a prospective study involving 47 patients with RA treated with methotrexate and biological therapy (anti-TNF-α) in remission according to EULAR criteria (DAS28<2.6),14 27 patients (mean duration of disease 19 months) received combination therapy as first-line treatment for 12 months and 20 patients (mean duration of illness of 120 months) were treated with biological therapy (anti-TNF-α) after inadequate response to DMARDs. It was observed that a shorter duration of disease was a predictor of remission.
Recently, there has been a meta-analysis of high-quality studies that included patients with RA of more than 2 years and in remission with DMARD treatment, who suspended medication.15 It was observed that the suspension of medication must be done in a careful manner, monitoring the degree of disease activity to restart treatment as early as possible.
ConclusionsThe therapeutic goal in RA is to attain remission or at least a low activity, to introduce DMARD therapy as early as possible, to induce remission or low disease activity and, if feasible, achieve remission without treatment.
We do not have enough information about patients who should stop treatment and when to stop it when remission of the disease is reached.
In early RA, the “window of opportunity” can be used for treatment with DMARDs alone or in combination to induce remission and prevent radiological deterioration. In patients with sustained clinical remission after a year of therapy, one could try stopping the medication and closely monitoring patients looking for signs of activity in order to reintroduce therapy as soon as possible.
In established RA treatment, discontinuation is more controversial. One could try to suspend it in patients with RA in remission for at least a year, with close monitoring to reintroduce it when activity is detected.
There is no data to establish guidelines regarding the possibility of reducing treatment dose or prolonging the administration time interval.1
DisclosuresThe authors have no disclosures to make.
Please cite this article as: Nóvoa Medina FJ, Francisco Hernández F. ¿Se puede suspender la medicación en los pacientes con artritis reumatoide en remisión? Reumatol Clin. 2012;8(1):39–41.


