

Day hospitalization (DH) is medical or nursing medical attention for patients who require, during the same day, the application of treatments or diagnostic techniques that, without the existence of these centers, would require hospitalization. Day hospitals offer the same services available in a hospital to patients who need chronic treatment or biological therapy for rheumatic diseases, but without the need for their internment. This alternative reduces both the inherent risks of hospitalization to the patient as well as the costs of health assistance associated to treatment and hospitalization.1
The motive of this letter is to describe a series of recommendations used to unify Rheumatology Day Hospitals of the Comunidad Valenciana. Currently, the scenario in which the Rheumatology Day Hospitals of the Comunidad Valenciana (Spain) is one of absence of legislation and rules that regulate the activities performed there or that establish a model of reference to which every hospital must adapt. This fact has generated an elevated variability between different DH in this community, analyzed by Román et al.2
A meeting of 12 rheumatologists and one nurse was organized in Valencia, representing 11 hospitals in the Comunidad Valenciana (in Alicante, Hospital Clínico de San Juan, Hospital General de Elda, Hospital General Universitario de Alicante, Hospital de la Marina Baixa de Villajoyosa, Hospital General Universitario de Elche; in Castellón, Hospital General de Castellón, and in Valencia, Hospital Infantil La Fe, Hospital Universitario La Fe, Hospital Universitario Dr. Peset, Hospital General Universitario de Valencia and the Hospital Clínico Universitario de Valencia) in order to collect proposals for a new DH model, moderated by structured brainstorming.3 From these proposals and the analysis of the current models deficiencies,2 a work frame for proposing recommendations to improve and unify the current DH model of the Comunidad Valenciana, as other documents or specialties recommend on a national level.4,5
There are established recommendations centered on resources (defining needs and competences of the rheumatologist, pharmacist and nursing staff), procedures (such as protocols, questionnaires, schedules and DH circuits, integral attention and telephone consultations) as well as quality-related aspects that include the rheumatologist in the DH management process.
We recommend adapting both material and human resources, anticipating an increase in patients receiving treatment for rheumatic diseases. Acting protocols should be developed for all DH processes (allowing for a better control of those patients treated in DH and a better functioning of the center6), elaborate satisfaction and quality of life questionnaires, improve the centers circuits, increase patient attention hours, perform integral attention, etc. To improve quality-related aspects and the service offered to patients, we recommend integrating the rheumatologist in the processes of the Day Hospital. An implantation plan for the recommendations and the establishment of recommendations and the establishment of indicators allow the evaluation of the improvements introduced.
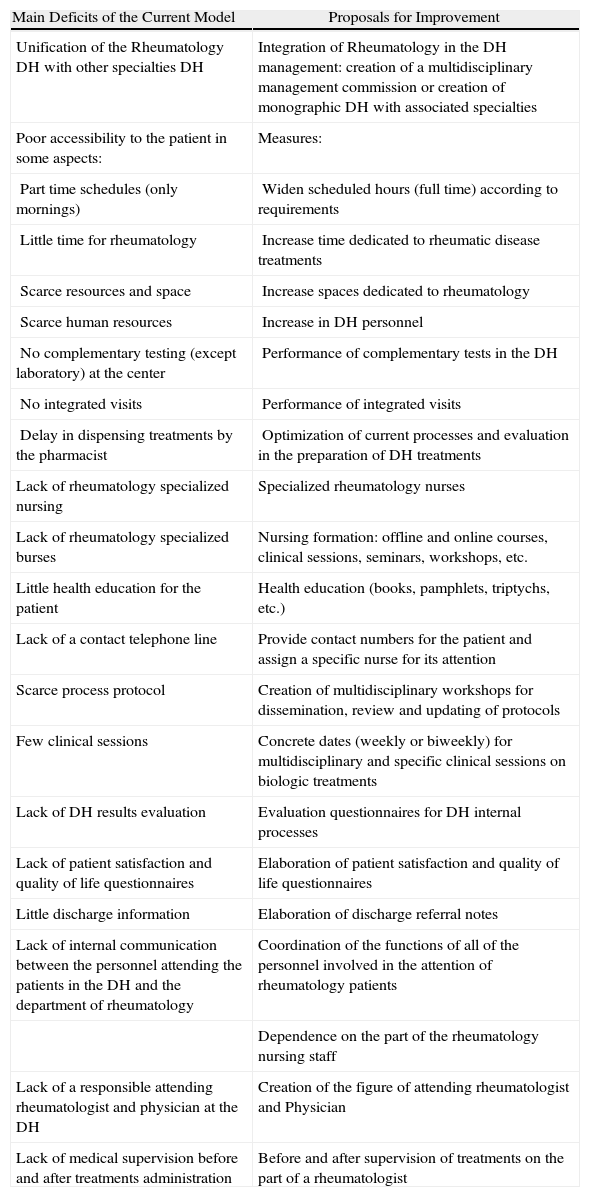
The main deficiencies of the current model and proposals for improvement are summarized in Table 1.
