
Gluteal pain is a frequent cause of medical attention in the daily clinical practice. It can be caused by multiple pathologies, being ischiofemoral impingement syndrome among those included in its differential diagnosis. Encompassed within the deep gluteal syndromes, this entity occurs as a consequence of the entrapment of the neuromuscular structures between the lesser femoral trochanter and the ischial tuberosity, causing pain in the root of the lower limb, with irradiation towards the thigh or the gluteal region and poor tolerance to deambulation and sedestation. The magnetic resonance imaging of the hip is fundamental for its diagnosis, and its management consists on medical treatment at onset. Despite not being a frequent diagnosis in the clinical practice in Rheumatology, keeping it in mind helps improving its prognosis by establishing an early and adequate treatment.
El dolor glúteo es un motivo frecuente de consulta médica en la práctica clínica diaria. Las causas son muy variadas, pudiendo encontrar entre aquellas que forman parte de su diagnóstico diferencial el síndrome de pinzamiento isquiofemoral. Éste, incluido actualmente dentro de los síndromes de glúteo profundo, es consecuencia del atrapamiento de las estructuras neuromusculares englobadas entre el trocánter menor y la tuberosidad isquiática, lo que ocasiona un cuadro de dolor en la raíz del miembro inferior, con irradiación hacia el muslo o hacia región glútea, y mala tolerancia a la deambulación y a la sedestación. La prueba diagnóstica fundamental es la resonancia magnética de cadera, y su manejo suele ser médico inicialmente. A pesar de no ser una entidad frecuente en las consultas de Reumatología, tener esta patología en mente ayuda a mejorar su pronóstico, al poder ofrecer un tratamiento adecuado y precoz.
