

Health-related quality of life (HRQoL) is an important indicator of population health and can measure the impact of medical actions. The main objective of this study was to determine the HRQoL of patients with rheumatic diseases (RD) and compare it with that of the general population.
MethodsObservational, cross-sectional, single-center study, with consecutive inclusion of outpatients over 18 years of age seen at a Rheumatology hospital-based outpatient clinic in Madrid. Sociodemographic, clinical variables and HRQoL were recorded. HRQoL was measured with the 5-dimension, 5-level EuroQoL (EQ-5D-5L), which includes the EQ-Index (0–1 scale) and a visual analog scale (VAS, 0–100 scale). A descriptive analysis and a comparison with the HRQoL of the Spanish general population were performed.
Results1144 patients were included, 820 (71.68%) women, with a mean age of 56.1 years (range 18–95), of whom 241 (25.44%) were new patients. In patients with RD, the HRQoL measured with the EQ-Index and with the VAS, was 0.186 and 12 points lower, respectively, than in the general population. The decrease in HRQoL affected the 5 health dimensions, especially “pain/discomfort”, followed by “daily activities” and “mobility”. This reduction in HRQoL was observed in both men and women, and in all age ranges, although it was greater between 18 and 65 years of age. The reduction in HRQoL affected all RD subtypes, especially the “peripheral and axial mechanical pathology” and the “soft tissue pathology” group.
ConclusionsPatients with rheumatic diseases report worse HRQoL when compared to the general population in all dimensions of HRQoL.
La calidad de vida relacionada con la salud (CVRS) se considera un indicador importante para valorar el estado de salud poblacional y medir el impacto de las actuaciones médicas. El principal objetivo de este estudio es conocer la CVRS de los pacientes con enfermedades reumáticas (RD, por sus siglas en inglés) y compararla con la población general.
MétodosEstudio observacional, transversal, unicéntrico, con inclusión consecutiva de pacientes ambulatorios mayores de 18 años atendidos en la consulta hospitalaria de reumatología. Se recogieron variables sociodemográficas, clínicas y CVRS medida con el EuroQoL de 5 dimensiones y 5 niveles (EQ-5D-5L) que incluye el EQ-Índex (escala 0-1) y una escala visual analógica (EVA, escala 0-100). Se realizó un análisis descriptico y una comparación con la población española según la Encuesta Nacional de Salud.
ResultadosSe han incluido 1.144 pacientes, 820 (71,68%) mujeres, con edad media de 56,1 años (rango 18-95), de los que 241 (25,44%) eran pacientes nuevos. En los pacientes con RD, la CVRS medida con el EQ-Index y con la EVA, fue de 0,186 y 12 puntos menor, respectivamente, que en la población general. La CVRS afectó a las 5 dimensiones de salud, especialmente a «dolor/malestar», seguida de «actividades cotidianas» y «movilidad». Esta reducción de la CVRS se mantuvo tanto en varones y mujeres, y en todos los segmentos de edad, aunque fue mayor entre los 18 y 65 años. La reducción de CVRS afectó a todos los subtipos de RD, especialmente a la «Enfermedad mecánica periférica y axial» y al grupo de «Enfermedad de tejidos blandos».
ConclusionesLos pacientes con enfermedades reumáticas declaran peor CVRS en comparación a la población general en todas las dimensiones de la CVRS.
Health systems have the mission of improving the health of the population they serve, which implies improving the survival and quality of life of patients. For this reason, health-related quality of life (HRQoL) is a key indicator to measure health outcomes1 and to describe the health situation in specific populations, including patients with rheumatic diseases (RD).2–4
HRQoL has generated increasing interest in recent years, as indicated by the increase in publications on the subject.5 There is no consensus regarding the definition, but there is agreement on its multidimensional and subjective nature.6 In a stratification pyramid of the different health measurement systems, HRQoL would be at the apex, since it is capable of offering morbidity and mortality data and a vision of the patient in the optimal death-function continuum.5
The 5-dimension EuroQoL (EQ-5D) is one of the most widely used generic measurement instruments in patients with chronic diseases, including patients with RD,7 and has been validated in multiple countries, including Spain.8 The EQ-5D measures five dimensions of health (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). Since the EQ-5D offers a quantitative result of the individual's perception of their health status, it allows comparison of HRQoL between patients, diseases, or with the general population.9 The 5-level EQ-5D (EQ-5D-5L) assesses each dimension with five response levels (1–5) and also has a visual analog scale (VAS) ranging from 0 (worst state of health imaginable) to 100 (best self-perceived state of health). The EQ-Index, calculated with the levels of the dimensions, ranges from 1 (perfect health) to 0 (a state of health equivalent to death).8,9
RD are among the most common chronic diseases, with a high disease burden.10 In Spain, the prevalence of RD is 22.6% in the general population,11 which implies a large use of resources in primary and specialized care. Therapeutic outcome assessments in Rheumatology are usually based on levels of activity measured with disease-specific tools, but different studies show discrepancies between doctors’ perceptions of HRQoL and information referred by the patient.12–14 The European League Against Rheumatism (EULAR) proposes maximizing the HRQoL of patients as the main objective,15 but in usual clinical practice it is not considered a primary health outcome. For these reasons, this project was developed, the objective of which was to describe the HRQoL of patients seen in the Rheumatology Department of the Ramón y Cajal University Hospital (RS-RyCUH) and to compare their HRQoL with that of the general population.
