






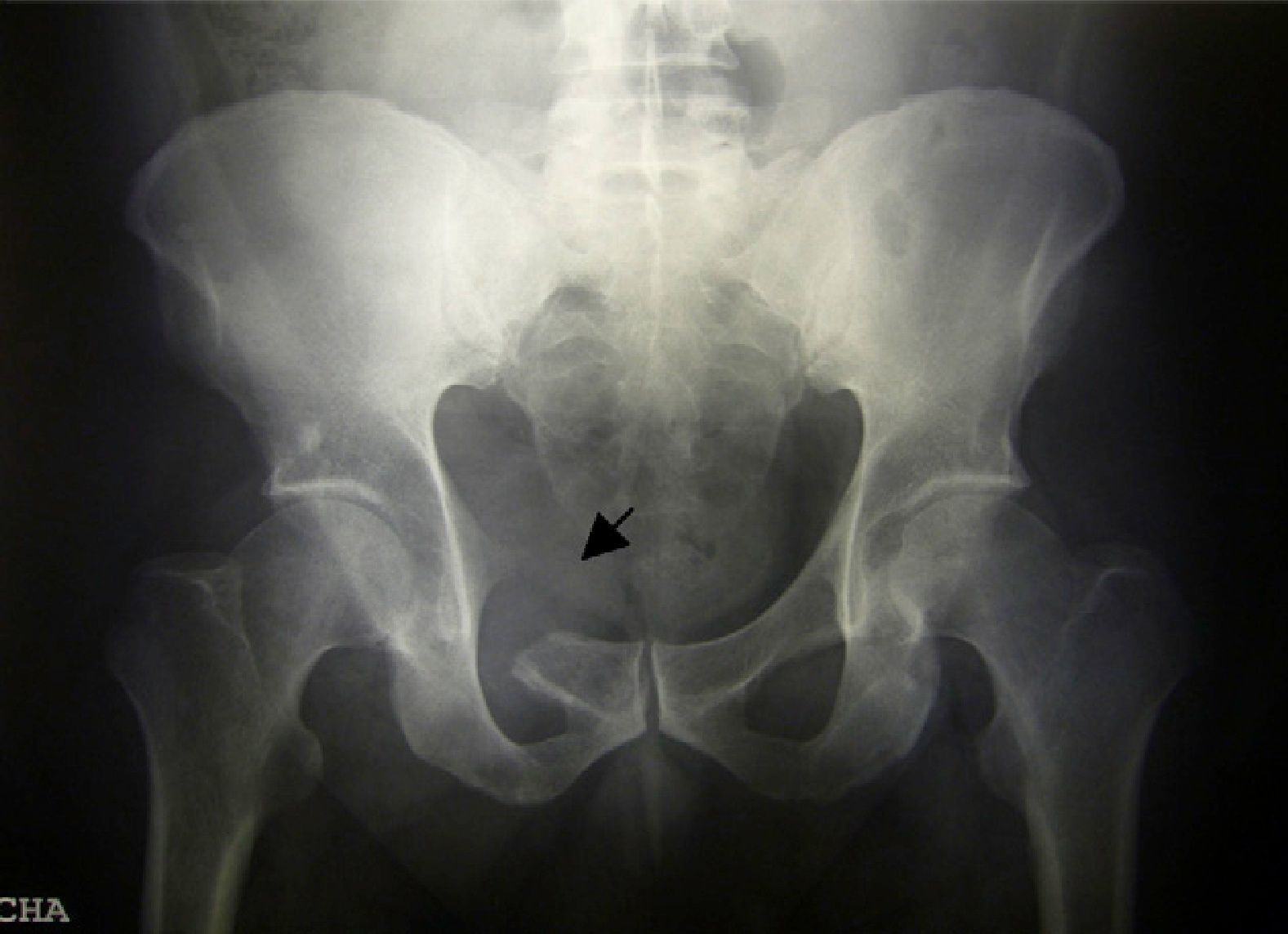
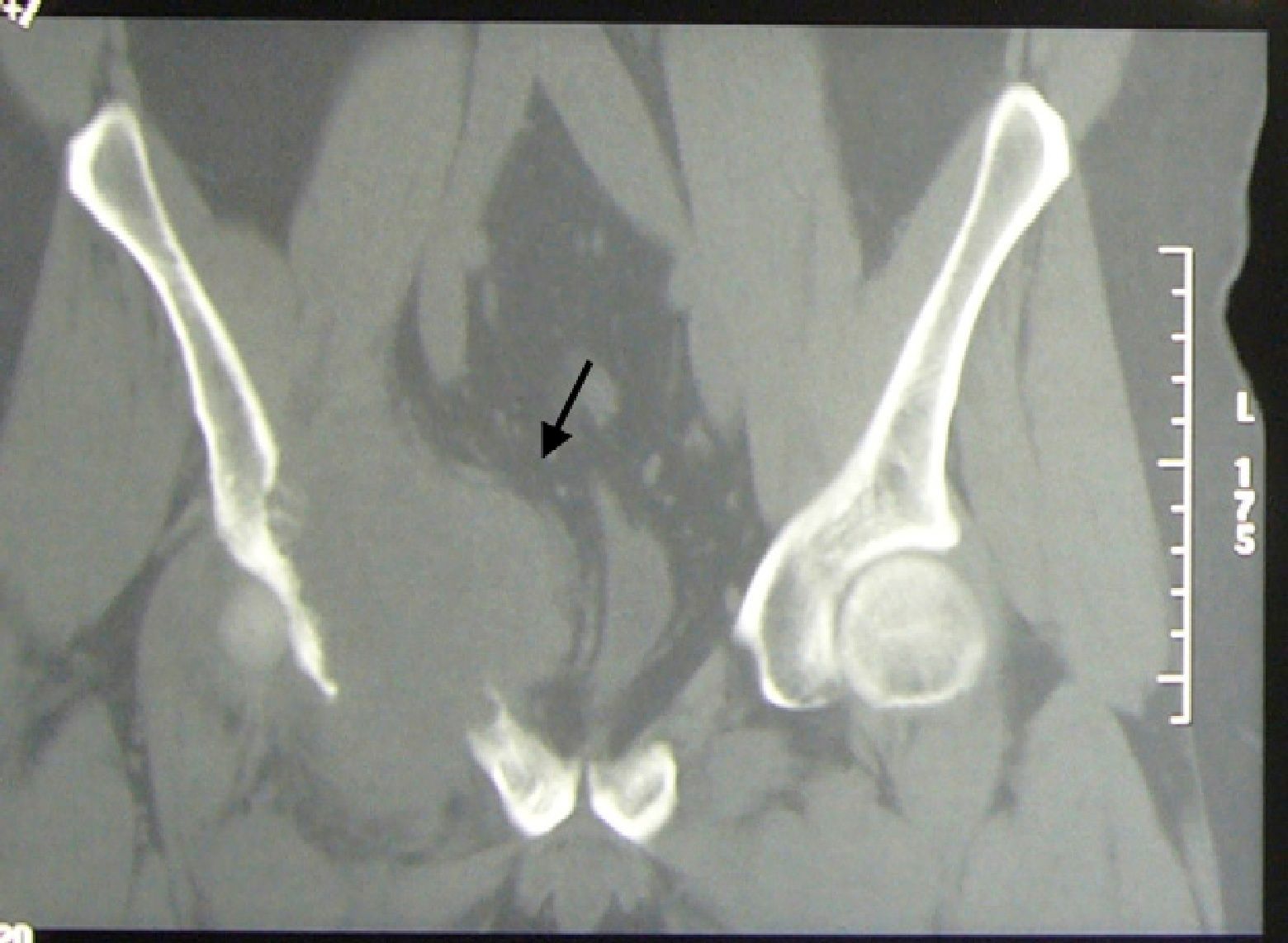
A 43-year-old male came to the clinic due to mechanical lower back pain, which had lasted for 2years. Physical examination showed painful limitation for right leg flexion and extension, with no neurological deficit. Laboratory analysis highlighted hemoglobin 10.6g/dl, normal ESR and GGT 111U/L (0–40). Simple X-ray (Fig. 1), CT (Fig. 2) and MR (Fig. 3) of the hips evidenced a 90mm×80mm×80mm mass in the right hemipelvis with an osteolytic component which affected half of the cotillus, iliac and pubic ramus, displacing the bladder and subjacent structures leftward.