Gluteal pain is a frequent reason for surgery visits, and its differential diagnosis is broad, due to the varied aetiology that can cause it. It can be due to either mechanical or inflammatory causes, whether local or systemic processes,1 and have its origin in the buttock or come from the spine.
One of these causes, which is rarely thought of in clinical symptoms of this type, is ischiofemoral impingement syndrome. This is characterised by the appearance of pain at the posterior and medial level of the root of the lower limb, caused by a reduction in the space between the lesser trochanter and the ischial tuberosity, resulting in impingement of nearby structures.1
Clinical observationWe present a series of 5 clinical cases of ischiofemoral impingement syndrome diagnosed in our hospital. Within our series, 100% of the patients were women, with a mean age of 57.8years. All of them had bilateral ischiofemoral impingement, although only 40% of the cases had associated bilateral symptoms. A total of 80% had another associated musculoskeletal pathology, the most frequent being chronic low back pain, which appeared in 40% of those cases. The mean time of evolution of the symptoms presented was 2.3years. The management of all patients was medical, without resorting to surgical intervention, and only 20% of the patients achieved total resolution of the symptoms. The remaining 80% only achieved partial improvement in their symptoms.
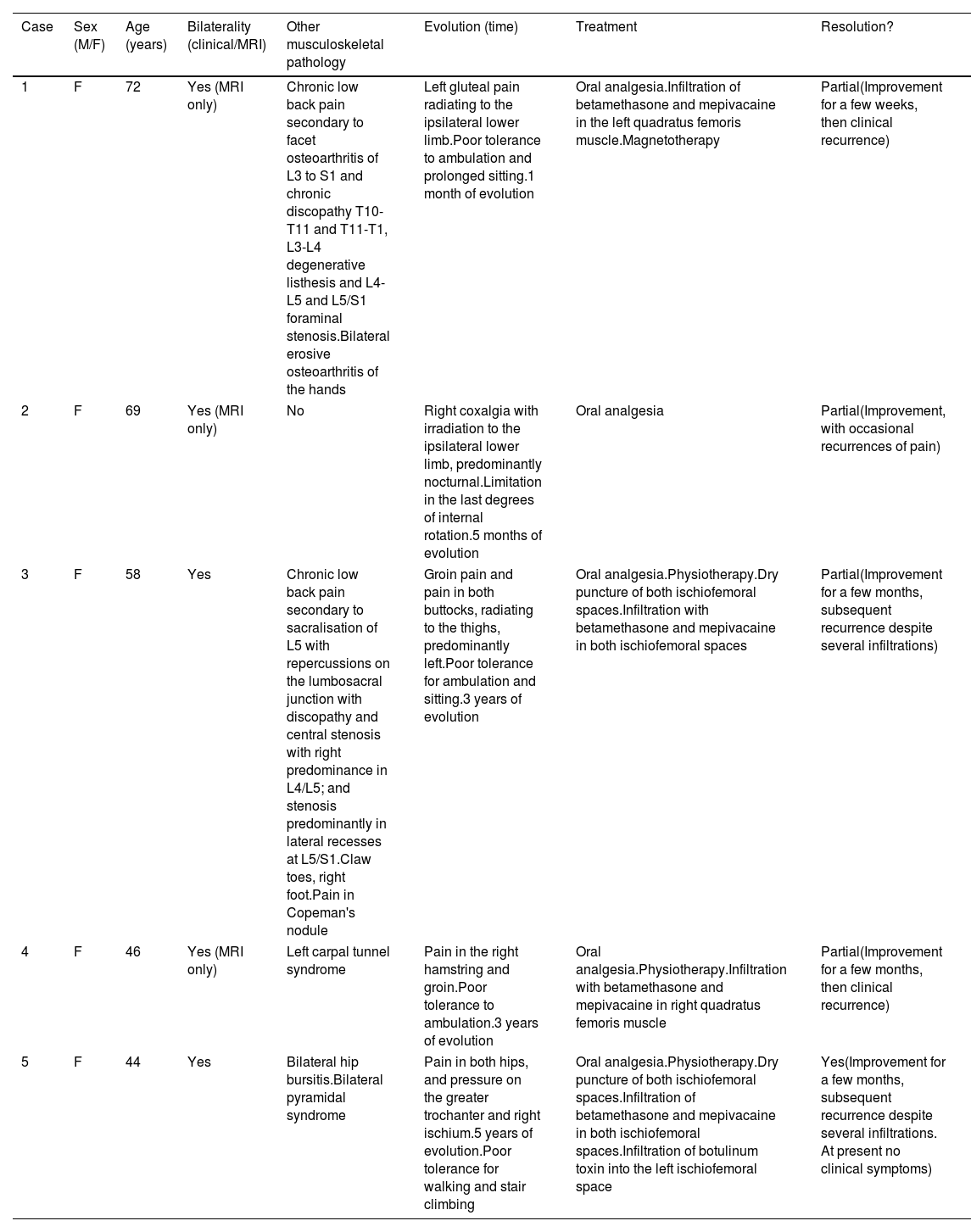
Table 1 shows the characteristics of the 5 clinical cases of ischiofemoral impingement syndrome.
Description of the clinical cases of ischiofemoral impingement syndrome diagnosed in our hospital. In the table we find characteristics of sex, age in years, bilaterality of symptoms, presence of other concomitant rheumatological diagnoses, treatments used in the management of ischiofemoral impingement syndrome, clinical evolution and resolution of the symptoms after treatment.