MethodsObservational, cross-sectional study, with data obtained from the medical record (MR) and questionnaires completed by the patient. The study subjects were patients who attended the RS-RyCUH clinic, both as new patients and for follow-up.
Inclusion criteriaAge>18 years, without communication problems and who agreed to participate in the study by signing a written informed consent. The patients were included consecutively.
The case report form (CRF) included sociodemographic variables (civil status, cohabitation, educational level, employment situation, identification of the person who contributed the most income to the household, social class, self-perceived health status, comorbidities, body mass index (BMI), smoking habit, and physical activity) used by the Ministry of Health and the National Statistics Institute (NSI)16,17 in their population health surveys. Likewise, the CRF asked the patients if they had had any other diseases diagnosed by a doctor in the last 12 months, from a list of 32 diseases. To explore alcohol consumption, the AUDIT-C questionnaire18,19 was used. To measure the degree of health literacy, the 16-item European Health Literacy Survey Questionnaire (HLS-EU-Q16) validated in Spain20 was used. The instrument for measuring HRQoL was the EQ-5D-5L, used in the Spanish National Health Survey (ENSE) 2011–2012,16,17,21 which was the last ENSE that measured HRQoL in adults.
Based on the ICD-10 classification of “diseases of the musculoskeletal system and connective tissue”, seven diagnostic categories were established: peripheral and axial mechanical pathology; soft tissue pathology; neuropathies; metabolic pathology; infectious pathology; inflammatory and microcrystalline arthropathies; and vasculitis-connective tissue diseases. Each of these categories was subdivided into their corresponding diagnostic subcategories.22 As some patients could have more than one rheumatic disease, the variables “main diagnosis” and “secondary diagnosis” were created with the same category structure. The diagnosis, in turn, was classified as confirmed or suspected. The doctor filled out a database (DB) with information from the MR.
Sample sizeTo obtain a precision of 3% in the categorical variables, with the assumption of maximum indeterminacy (p=q=0.5), 1056 patients would have been necessary (α=0.05; β=0.8). The mean VAS of the EQ-5D-5L in the ENSE was 77.9 (standard deviation (SD)=18.6).21 If in the RS-RyCUH, the VAS obtained had a variance similar to that obtained in a study carried out in Portugal (mean: 60.7; SD=19.3),23 904 patients would be necessary to find a difference of 2.5 points between the hospital sample and the general population. For these reasons, a sample size with sufficient power and statistical precision of around 1000 patients was considered.
Data collectionThe CRF draft version was tested in a pilot study with 5 patients, after which the final CRF version was prepared in paper format. Trained personnel (auxillary nurses) assisted patients with the CRF when required. The information collected through the CRF and the MR was entered in the DB.
Statistical analysisFor the descriptive analysis, categorical variables were described as proportions (%). To describe the continuous variables, the normality of their distribution was first verified using the Kolmogorov–Smirnov test. For continuous variables with a normal distribution, the mean and SD were used. For continuous variables without a normal distribution, the median and interquartile range (IQR) were used. To fully illustrate the distribution of non-normally distributed continuous variables, the mean and SD were also shown.
HRQoL was described using the categorical and continuous EQ-5D-5L variables. The five categorical variables included the proportion of patients who reported a problem in each of the 5-dimensions of the EQ-5D-5, and the continuous variables were the VAS and the EQ-Index.24
As the VAS and EQ-Index did not have a normal distribution, the study of univariate associations of the VAS and EQ-Index with gender and age groups was performed using the Mann–Whitney U test (two samples), or the Kruskal–Wallis test (more than two samples). Finally, the patients’ HRQoL was compared with the HRQoL of the Spanish adult population according to the ENSE,21 and between the subgroups for which information was available. In this comparison, the t-test was used for two independent samples, since the ENSE data only included the number, mean, and SD.
The contrasts were made with two tails and a p<0.05 was considered a statistically significant association. Data analysis was performed using the SPSS statistical package (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Ethical aspectsThe patient was informed that their responses would be anonymized. The patients who agreed to participate signed the written informed consent and completed the CRF. The anonymized data were included in the DB and were processed with the security measures established in the Data Protection Law.25 The researchers preserved the confidentiality of the data as determined by the Law on Patient Autonomy, Clinical Information and Documentation.26 The research protocol was approved by the Ramón y Cajal University Hospital ethics and clinical research committee (Code 072-20).