Main Deficits in the Current Valencia Rheumatology HD Model and Proposals for Improvement.
| Main Deficits of the Current Model | Proposals for Improvement |
| Unification of the Rheumatology DH with other specialties DH | Integration of Rheumatology in the DH management: creation of a multidisciplinary management commission or creation of monographic DH with associated specialties |
| Poor accessibility to the patient in some aspects: | Measures: |
| Part time schedules (only mornings) | Widen scheduled hours (full time) according to requirements |
| Little time for rheumatology | Increase time dedicated to rheumatic disease treatments |
| Scarce resources and space | Increase spaces dedicated to rheumatology |
| Scarce human resources | Increase in DH personnel |
| No complementary testing (except laboratory) at the center | Performance of complementary tests in the DH |
| No integrated visits | Performance of integrated visits |
| Delay in dispensing treatments by the pharmacist | Optimization of current processes and evaluation in the preparation of DH treatments |
| Lack of rheumatology specialized nursing | Specialized rheumatology nurses |
| Lack of rheumatology specialized burses | Nursing formation: offline and online courses, clinical sessions, seminars, workshops, etc. |
| Little health education for the patient | Health education (books, pamphlets, triptychs, etc.) |
| Lack of a contact telephone line | Provide contact numbers for the patient and assign a specific nurse for its attention |
| Scarce process protocol | Creation of multidisciplinary workshops for dissemination, review and updating of protocols |
| Few clinical sessions | Concrete dates (weekly or biweekly) for multidisciplinary and specific clinical sessions on biologic treatments |
| Lack of DH results evaluation | Evaluation questionnaires for DH internal processes |
| Lack of patient satisfaction and quality of life questionnaires | Elaboration of patient satisfaction and quality of life questionnaires |
| Little discharge information | Elaboration of discharge referral notes |
| Lack of internal communication between the personnel attending the patients in the DH and the department of rheumatology | Coordination of the functions of all of the personnel involved in the attention of rheumatology patients |
| Dependence on the part of the rheumatology nursing staff | |
| Lack of a responsible attending rheumatologist and physician at the DH | Creation of the figure of attending rheumatologist and Physician |
| Lack of medical supervision before and after treatments administration | Before and after supervision of treatments on the part of a rheumatologist |
We believe it is relevant to consider these recommendations, because other studies7 suggest the importance of evaluating the function of the DH to plan strategies that permit the increasing use of these centers.
Finally, this study only shows those measures for the DH of the Comunidad Valenciana but we believe that these measures are applicable in DH in all of Spain (with prior studies to determine the situation of the Spanish DH and then adapt the measures proposed in this study).
Conflict of InterestThe study was carried out with the support of an unrestricted grant provided by Roche Farma, S.A.
We thank Andreu Covas Estruga and Verónica Albert Sánchez, of Gestió Organització Comunicació, S.A., for their support in the conduction of the methodology used for the elaboration of the study.
Miguel Belmonte Serrano, Francisco Javier Navarro Blasco, Inmaculada Calvo Penadés, Emma Beltrán Catalán, Esteban Salas Heredia, Paloma Vela Casasempere, Jenny De la Torre, Vega Jovani Casano, Juan José García Borrás and Juan Ramón Corts Giner.
En el anexo se relacionan los integrantes del Grupo para el estudio de los hospitales de día de reumatología de la Sociedad Valenciana de Reumatología.
Please cite this article as: Román Ivorra JA, et al. Implantación de un modelo de hospital de día: propuesta de medidas que garanticen las necesidades específicas de los servicios de reumatología de la Comunidad Valenciana (España). Reumatol Clin. 2011;7(6):421–22.