| Case | Sex (M/F) | Age (years) | Bilaterality (clinical/MRI) | Other musculoskeletal pathology | Evolution (time) | Treatment | Resolution? |
|---|---|---|---|---|---|---|---|
| 1 | F | 72 | Yes (MRI only) | Chronic low back pain secondary to facet osteoarthritis of L3 to S1 and chronic discopathy T10-T11 and T11-T1, L3-L4 degenerative listhesis and L4-L5 and L5/S1 foraminal stenosis.Bilateral erosive osteoarthritis of the hands | Left gluteal pain radiating to the ipsilateral lower limb.Poor tolerance to ambulation and prolonged sitting.1 month of evolution | Oral analgesia.Infiltration of betamethasone and mepivacaine in the left quadratus femoris muscle.Magnetotherapy | Partial(Improvement for a few weeks, then clinical recurrence) |
| 2 | F | 69 | Yes (MRI only) | No | Right coxalgia with irradiation to the ipsilateral lower limb, predominantly nocturnal.Limitation in the last degrees of internal rotation.5 months of evolution | Oral analgesia | Partial(Improvement, with occasional recurrences of pain) |
| 3 | F | 58 | Yes | Chronic low back pain secondary to sacralisation of L5 with repercussions on the lumbosacral junction with discopathy and central stenosis with right predominance in L4/L5; and stenosis predominantly in lateral recesses at L5/S1.Claw toes, right foot.Pain in Copeman's nodule | Groin pain and pain in both buttocks, radiating to the thighs, predominantly left.Poor tolerance for ambulation and sitting.3 years of evolution | Oral analgesia.Physiotherapy.Dry puncture of both ischiofemoral spaces.Infiltration with betamethasone and mepivacaine in both ischiofemoral spaces | Partial(Improvement for a few months, subsequent recurrence despite several infiltrations) |
| 4 | F | 46 | Yes (MRI only) | Left carpal tunnel syndrome | Pain in the right hamstring and groin.Poor tolerance to ambulation.3 years of evolution | Oral analgesia.Physiotherapy.Infiltration with betamethasone and mepivacaine in right quadratus femoris muscle | Partial(Improvement for a few months, then clinical recurrence) |
| 5 | F | 44 | Yes | Bilateral hip bursitis.Bilateral pyramidal syndrome | Pain in both hips, and pressure on the greater trochanter and right ischium.5 years of evolution.Poor tolerance for walking and stair climbing | Oral analgesia.Physiotherapy.Dry puncture of both ischiofemoral spaces.Infiltration of betamethasone and mepivacaine in both ischiofemoral spaces.Infiltration of botulinum toxin into the left ischiofemoral space | Yes(Improvement for a few months, subsequent recurrence despite several infiltrations. At present no clinical symptoms) |
F: Female; M: Male; MRI: Magnetic Resonance Imaging.
Ischiofemoral impingement syndrome is a rare diagnosis among rheumatologists. After reviewing the literature published over the last 10years on this topic, only two studies have been published in specialised rheumatology journals.
This is a syndrome caused by friction of different anatomical structures, as a result of the decrease in the ischiofemoral space (bordered by the lesser trochanter and the ischial tuberosity), one of the possible impingement points in the bony pelvis.2 This generates excessive or abnormal friction between these structures, causing intermittent entrapment or impingement of the quadratus femoris muscle, leading to oedema, atrophy or sometimes even rupture of the muscle,3,4 which leads to clinical symptoms.
Its ethology and pathophysiology are not fully understood. It was initially described by Johnson in 1977 in patients with persistent coxalgia after hip replacement surgery and was later evidenced in patients who have suffered an intertrochanteric fracture after corrective pelvic osteotomy, or in patients with osteoarthritis in the hip.5,6 However, it has been seen that the majority of cases have a primary or idiopathic cause.7 Bilateral involvement may occur in 25% of cases.2 In addition, cases have been described of patients with reduced ischiofemoral space without clinical symptoms, or patients with bilateral impingement who present symptoms in only one limb.7
Its prevalence is unknown, and only series with few published cases are available. As in our case series, the majority of patients are women, which may be related to the anatomical arrangement of the female pelvis, which has more prominent ischial tuberosities.2 It has also been seen in patients with a weakness in the abductor muscles (causing dynamic impingement of the space), or with lower limb dysmetria.1
Clinically, patients present with posteromedial pain at the root of the lower limb, frequently associated with radiation of pain to the thigh or buttocks.8 Although it is true that some authors describe the clinical symptoms as hip pain,2,4,5 it is common for patients to refer to it as gluteal pain, and it is currently included in the literature within the syndromes of the deep glutei.8–10 The pain can worsen with external rotation, adduction and extension of the hip. This limits hip movement, with walking and sitting being especially poorly tolerated, as we observed in some of our cases included in the series. As a result, patients frequently seek an analgesic position.8 Acute symptoms can develop (due to the accumulation of oedema and inflammation in the anatomical structures included) or chronic symptoms (due to the appearance of fibrous tissue that traps the sciatic nerve), evolving over months or even years.8,9
A differential diagnosis should be reached with pathologies that produce similar symptoms, such as psoas tendon rupture, lumbar radiculopathy, hamstring or adductor tendinopathy, or quadratus femoris rupture, as well as the causes of groin pain: bursitis and osteitis of the hip, synphysitis, entrapment of the sciatic nerve or pudendal nerve, among others.2,5,11
When examining these patients, we should be aware of two exploratory manoeuvres that suggest the presence of ischiofemoral impingement:
- •
Ischiofemoral impingement test.10 This manoeuvre is positive when the patient presents pain on extension, external rotation and forced adduction of the hip, improving pain with abduction. With this manoeuvre, it is possible to verify the dynamic space between the ischium and the lesser trochanter3,11,12 and its positivity has even been correlated with the presence of impingement in imaging tests.12
- •
Test of gait with long strides.5 By forcing the patient to take long strides, the pain in the region lateral to the ischial tuberosity is reproduced with the final extension of the hip during walking, with the pain improving when taking shorter steps.
