




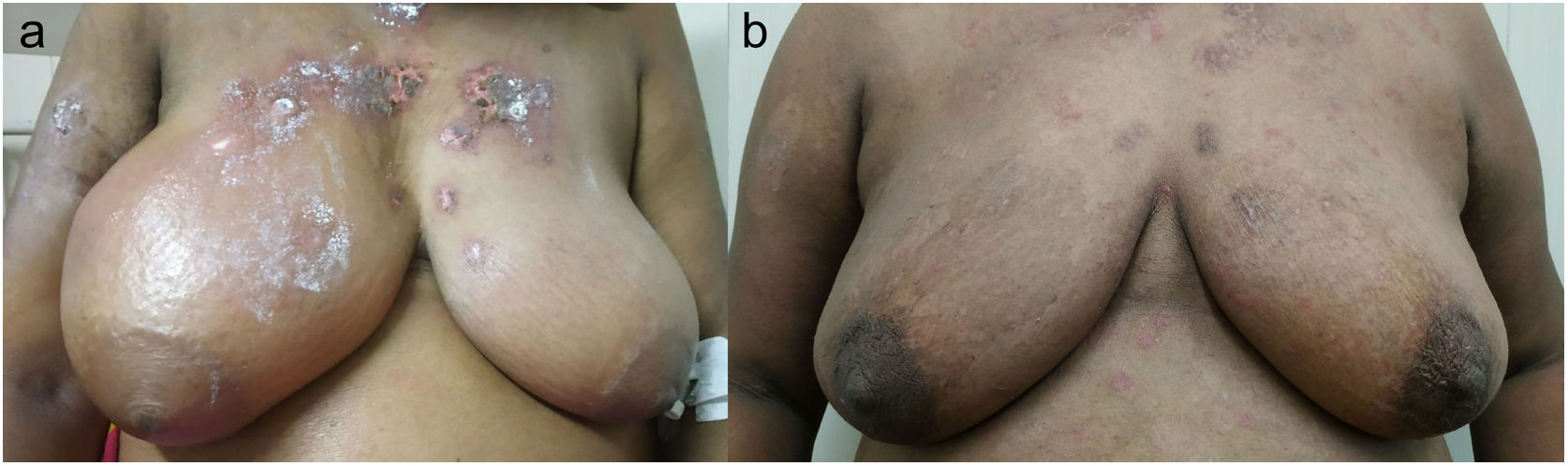
A 45-year-old-woman presented with a non-pruritic, maculopapular rash over her face, chest, and back for four months and a gradually progressive, painful swelling of the right breast and right upper limb for the last two months. There was no fever, loss of weight or appetite, or B-symptoms. On examination, an extensive rash was present on the face, chest, and back with discoid lesions over the ears. The right breast and upper limb were erythematous, swollen, indurated, and tender with peau d’orange changes (Fig. 1A). There was no axillary or cervical lymphadenopathy. Her hemogram was unremarkable and other investigations revealed positive anti-nuclear antibody (ANA), low complements, and SS-A, Ro-52, and Ribosomal P positivity on ANA blot. Ultrasound revealed diffuse dermal edema, patent axillary and subclavian veins and no masses. Skin biopsy from the rash showed interface dermatitis. Because of a typical rash, positive ANA, and interface dermatitis on biopsy, oral prednisolone, and hydroxychloroquine was started for lupus-related mastitis and acute cutaneous lupus erythematosus rash. There was rapid improvement in the breast and arm swelling over four weeks (Fig. 1B).
Lupus Mastitis (LM) is lupus panniculitis involving the mammary gland. It is seen at a mean age of 40 years in patients with pre-established lupus and is associated with discoid lupus erythematosus. It is rare with less than 50 documented cases.1 It presents as subcutaneous mass (clinically and radiographically) with skin changes and should be differentiated from infection and malignancy, especially inflammatory breast carcinoma. Irregular, asymmetric masses, coarse calcifications (suggesting fat necrosis), and fibrosis are seen on imaging. Hyaline fat necrosis is the typical histological hallmark of LM. Periseptal/lobular panniculitis, lobular lymphocytic infiltrates and microcalcifications are also seen.1 Bilateral lesions should prompt a workup for non-Hodgkin's lymphoma.2 Breast abscess and diabetic mastopathy should be considered in appropriate clinical situations. Idiopathic Granulomatous Mastitis (IGM) is a close differential diagnosis with a possible autoimmune etiology but it rarely has calcifications on imaging and biopsy reveals non-caseating granulomas.3 Other connective tissue diseases causing mastitis are vasculitides (granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, giant cell arteritis, Behcet's disease, polyarteritis nodosa), granulomatous diseases (sarcoidosis, Crohn's disease), IgG4 related disease and Sjogren's syndrome. These can be differentiated by serology and biopsy.4 LM responds well to hydroxychloroquine with or without steroids. Surgery may worsen it, hence an accurate diagnosis is essential.5
Contributor informationRR & SJ: Identified and managed the case, write the manuscript. AC: Identified and managed the case and reviewed the manuscript. AG: Identified the case and reviewed the manuscript.
Patient consentWritten consent has been obtained from the patient for this publication.
Financial disclosures/funding sourcesNone of the authors have any financial disclosure or funding sources.
Conflicts of interestNone of the authors have any conflicts of interest to disclose.


