








The peripheral microangiopathy may be well evaluated and studied by nailfold capillaroscopy (NFC) which is a safe and non-invasive technique. NFC has been reported to have both diagnostic and prognostic values in patients presenting with Raynaud's phenomenon.
ObjectiveThe overarching objective of this work was to make a consensus on what domains should be included in a capillaroscopy report and that it can be used in daily clinical practice and clinical research in the area of rheumatology.
MethodsA Delphi questionnaire was developed regarding capillaroscopy report from a literature review and expert consensus. The first Delphi round included 14 core areas, its 18 domains with 50 subdomains, derived from a systematic literature review. The level of evidence was determined for each core set using the Oxford Centre for Evidence-based Medicine (CEBM) system. Nine response categories have been set per each item ranging between 1 and 9. Round 2, aimed to reach preliminary consensus “in” or “out” for domains. It included all items that were rated “critical” by at least 80% of the participants as well as any new domains proposed in round 1.
ResultsThe participants to the first, and second round were 11 experts. Fourteen domains were discussed in the two rounds. At the end of the survey, the final report template of NFC in rheumatology reached a consensus.
ConclusionA nailfold capillaroscopy report template has been developed by this study, based on outcomes of a Delphi process, by international participants panel. All domains met the 80% voting threshold set in this work. The reporting template can be used for both clinical research as well as day to day practice to provide guidance and standardize the NFC reporting.
La microangiopatía periférica puede ser evaluada y estudiada adecuadamente mediante capilaroscopia ungueal (NFC), que es una técnica segura y no invasiva. Se ha informado que la NFC tiene valores tanto diagnósticos como pronósticos en pacientes que presentan el fenómeno de Raynaud.
ObjetivoEl objetivo general de este trabajo fue aportar de manera objetiva y lograr un consenso sobre los dominios que se incluirán en los resultados de un modelo de informe de la NFC y que pueda ser aplicable tanto para la práctica clínica estándar como para la investigación clínica en reumatología.
MétodosSe elaboró un cuestionario Delphi sobre el informe de capilaroscopia a partir de una revisión bibliográfica y del consenso de expertos. La primera ronda Delphi incluyó 14 áreas centrales, sus 18 dominios con 50 subdominios, derivados de una revisión sistemática de la literatura. El nivel de evidencia se determinó para cada conjunto básico utilizando el sistema del Centro de Medicina basada en la Evidencia de Oxford. Se han establecido 9 categorías de respuesta para cada ítem, que oscilan entre 1 y 9. La ronda 2 tenía como objetivo llegar a un consenso preliminar «dentro» o «fuera» de los dominios. Incluía todos los elementos que fueron calificados como «críticos» por al menos el 80% de los participantes, así como cualquier dominio nuevo propuesto en la ronda 1.
ResultadosEn la primera y segunda ronda participaron 11 expertos. En las 2 rondas se discutieron 14 dominios. Al final de la encuesta, el modelo de informe final de la NFC en reumatología alcanzó un consenso.
ConclusiónEste estudio desarrolló una plantilla de informe de capilaroscopia ungueal, basada en los resultados de un proceso Delphi por un panel internacional de participantes. Todos los dominios alcanzaron el umbral de votación del 80% establecido en este trabajo. La plantilla de informes se puede utilizar tanto para la investigación clínica como para la práctica diaria, para proporcionar orientación y estandarizar los informes de la NFC.
Over the past years, nailfold capillaroscopy (NFC) has gained popularity and its use among rheumatologists has increased substantially. Basically, the microvascular damage has been defined as progressive alteration of the capillaries structure and morphology with progressive decrease in their density, together with alternation of the blood flow.1 Consequently, assessment of peripheral microcirculation has booked its place as an important tool for valuation of patients with Raynaud's phenomenon and for the early diagnosis of systemic sclerosis. In addition, there Is also some evidence indicating positive relation between changes in the nailfold capillaroscopic pattern and the affection of target organs. The recognition of the capillaroscopic patterns characterizing the secondary Raynaud's phenomenon (RP) has been proposed as a prognostic marker for the early detection of the risk of visceral RP (e.g. coronary heart disease).2,3
The NFC reproducibility and credentials has attracted the attention, as regular monitoring and assessment of nailfold capillaroscopy may soon be considered a tool for the analysis not only of the peripheral circulation in autoimmune rheumatic diseases but also the microvascular systemic organ affection.4,5 However, whilst nailfold capillaroscopy may represent the best method to analyze microvascular abnormalities in autoimmune rheumatic diseases, uncertainty may arise when documentation and reporting of the findings of the procedure are not standardized. Given the rapidly growing use of NFC by a variety of healthcare professionals in both the standard day to day practice as well as in research context to predict the disease progression and monitor treatment effects, a barrier for further evaluation is the lack of consensus on how to document the demographics/outcomes of the assessment. Therefore, standardization of the NFC reporting seems paramount. To step forward to this need, experts in the field of capillaroscopy/microcirculation provide in this evidence-based consensus study their view on determining the core set domains for nailfold capillaroscopy (NFC) reporting, for both clinical practice as well as clinical research.