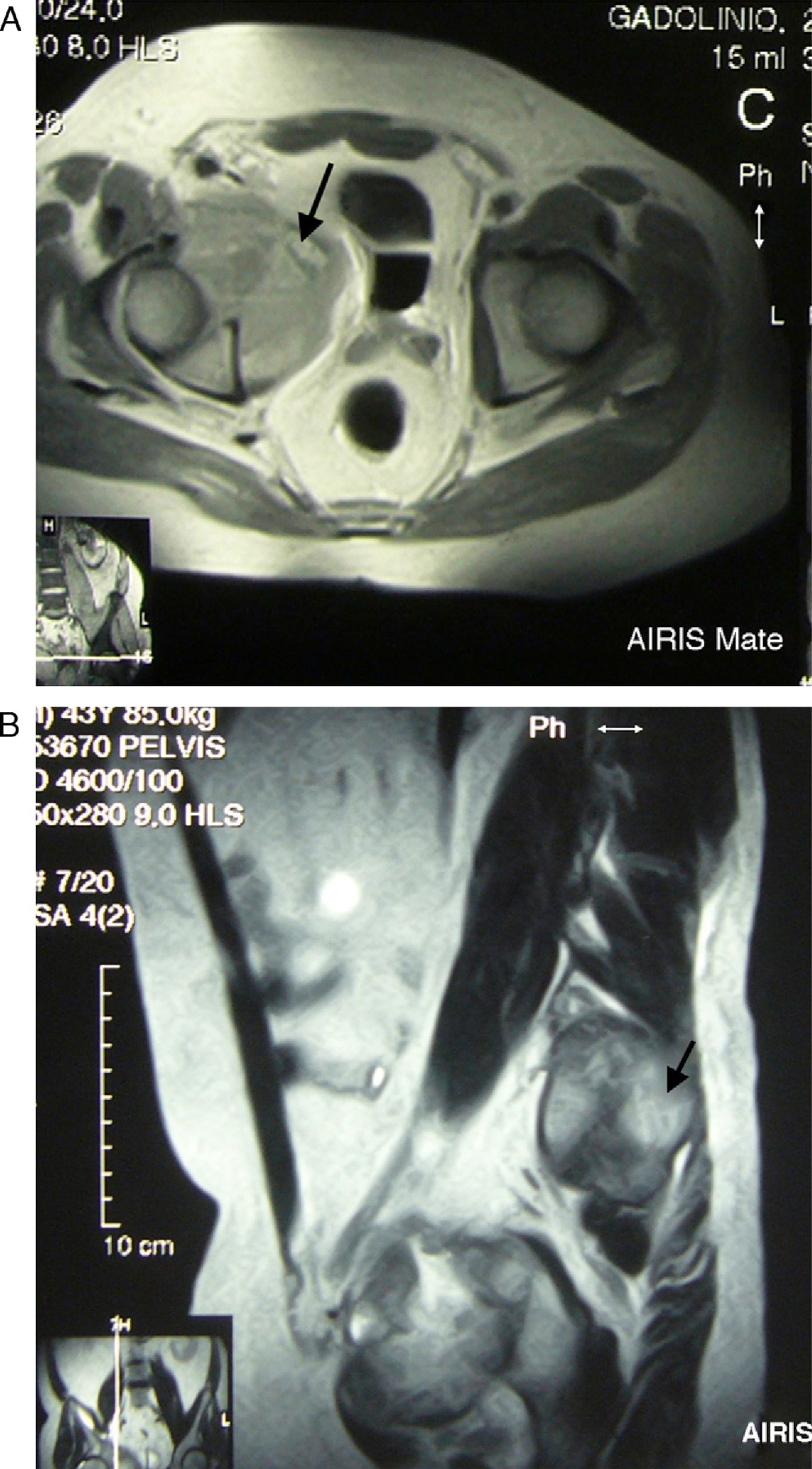
(A and B) Axial and coronal MR of the hips RM in T2 sequence with contrast. A voluminous mass in the right hemipelvis is shown, affecting the anterior half of the cotillum, the iliac and pubic ramus, displacing the urinary bladder and adjacent structures leftward, with an isointense signal with bone and increased intensity with contrast, except in areas of intense necrosis.
The histological study of an ultrasound guided biopsy concluded that the patient presented a peripheral primitive neuroectodermal tumor (PNET)/Ewing's sarcoma (ES). Chemotherapy was started with alternating cycles of vincristin/cyclophoshamide/adriamicine-iphosphamide/etoposid.
DiscussionPrimitive neuroectodermic tumors are neoplasias with a differentiation to neuronal tissue which, if involving peripheral nerves, is called peripheral primitive neuroectodermic tumor.1 Because it shares the t(11;22) translocation with ES, it is considered the same disease. This tumor represents 3%–6% of solid tumors and 1.4%–1.8% of malignant processes, with an incidence of 3cases/million/inhab./year.2 90% of the cases appear between 5 and 30years and is more common in men. It is manifested by pain (in the pelvis, femur or humerus),3,4 swelling and, sometimes, fever, weight loss, anemia and leukocytosis.
X-ray findings reflect osteolysis, erosions, periostitis and soft tissue masses, as in our case. Immunohistochemistry is important to establish the differential diagnosis.5
Important findings in our patient were: age at presentation was uncommon as was the insidious nature of its progression, with no constitutional symptoms, fever or laboratory abnormalities. The natural history of PNET/ES is unknown although it tends to be aggressive in tumors developed in deep areas, when size is large or those presenting translocations.6 A combination of surgery, radiotherapy and chemotherapy attain an increase in survival and disease-free survival.7,8
Please cite this article as: Carrasco Cubero C, et al. Varón de 43 años con masa pélvica derecha. Reumatol Clin. 2012;8:225–6.