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
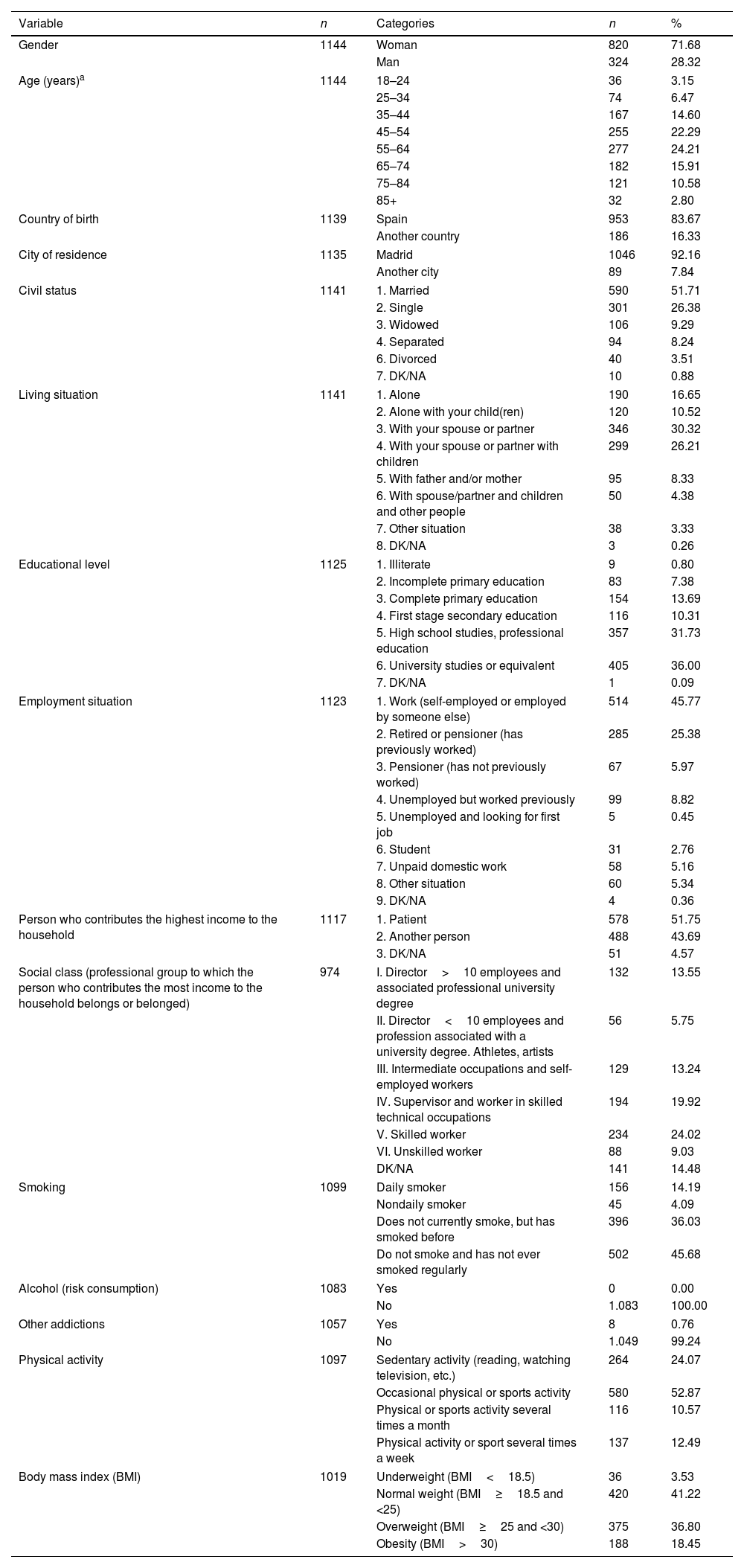
ResultsSociodemographic characteristicsFrom January 2020 to December 2021, 1144 patients were included in the study, with a mean age of 56.10 years, of whom 820 (71.68%) were women. The most frequent civil status was married (51.71%) with a predominance of patients with university or equivalent studies (36.00%). The health literacy questionnaire was completed by 931 patients, of which 34.8% had a problematic or inadequate health literacy level. Regarding employment situation, the group that works for their own account or for others (45.77%) predominated, and in 51.75% of households, the person who contributed the highest income was the patient. The questionnaire on social class (defined according to the professional group to which the person who contributes the most income to the household belongs) was answered by 974 patients, and the majority (24.02%) belonged to class V (qualified worker) (Table 1).
Description of the sample: sociodemographic variables.