MethodsDesignThe evidence-based consensus was developed adopting a multistep process strategy: 1. Formulation of the overarching principles of NFC reporting; 2. Identify the candidate core items and domains; 3. Literature search for core items and domains of NFC reporting; 4. Critical assessment and selection of the evidence; 5. Presentation of results, and recommendations. This work led to the development of a draft core set of domains (and subdomains) to be included in the NFC reporting. The domains were stratified into those ones which were part of the inner core set (essential to NFC reporting), middle core set (relevant but not essential to assess in NFC reporting) or outer core (should be part of a research agenda). The study design was formulated based on the “Clinical, Evidence-based, Guidelines (CEG)” guideline development process protocol which involves a scientific evidence and consensus, based on the existing scientific evidence and clinical experience. The manuscript conformed to the preferred reporting items for systematic reviews and meta-analyses guidelines for reporting systematic reviews.6
Development stagesCore teamThis was composed of three experts who are all professionally involved in doing nailfold capillaroscopy (NFC). With recognized experience in NFC research. The core team supervised, coordinated and assisted with developing the scope of the project and the key clinical questions, nominating the expert panel and drafting the manuscript.
Literature review teamLed by an experienced literature review consultant and the assistance of an expert in methodology; the literature review was conducted based on the specific research questions identified. The team completed the literature search, data abstraction as well as the quality of evidence rating. The studies were categorized by grades of recommendation7,8 and strength of evidence according to Oxford Centre for Evidence-based Medicine (CEBM) system.8
Expert panelThe core leadership team nominated 11 participants. The criteria for their selection included: have professional knowledge and experience in the field of nailfold capillaroscopy as well as active participation in scientific research. The expert panel assisted with developing the scope of the project and refining the key clinical questions. The statements were sent to the expert panel for voting on the recommendations.
Data sources and search strategiesLiterature search strategies were developed for PubMed, Embase, and Cochrane Library databases to identify randomized clinical trials evaluating the nailfold capillaroscopy, its standardization and reporting for the assessment of microcirculation. The search strategies were designed to be broad to have high sensitivity for identifying relevant literature and included search terms for nailfold capillaroscopy, standardization and reporting randomized clinical trials. The literature searches were carried out on January 24, 2022, for PubMed and Cochrane Library databases, and on January 31, 2022, for Embase. Additional relevant studies were retrieved by reviewing the reference lists of studies identified with the database search strategies that met the pre-set inclusion criteria.
Study selectionRelevant studies were selected by applying inclusion and exclusion criteria to the literature retrieved with the search strategies.
Inclusion criteriaArticles included were systematic reviews, randomized controlled trials (RCTs), uncontrolled trials, observational studies including cohort, case–control and cross-sectional studies, or those where economic evaluation was made.
Exclusion criteriaEditorials, commentaries, conference abstracts and non-evidence-based narrative/personal reviews, manuscripts lacking English version, were excluded.
Delphi processDelphi technique was adopted to develop core set domains for reporting nailfold capillaroscopy in both clinical practice as well as clinical research.9,10 The Delphi process was conducted through online questionnaires. Each Delphi round was followed by discussion, amendments or addition of items, then repeated anonymous voting.
Voting processLive online delivered voting was carried out in rounds that are strictly time limited. All members of the task force were invited to participate and are pre-informed of the opening and closure times of each round of votes. Unique access links were sent out, and votes were gathered and processed. After each voting, domains were revised based on feedback from the expert group, together with further critical review of the available literature. Additional/amended domains were added. Only the members of the task force had the right to vote on the domains.