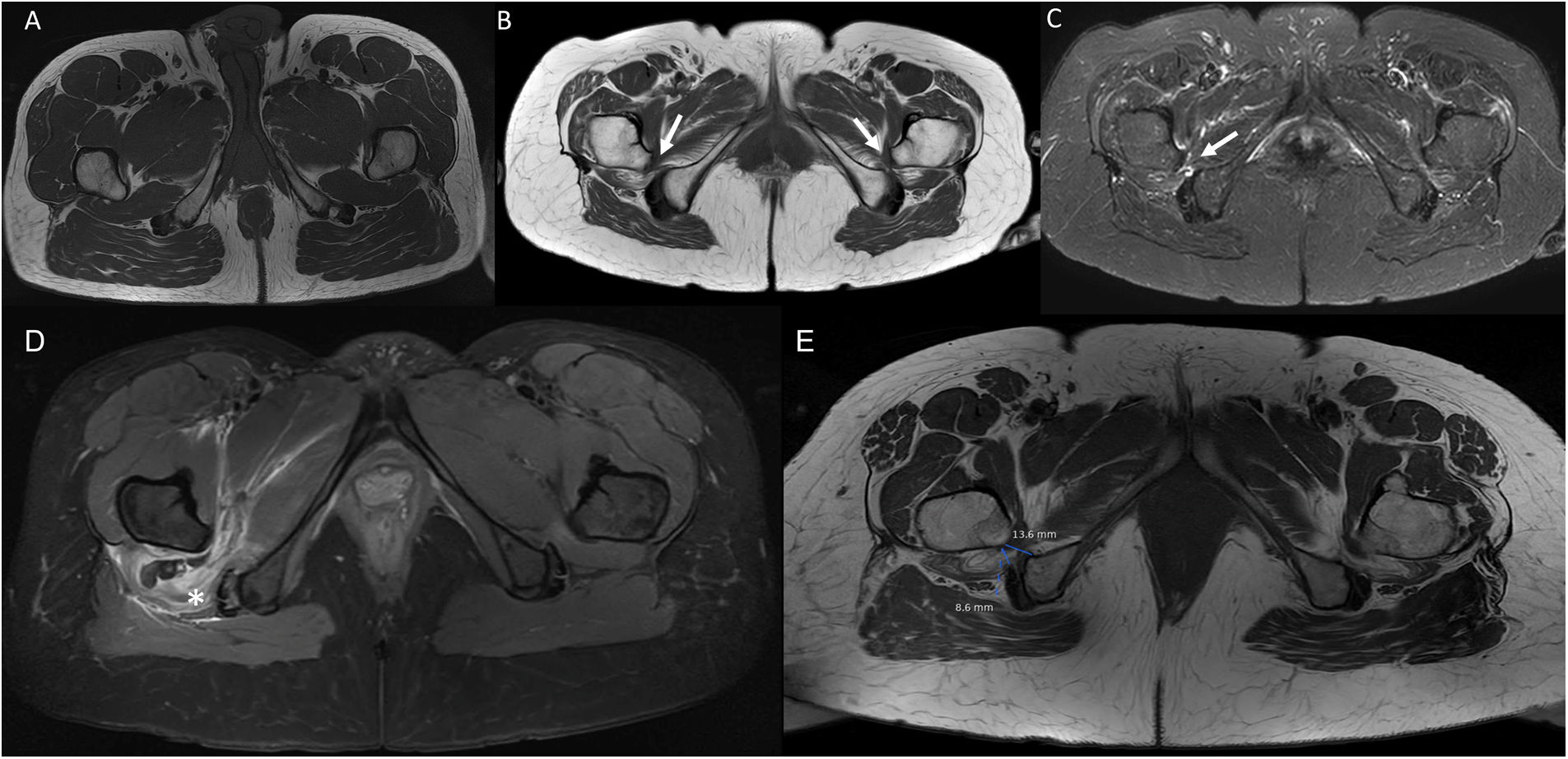
Magnetic resonance imaging (MRI) of the hip is the gold standard test for decreasing the ischiofemoral space (Fig. 1).12 Impingement is considered when the ischiofemoral space is less than 23 (±8) cm, or when the width of the quadratus femoris muscle is less than 12 (±4) cm.5,8 However, there is controversy with the use of these reference values,1,11 given that this space is highly variable depending on the gait cycle and the patient's position during the imaging test, and MRI tends to overestimate its measurement, so the physical examination of the patient is essential in the diagnosis of this pathology. MRI can also detect alteration of the quadratus femoris muscle signal due to oedema or fibre rupture, fat infiltration in cases of chronic impingement, or insertional tendinopathy of the hamstrings or iliopsoas.2,9,11 Another technique that is very useful is dynamic hip ultrasound to corroborate the impingement of the ischiofemoral space with the change in position of the lower limb, as well as to assess whether the patient's symptoms are due to impingement or other causes.11
 and STIR (C) sequences. (A) Image of normal anatomy. (B) Patient number 2 in our series: bilateral decrease in the ischiofemoral space (white arrows). (C) The same patient, where there is also slight oedema in the soft tissues (femoral square) of the right ischiofemoral space and atrophy in both. D) MR image of axial plane. Proton density-enhanced (PD) sequence with fat saturation. Thickening with oedema and haematoma in the right quadratus femoris muscle (*) due to rupture in patient with ischiofemoral space impingement. (E) MRI image in axial plane. T1-weighted sequence. Measurement of the femoral square and ischiofemoral space in patient with impingement.")