| Variable | n | Categories | n | % |
|---|---|---|---|---|
| Gender | 1144 | Woman | 820 | 71.68 |
| Man | 324 | 28.32 | ||
| Age (years)a | 1144 | 18–24 | 36 | 3.15 |
| 25–34 | 74 | 6.47 | ||
| 35–44 | 167 | 14.60 | ||
| 45–54 | 255 | 22.29 | ||
| 55–64 | 277 | 24.21 | ||
| 65–74 | 182 | 15.91 | ||
| 75–84 | 121 | 10.58 | ||
| 85+ | 32 | 2.80 | ||
| Country of birth | 1139 | Spain | 953 | 83.67 |
| Another country | 186 | 16.33 | ||
| City of residence | 1135 | Madrid | 1046 | 92.16 |
| Another city | 89 | 7.84 | ||
| Civil status | 1141 | 1. Married | 590 | 51.71 |
| 2. Single | 301 | 26.38 | ||
| 3. Widowed | 106 | 9.29 | ||
| 4. Separated | 94 | 8.24 | ||
| 6. Divorced | 40 | 3.51 | ||
| 7. DK/NA | 10 | 0.88 | ||
| Living situation | 1141 | 1. Alone | 190 | 16.65 |
| 2. Alone with your child(ren) | 120 | 10.52 | ||
| 3. With your spouse or partner | 346 | 30.32 | ||
| 4. With your spouse or partner with children | 299 | 26.21 | ||
| 5. With father and/or mother | 95 | 8.33 | ||
| 6. With spouse/partner and children and other people | 50 | 4.38 | ||
| 7. Other situation | 38 | 3.33 | ||
| 8. DK/NA | 3 | 0.26 | ||
| Educational level | 1125 | 1. Illiterate | 9 | 0.80 |
| 2. Incomplete primary education | 83 | 7.38 | ||
| 3. Complete primary education | 154 | 13.69 | ||
| 4. First stage secondary education | 116 | 10.31 | ||
| 5. High school studies, professional education | 357 | 31.73 | ||
| 6. University studies or equivalent | 405 | 36.00 | ||
| 7. DK/NA | 1 | 0.09 | ||
| Employment situation | 1123 | 1. Work (self-employed or employed by someone else) | 514 | 45.77 |
| 2. Retired or pensioner (has previously worked) | 285 | 25.38 | ||
| 3. Pensioner (has not previously worked) | 67 | 5.97 | ||
| 4. Unemployed but worked previously | 99 | 8.82 | ||
| 5. Unemployed and looking for first job | 5 | 0.45 | ||
| 6. Student | 31 | 2.76 | ||
| 7. Unpaid domestic work | 58 | 5.16 | ||
| 8. Other situation | 60 | 5.34 | ||
| 9. DK/NA | 4 | 0.36 | ||
| Person who contributes the highest income to the household | 1117 | 1. Patient | 578 | 51.75 |
| 2. Another person | 488 | 43.69 | ||
| 3. DK/NA | 51 | 4.57 | ||
| Social class (professional group to which the person who contributes the most income to the household belongs or belonged) | 974 | I. Director>10 employees and associated professional university degree | 132 | 13.55 |
| II. Director<10 employees and profession associated with a university degree. Athletes, artists | 56 | 5.75 | ||
| III. Intermediate occupations and self-employed workers | 129 | 13.24 | ||
| IV. Supervisor and worker in skilled technical occupations | 194 | 19.92 | ||
| V. Skilled worker | 234 | 24.02 | ||
| VI. Unskilled worker | 88 | 9.03 | ||
| DK/NA | 141 | 14.48 | ||
| Smoking | 1099 | Daily smoker | 156 | 14.19 |
| Nondaily smoker | 45 | 4.09 | ||
| Does not currently smoke, but has smoked before | 396 | 36.03 | ||
| Do not smoke and has not ever smoked regularly | 502 | 45.68 | ||
| Alcohol (risk consumption) | 1083 | Yes | 0 | 0.00 |
| No | 1.083 | 100.00 | ||
| Other addictions | 1057 | Yes | 8 | 0.76 |
| No | 1.049 | 99.24 | ||
| Physical activity | 1097 | Sedentary activity (reading, watching television, etc.) | 264 | 24.07 |
| Occasional physical or sports activity | 580 | 52.87 | ||
| Physical or sports activity several times a month | 116 | 10.57 | ||
| Physical activity or sport several times a week | 137 | 12.49 | ||
| Body mass index (BMI) | 1019 | Underweight (BMI<18.5) | 36 | 3.53 |
| Normal weight (BMI≥18.5 and <25) | 420 | 41.22 | ||
| Overweight (BMI≥25 and <30) | 375 | 36.80 | ||
| Obesity (BMI>30) | 188 | 18.45 | ||
DK/NA: don’t know/no answer.
Regarding lifestyle habits, 14.19% of the patients were smokers and no patients had risky consumption of alcohol. The predominant degree of physical activity was “occasional physical or sports activity” (52.87%), followed by “sedentary activity” (24.07%). The BMI could be calculated in 1019 patients, of whom 36.80% were overweight and 18.45% were obese (Table 1).