RatingRound 1: Nine response categories are set per each item ranging between 1 and 9 with 1 indicative of ‘complete disagreement’ and 9 indicating ‘complete agreement’. Rankings of 7–9 indicate domains of critical importance, rankings of 4–6 indicate domains that are important but not critical, and rankings of 1–3 indicate domains of low importance. In the first e-Delphi round, it was open for the participants to propose additional domains. Round 2: three responses “in, out or undecided”. All domains were allowed for the entry of comments which were reviewed by the scientific committee. In all the votes’ rounds, the members were urged to leave comments. This enabled the panel to identify an instance of misinterpretation of the domain and invalidate the vote on that item.
Consensus processThe structured Delphi approach ensures that the opinions of participants are equally considered.11 The first Delphi round included one item for each candidate domain with its subdomains. Round 2, aimed to reach preliminary consensus “in” or “out” for domains. It included all items that were rated “of critical importance” (rated in the range of 7–9) by at least 80% of the participants as well as any new domains proposed in round 1. Three response categories per item: “include”, “undecided” or “do not include”. Round 3 might be needed, to reach preliminary consensus “in” or “out” for domains that did not reach preliminary consensus in round 2. Three response categories per item “include”, “undecided”, “do not include”.12 The definitions we used for the consensus of the core areas and domains were summarized in Table 1.
The definitions for the consensus of the core areas and domains.
| Core area | Definition |
|---|---|
| Capillary density | Number of capillaries/1mm. |
| Capillary length | Distance between the capillary apex and the point where the capillary loop is no longer visible. |
| Capillary diameter | Width of the arterial (afferent), apical, venous (efferent) loop (especially apical loop). |
| Giant capillary | A homogeneously (very) enlarged capillary, with a diameter of >50mm. |
| Morphology | The shape of each individual capillary. |
| Blood flow | Regular erythrocytes column, slowed down. |
| Ghost capillary | A capillary that slips in and out of the field of view (during live imaging) because it is only intermittently perfused. |
| Avascular area | Section of the nailfold where no capillaries can be seen. It can sometimes be difficult to decide whether this is ‘true’ avascularity or due to difficulties in visualizing (sections of) the distal row. When using a contact probe, a section of the nailfold can appear avascular if too much pressure is applied. |
| Haemorrhage | Dark areas of hemosiderin on the nailfold capillary bed due to the capillary wall rupture. |
| Angiogenesis | Abnormal shapes (other shapes than hairpin, tortuous, or crossing). |
| Pericapillary oedema | Pericapillary increase of interstitial fluid. |
Definition of consensus was established before initiating the online Delphi procedure and data analysis. The core team reviewed and discussed the consensus criteria and the criteria for excluding domains from consideration in subsequent rounds. Consensus definition were set as: consensus ‘in’: rated ‘do not include’ by <30% of panellists, consensus ‘out’: rated ‘include’ by <30 of panellists, no consensus: rated ‘include’ by at least 30% and rated ‘exclude’ by at least 30%.
Chronogram of Delphi roundsThe first round took place between 13th and 17th May 2022 (5 days). The first-round outcomes were revised in view of the comments and included in the second round. The second round took place between 1st and 10th Jun 2022 (11 days). The third round deemed unnecessary as consensus was achieved by the end of the second round.
Ethics and consentThis study was performed in accordance with the Helsinki Declaration. The “Clinical, Evidence-based, Guidelines (CEG)” initiative protocol was approved the local ethical committee: ethical approval code: 34842/8/21, ethical board Tanta University. All the participants were kept anonymous, in compliance with data protection regulations.
ResultsContent analysis of the literatureThe literature review included 331 studies that discussed report recommendations, definitions, standards, and techniques for quantifying NFC results. Fig. 1 depicts the systematic review research strategy adopted in this work.
Delphi roundsThis was based on an online survey
- -
The first round of the electronic survey included core items identified in the literature review together with their candidate domains and subdomains. The participants identified seven subdomains to be added: two items under Raynaud's phenomenon core area (number of attacks during the week, number of finger ulcers), 2-items under procedure (number of fingers examined and date of the first examination), 1-item under medical status (comorbidities), 1-item under medical status (medications), and 1-item under findings (subpapillary plexus). The final list of the core areas and domains/subdomains are shown in Fig. 2. The response rate in this round was 100% (11/11). Table 2 shows the results of this round which revealed that on 81.8% of the topics, there was agreement on the key NFC Core set domains (i.e., 75% of respondents strongly agreed or agreed).