Composition of MR images on the axial plane. T1-weighted (A and B) and STIR (C) sequences. (A) Image of normal anatomy. (B) Patient number 2 in our series: bilateral decrease in the ischiofemoral space (white arrows). (C) The same patient, where there is also slight oedema in the soft tissues (femoral square) of the right ischiofemoral space and atrophy in both. D) MR image of axial plane. Proton density-enhanced (PD) sequence with fat saturation. Thickening with oedema and haematoma in the right quadratus femoris muscle (*) due to rupture in patient with ischiofemoral space impingement. (E) MRI image in axial plane. T1-weighted sequence. Measurement of the femoral square and ischiofemoral space in patient with impingement.
In terms of treatment, as we observed in our series, medical management is usually chosen from the outset, indicating relative rest and avoiding activities that reproduce the clinical symptoms. Also indicated is the use of analgesics or anti-inflammatories, injections of both glucocorticoids and local aesthetics - or even botulinum toxin - and physiotherapy with the aim of strengthening the abductors or re-educating the patient to limit the amplitude of the stride when walking.5,7,9 However, some patients tend to have a poor response, so in the case of persistence of clinical symptoms, definitive surgical treatment using different techniques is indicated, including resection or distalisation of the lesser trochanter, ischioplasty or femoral osteotomy.2,5,11
ConclusionAlthough it is not a frequent pathology in our daily clinical practice, rheumatologists must consider ischiofemoral impingement syndrome in patients with radiating gluteal pain, since the prognosis will depend on the rapidity of diagnosis and the correct referral of the patient in order to offer adequate and early treatment.
Conflict of interestThe authors declare that they do not have any type of conflict of interest in the production and publication of this study.