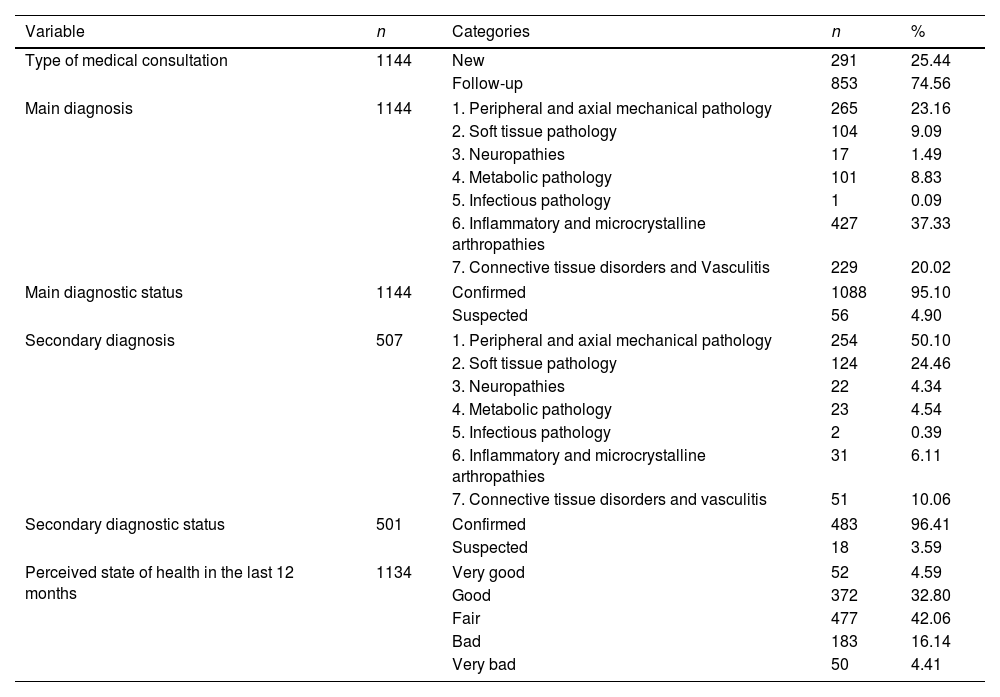
DiagnosisA quarter of the patients attended the consultation for the first time, and the rest went for a follow-up visit. All patients had a primary diagnosis and 507 (44.32%) patients had a secondary diagnosis.
The most frequent main diagnosis was inflammatory and microcrystalline arthropathies (37.33%), followed by peripheral and axial mechanical pathology (23.16%) and connective tissue diseases and vasculitis (20.02%). In 95.1% of the patients, the main diagnosis was confirmed. The most frequent secondary diagnosis was diseases in the peripheral and axial mechanical pathology group (50.1%), followed by the soft tissue pathology group (24.46%); 96.41% of the secondary diagnoses were confirmed (Table 2).
Description of the sample: clinical variables and perceived state of health.
| Variable | n | Categories | n | % |
|---|---|---|---|---|
| Type of medical consultation | 1144 | New | 291 | 25.44 |
| Follow-up | 853 | 74.56 | ||
| Main diagnosis | 1144 | 1. Peripheral and axial mechanical pathology | 265 | 23.16 |
| 2. Soft tissue pathology | 104 | 9.09 | ||
| 3. Neuropathies | 17 | 1.49 | ||
| 4. Metabolic pathology | 101 | 8.83 | ||
| 5. Infectious pathology | 1 | 0.09 | ||
| 6. Inflammatory and microcrystalline arthropathies | 427 | 37.33 | ||
| 7. Connective tissue disorders and Vasculitis | 229 | 20.02 | ||
| Main diagnostic status | 1144 | Confirmed | 1088 | 95.10 |
| Suspected | 56 | 4.90 | ||
| Secondary diagnosis | 507 | 1. Peripheral and axial mechanical pathology | 254 | 50.10 |
| 2. Soft tissue pathology | 124 | 24.46 | ||
| 3. Neuropathies | 22 | 4.34 | ||
| 4. Metabolic pathology | 23 | 4.54 | ||
| 5. Infectious pathology | 2 | 0.39 | ||
| 6. Inflammatory and microcrystalline arthropathies | 31 | 6.11 | ||
| 7. Connective tissue disorders and vasculitis | 51 | 10.06 | ||
| Secondary diagnostic status | 501 | Confirmed | 483 | 96.41 |
| Suspected | 18 | 3.59 | ||
| Perceived state of health in the last 12 months | 1134 | Very good | 52 | 4.59 |
| Good | 372 | 32.80 | ||
| Fair | 477 | 42.06 | ||
| Bad | 183 | 16.14 | ||
| Very bad | 50 | 4.41 | ||
With respect to perceived state of health in the last 12 months, 37.39% of patients reported it was good or very good, 42.06% fair, and 20.55% bad or very bad (Table 2).
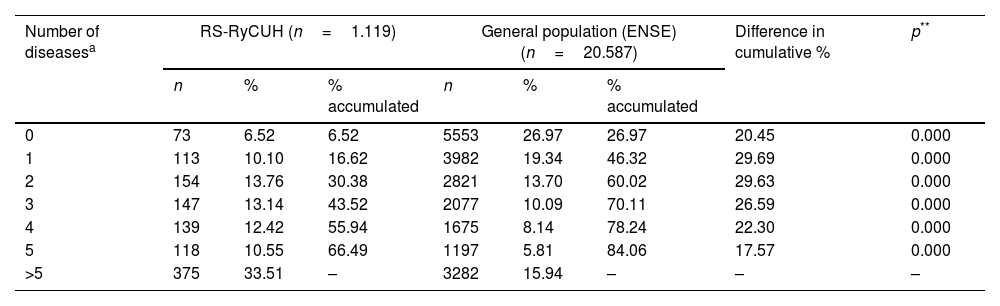
The three most frequent diseases were rheumatological: chronic back pain (lumbar) (45.80%); osteoarthritis (excluding arthritis) (38.46%); and chronic back pain (cervical) (35.84%). After these, the most frequent were high cholesterol (27.27%) and high blood pressure (26.66%) (Supplementary Table 1). A minority of patients, 6.52%, stated they did not suffer from any of the 32 diseases included in the questionnaire (assuming those who answered no or did not respond did not suffer from the disease), 10.10% declared they had one, 13.76%, two, 69.62%, three or more, and 44.06% declared having five or more diseases. The median number of diseases diagnosed by a doctor per patient in the previous year was 4 (IQR: 2–6) (Supplementary Table 2). The number of illnesses per patient was significantly higher in RS-RyCUH patients than in the general population (Table 3).