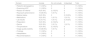
Table 2.Delphi round 1 results: core domains set of nailfold capillaroscopy (NFC) report.
Domain Mean rate±SD % of agreement Level of agreement Core area: patient's demographics 8.18±1.4 81.8 H Core area: examining health care professionals 8.18±1.6 81.8 H Core area: reason for referral 8.18±1.5 81.8 H Core area: Raynaud's phenomenon 8.18±1.4 90.9 H Core area: medical status 8.63±1.3 90.9 H Core area: medications 8.63±1.2 90.9 H Core area: lab results: ANA/ENA 8.63±1.2 90.9 H Core area: preparation 8.27±1.4 81.8 H Core area: device 8.63±1.2 90.9 H Core area: the procedure 8.82±0.6 100 H Core area: image quality 8.63±0.6 100 H Core area: findings 8.8±0.4 100 H Core area: interpretation 8.72±0.7 100 H Core area: recommendations 8.63±0.8 100 H - -
The second round was based on the first round's results and the response rate in this round was 100% (11/11). Outcomes revealed that a consensus has been achieved on the “in” or “out” core areas and domains. 81.8–100% of respondents agreed the key NFC Core set domains to be included. Table 3 shows the results of this round outcomes.
Table 3.Delphi round 2 results: core domains set for nailfold capillaroscopy reporting.
Domain Include Do not include Undecided Total • Patient's demographics 11 (100%) 0 0 11 (100%) • Examining HCP 11 (100%) 0 0 11 (100%) • Reason for referral 9 (81.8%) 2 (18.2%) 0 11 (100%) • Raynaud's phenomenon 10 (90.9%) 1 (9.1%) 0 11 (100%) • Medical status 9 (81.8%) 0 2 (18.2%) 11 (100%) • Medications 9 (81.8%) 1 (9.1%) 1 (9.1%) 11 (100%) • Lab results 8 (72.7%) 1 (9.1%) 2 (18.2%) 11 (100%) • Preparation 9 (81.8%) 2 (18.2%) 0 11 (100%) • Device 9 (81.8%) 1 (9.1%) 1 (9.1%) 11 (100%) • The procedure 9 (81.8%) 2 (18.2%) 0 11 (100%) • Image quality:visibility 10 (90.9%) 1 (9.1%) 0 11 (100%) • Findings 11 (100%) 0 0 11 (100%) • Interpretation 11 (100%) 0 0 11 (100%) • Recommendations 11 (100%) 0 0 11 (100%)

The Delphi form was sent to expert panel (n=11), who participated in the two rounds. Respondents were five internationals, with participation of two Italian (18.2%) and two German (18.2%) and one from UK (9.1%) experts, whereas six national experts were gathered from different governorates and health centres across Egypt: Cairo University (9.1%), Ain Shams University (9.1%), Tanta University (9.1%), Fayoum University (9.1%), Assiut University (9.1%), and National Research Centre (9.1%).
Reporting templateBased on the outcomes of this work, a final reporting template of NFC for use in standard clinical practice and reached has been set up. The reporting template is shown in Fig. 3.
Discussion
The NFC outcomes not only have a diagnostic value, but also have a positive predictive role for the development of specific spectrum disorders. Therefore, a detailed and analytical documentation of the nailfold capillaroscopy findings can be useful to ensure attaining a reproducibly quantitative as well as qualitative recording of the various NFC parameters. So far there is no standard model for NFC reporting. The current study aimed to bring objectivity and achieve consensus about outcome domains to be included in a model of nailfold capillaroscopy report. Also, to ensure that the level of the details included in the report meet the expected standards for both clinical practice as well as clinical research. Online Delphi procedure was adopted with the help of international expert panel to reach a consensus about the core items, domains as well as subdomains for NFC reporting.