Number of illnesses or long-term health problems in the last twelve months diagnosed by a doctor. Differences between RS-RyCUH patients and the general population.
| Number of diseasesa | RS-RyCUH (n=1.119) | General population (ENSE) (n=20.587) | Difference in cumulative % | p** | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | % accumulated | n | % | % accumulated | |||
| 0 | 73 | 6.52 | 6.52 | 5553 | 26.97 | 26.97 | 20.45 | 0.000 |
| 1 | 113 | 10.10 | 16.62 | 3982 | 19.34 | 46.32 | 29.69 | 0.000 |
| 2 | 154 | 13.76 | 30.38 | 2821 | 13.70 | 60.02 | 29.63 | 0.000 |
| 3 | 147 | 13.14 | 43.52 | 2077 | 10.09 | 70.11 | 26.59 | 0.000 |
| 4 | 139 | 12.42 | 55.94 | 1675 | 8.14 | 78.24 | 22.30 | 0.000 |
| 5 | 118 | 10.55 | 66.49 | 1197 | 5.81 | 84.06 | 17.57 | 0.000 |
| >5 | 375 | 33.51 | – | 3282 | 15.94 | – | – | – |
RS-RyCUH: Rheumatology Service of the Ramón y Cajal University Hospital; ENSE: National Health Survey of Spain 2011–2012.
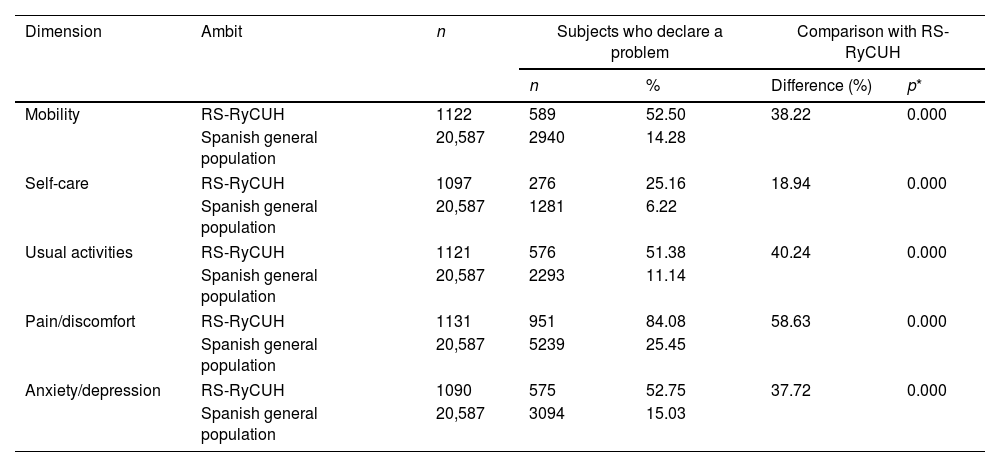
Over half of the patients, 52.50%, declared having a problem in the “mobility” dimension of the EQ-5D-5L, 25.16% in “self-care”, 51.38% in “daily activities”, 84.08% in “pain/discomfort” and 52.75% in “anxiety/depression” (Supplementary Table 3). The proportion of patients with problems in each of the dimensions was higher than in the general Spanish population (Table 4).
Population over 18 years of age reporting a health problem in each of the dimensions of the EQ-5D-5L in SR-HURyC patients, and in the general Spanish population.
| Dimension | Ambit | n | Subjects who declare a problem | Comparison with RS-RyCUH | ||
|---|---|---|---|---|---|---|
| n | % | Difference (%) | p* | |||
| Mobility | RS-RyCUH | 1122 | 589 | 52.50 | 38.22 | 0.000 |
| Spanish general population | 20,587 | 2940 | 14.28 | |||
| Self-care | RS-RyCUH | 1097 | 276 | 25.16 | 18.94 | 0.000 |
| Spanish general population | 20,587 | 1281 | 6.22 | |||
| Usual activities | RS-RyCUH | 1121 | 576 | 51.38 | 40.24 | 0.000 |
| Spanish general population | 20,587 | 2293 | 11.14 | |||
| Pain/discomfort | RS-RyCUH | 1131 | 951 | 84.08 | 58.63 | 0.000 |
| Spanish general population | 20,587 | 5239 | 25.45 | |||
| Anxiety/depression | RS-RyCUH | 1090 | 575 | 52.75 | 37.72 | 0.000 |
| Spanish general population | 20,587 | 3094 | 15.03 | |||
RS-RyCUH: Rheumatology Service of the Ramón y Cajal University Hospital.
Data of the Spanish general population: National Health Survey of Spain 2011–2012.
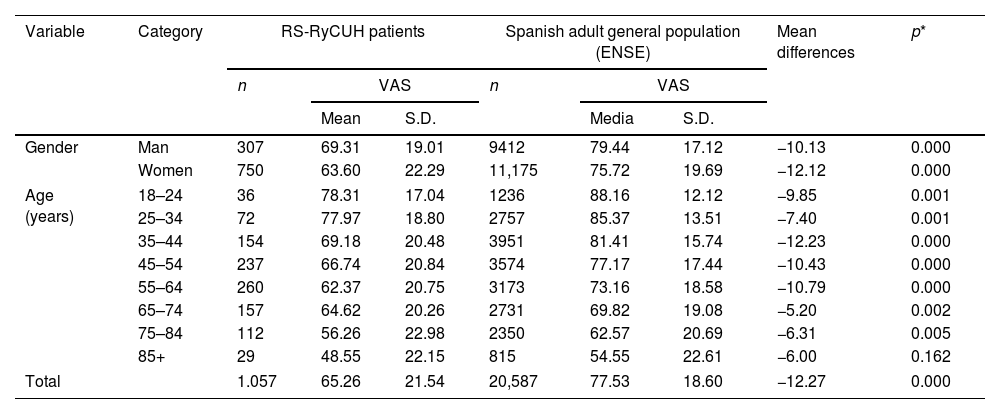
The VAS had a mean of 65.26 (SD: 21.54), and a median of 70 (IQR: 50–80). The VAS was higher in men (mean 69.31) than in women (mean 63.60) (p=0.000; Mann–Whitney U test), and lower with increasing age. For example, in patients aged 18–24 years old it was 78.31, and in subjects over 85 years old it was 48.55 (p=0.000; Kruskal–Wallis test). The mean VAS of the patients (65.26) was lower than that of the general population (77.53) (p=0.000), and also when compared by gender and age, except in those>85 years of age, in which the 6-point difference did not reach statistical significance (p=0.162) probably due to the small number of patients of this age (Table 5).
Comparison of the visual analog scale and the EQ-Index of the EQ-5D-5L in the SR-HURyC patients, with the general Spanish adult population, according to gender and age.
| Variable | Category | RS-RyCUH patients | Spanish adult general population (ENSE) | Mean differences | p* | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | VAS | n | VAS | ||||||
| Mean | S.D. | Media | S.D. | ||||||
| Gender | Man | 307 | 69.31 | 19.01 | 9412 | 79.44 | 17.12 | −10.13 | 0.000 |
| Women | 750 | 63.60 | 22.29 | 11,175 | 75.72 | 19.69 | −12.12 | 0.000 | |
| Age (years) | 18–24 | 36 | 78.31 | 17.04 | 1236 | 88.16 | 12.12 | −9.85 | 0.001 |
| 25–34 | 72 | 77.97 | 18.80 | 2757 | 85.37 | 13.51 | −7.40 | 0.001 | |
| 35–44 | 154 | 69.18 | 20.48 | 3951 | 81.41 | 15.74 | −12.23 | 0.000 | |
| 45–54 | 237 | 66.74 | 20.84 | 3574 | 77.17 | 17.44 | −10.43 | 0.000 | |
| 55–64 | 260 | 62.37 | 20.75 | 3173 | 73.16 | 18.58 | −10.79 | 0.000 | |
| 65–74 | 157 | 64.62 | 20.26 | 2731 | 69.82 | 19.08 | −5.20 | 0.002 | |
| 75–84 | 112 | 56.26 | 22.98 | 2350 | 62.57 | 20.69 | −6.31 | 0.005 | |
| 85+ | 29 | 48.55 | 22.15 | 815 | 54.55 | 22.61 | −6.00 | 0.162 | |
| Total | 1.057 | 65.26 | 21.54 | 20,587 | 77.53 | 18.60 | −12.27 | 0.000 | |
| Variable | Category | n | EQ-Index | n | EQ-Index | Mean differences | p* | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | S.D. | Mean | S.D. | ||||||
| Gender | Man | 304 | 0.788 | 0.184 | 9412 | 0.938 | 0.138 | −0.150 | 0.000 |
| Women | 755 | 0.703 | 0.236 | 11,175 | 0.892 | 0.159 | −0.189 | 0.000 | |
| Age (years) | 18–24 | 36 | 0.858 | 0.143 | 1236 | 0.976 | 0.098 | −0.117 | 0.000 |
| 25–34 | 73 | 0.818 | 0.178 | 2757 | 0.970 | 0.109 | −0.152 | 0.000 | |
| 35–44 | 164 | 0.746 | 0.203 | 3951 | 0.950 | 0.127 | −0.204 | 0.000 | |
| 45–54 | 241 | 0.740 | 0.214 | 3574 | 0.928 | 0.141 | −0.188 | 0.000 | |
| 55–64 | 257 | 0.698 | 0.227 | 3173 | 0.899 | 0.150 | −0.201 | 0.000 | |
| 65–74 | 158 | 0.756 | 0.213 | 2731 | 0.865 | 0.154 | −0.109 | 0.000 | |
| 75–84 | 102 | 0.659 | 0.271 | 2350 | 0.781 | 0.167 | −0.122 | 0.000 | |
| 85+ | 28 | 0.473 | 0.233 | 815 | 0.625 | 0.182 | −0.152 | 0.002 | |
| Total | 1059 | 0.728 | 0.226 | 20,587 | 0.914 | 0.150 | −0.187 | 0.000 | |
EQ-5D-5L: EuroQoL of 5-dimensions and 5-levels; RS-RyCUH: Rheumatology Service of the Ramón y Cajal University Hospital; ENSE: National Health Survey of Spain 2011–2012; VAS: visual analog scale; S.D.: standard deviation.