Bearing in mind the fact that NFC is a highly operator-dependent imaging tool, earlier attempts to set up standards for reporting the NFC findings highlighted the importance of the matter, but the outcomes of these studies revealed that there is still work remain to be done. Ingegnoli et al.,13 carried out a study to propose a pragmatic reporting checklist for NFC. The study produced a checklist on standardization of reporting capillaroscopy derived from an international consensus. Three overarching areas for reporting NVC were identified. These included patient preparation before NFC, device description and examination details. However, the study concluded that the available evidence is insufficient to make definitive recommendations. The study recommended a further step towards standardization and development of a future ‘NFC core set’. In another study, the Pan-American League of Associations for Rheumatology (PANLAR) capillaroscopy study group published a consensus for the format and content of the nailfold capillaroscopy report in rheumatology.14 Forty-six recommendations for the capillaroscopy report in rheumatology reached a consensus. They were stratified over six sections: patient's data, Raynaud's phenomenon, visibility, NFC examination, diagnosis, suggestion, and imaging. However, the study was based on a comparison of the expert's opinion, in the absence of a strong background of evidence, and it did not suggest a standard reporting format, highlighting a gap in the literature that need to be addressed. Results of this work identified 14 core areas (included in details in Fig. 2). This significant increase in the number of the core items reflects the main objective of this work that is development of NVC core set, which was meant to provide a relevant step forward towards NFC reporting standardization. The developed report template offers detailed specifications of the contents of the NFC report in clinical practice/scientific research, which should encompass specific information that is useful in describing the variable pathologic findings and provide reproducible and measurable information to the examining clinician.
Given its increasing use by a variety of physicians in different centres all over the world, the technique standardization published by the EULAR Study Group on Microcirculation in Rheumatic Diseases,15 regarding image acquisition and analysis, different techniques, normal and abnormal capillaroscopic characteristics and their meaning, scoring systems and reliability of image acquisition and interpretation, has paved the way for producing the reporting standardization too. Though these standards focussed on the technique and defining the capillaroscopic characteristics, it facilitated the concept of having a similar approach for reporting standards. Analysis of this study results revealed that the experts reached a consensus in both rounds on the core items to be reported in the format with some amendments. This reflects the relevance and clarity of the items included in the suggest report core items. In the meantime, the level of consensus agreement, is expected to help to harmonize and smooth NFC reporting and to overcome the personal preferences in documenting the NFC outcomes. Previously published general commendations on the accurate reporting of imaging investigations determined that a ‘good’ report of medical imaging should be designated by the eight Cs: clarity, correctness, confidence, concision, completeness, consistency, communication and consultation.16 The domains identified in this study based on the available evidence derived from the systematic review as well as their terminology were set to meet these ‘good’ report recommendationsIn conclusion, the adoption of a shared form of reporting NFC findings could be a relevant step towards NFC standardization. Considering that several factors may affect the NFC findings, this would defer the calls that NFC report should focus on defining capillaroscopic characteristics to be evaluated (density, dimension, abnormal shape and haemorrhages), but also to include other demographic and methodological standardization applicable for both day to day practice and clinical research. A Delphi survey was carried out including an international expert panel. The majority of the domains identified in the literature and the draft core set were identified by the participants to be important and valid. All domains met the 80% voting threshold set in this work. The work proposed an NFC recording template.
Standardization of nailfold capillaroscopy examination for the assessment of patients with Raynaud's phenomenon and systemic sclerosis has been recently published by the Study Group on Microcirculation in Rheumatic Diseases (EULAR SG/MC RD group).
What this study addsBuilding up the expert consensus from the EULAR SG MC group, it was recognized that the available evidence is insufficient to make definitive recommendations for nailfold capillaroscopy reporting. A further step is required towards standardization, and development of core set areas and domains for a future Nailfold capillaroscopy report that is fit for use in both clinical practice as well as research. This study fills this gap.
How this study might affect research, practice or policyThe current study aimed to bring objectivity and achieve consensus about outcome domains to be included in a model of nailfold capillaroscopy report. Also, to ensure that the level of the details included in the report meet the expected standards for both clinical practice as well as clinical research.
This study was performed in accordance with the Helsinki Declaration. The “Clinical, Evidence-based, Guidelines (CEG)” initiative protocol was approved the local ethical committee: ethical approval code: 34842/8/21, ethical board Tanta University. All the participants were kept anonymous, in compliance with data protection regulations.
Authors’ contributionsAll authors contributed to the study methodology, analysis, and interpretation of the data and outcomes as well as the manuscript writing, reading, and approval of the final version.
FundingThe author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interestNothing to declare.