The EQ-Index was calculated for 1059 patients (mean 0.728; SD: 0.226; median 0.776; IQR: 0.625–0.899). The EQ-Index was higher in men (mean 0.788) than in women (mean 0.703) (p=0.000; Mann–Whitney U test), and tended to be lower with advancing age. For example, in patients between 18 and 24 years old it was 0.858, while in subjects over 85 years old it was 0.473 (p=0.000; Kruskal–Wallis test). The mean EQ-Index in the patients (0.728) was lower than that of the general Spanish population (0.914) (p=0.000), and also when compared by gender and age (Table 5).
DiscussionThe present study, aimed to determine the HRQoL of patients seen in the rheumatology clinic of a university general hospital, detected a worse HRQoL in rheumatic patients than in the general population in all dimensions, especially for the “pain/discomfort”, followed by “daily activities” and “mobility” items. This reduction in HRQoL was observed for all age ranges. The reduction in HRQoL affected all RD subtypes, especially the “peripheral and axial mechanical pathology” and the “soft tissue pathology” group. Although HRQoL is considered a primary objective in chronic disease management, its implementation in clinical practice is limited and there are scarce data in the literature.
The patient sample for this series had a similar distribution, in terms of gender and RD, to that found in other studies.27–31 In addition, the current findings are consistent with previous studies regarding the higher frequency of comorbidities in rheumatic patients when compared to the general population. For example, only 6.5% of patients declared they did not have any disease (besides the disease for which they attended the consultation), while in the general Spanish population this proportion is 27%.24 Other studies also show a higher frequency of any comorbidity in patients with rheumatoid arthritis than in the general population.32–34 In addition, in this study, almost 70% of the patients had three or more associated diseases, while this proportion in chronic patients with other illnesses is 40%.35
The perception of health status as bad or very bad in more than 20% of those surveyed, compared to 6.7% in the Spanish population,21 could be partly due to the high presence of multiple morbidities in rheumatic patients.
These results on HRQoL in rheumatic patients are consistent with Branco et al.’s study.36 The most affected dimension was “pain/discomfort” (84%), followed by “anxiety/depression” and “mobility”, as expected, findings which were similar to other studies in rheumatic patients.37 In the Picavet study, the worst results in HRQoL were obtained in patients with multiple RD in all EQ-5D dimensions compared to patients without RD, mainly in the areas of pain/discomfort (62.5% versus 31.2%) and daily activities (34.5% versus 12.4%).38 When compared with other chronic diseases, RD obtained the lowest HRQoL rates.39 It is important to take into account that RD are mostly chronic, without a curative treatment, and the main therapeutic objective should be an improvement in HRQoL.
As in Sánchez-Iriso's study, the VAS was higher in men than in women,35 and decreased with age, with the mean VAS in RS-RyCUH patients being 12 points lower than in the general Spanish population. The EQ-Index was also lower in patients (0.728) than in the general Spanish population (0.914).
The most important limitation of this study was the lack of completion of some data, especially some items of the EQ-5D-5L, but the maximum loss was 54 (4.7%) data in the “anxiety/depression” dimension, so the study of the dimensions of the quality of life of the EQ-5D-5L was barely affected. The absence of data in any of the 5-dimensions meant that the EQ-Index could not be calculated in 85 (7.4%) patients. In addition, 87 (7.6%) patients did not complete the VAS. This absence of data, most probably due to a random variety of reasons, represented less than 8% of the total, and should not have introduced appreciable biases or altered the results of the study.40
The sample of patients constituted a good representation of the type of patients seen in the rheumatology department of a large hospital. In addition, the sample size, the consecutive inclusion of patients, which minimized potential selection bias, the verification of RD diagnoses by a rheumatologist, and the consistency between the data declared by the patient and the existing information in the MR, as verified in the data cleaning process, may also be considered a strength of the study.
The findings of this study suggest that HRQoL should be considered a fundamental variable in rheumatology clinics to describe the situation of patients and a measure of outcome of interventions they receive across all age groups, aiding the understanding of the effects of the disease and its treatment in patients. The repercussion of medical acts in people's lives is important and the gain in health can only be complete if the HRQoL of patients is improved, they are involved in achieving this multidimensional improvement, and achieve a more active doctor–patient relationship. The patient should not be a passive subject, but should take responsibility for maintaining their health and participate in decision-making in relation to their disease.
More studies are needed to assess the impact of lifestyle, comorbidities, as well as particular RD and their treatments on HRQoL. Studies on the effectiveness of therapeutic interventions in rheumatology should consider HRQoL as one of the key outcome variables.
Conflicts of interestThe authors declare that they have no conflicts of interest.
The following are the supplementary data to this article:


