




Infiltration of the thyroid gland by amyloid is a common phenomenon. However, the development of goiter and hyperthyroidism due to amyloid deposition is rare, even in patients with known amyloidosis.1,2 The detection of amyloid goiter as the first manifestation of secondary systemic amyloidosis is exceptionally rare in the literature. That circumstance has led us to present this clinical report.3,4
The patient was a 41-year-old man with a history of myelomeningocele that had been treated surgically at birth, long-standing postoperative sacral ulcer and neurogenic bladder without previously known nephropathy. He was admitted to the hospital with a large goiter and a thyroid storm. He was diagnosed as having Graves–Basedow disease. After medical therapy, the decision was made to perform thyroidectomy, which resulted in the incidental histological finding of amyloid goiter. The supplemental studies aided in establishing a diagnosis of AA systemic amyloidosis, secondary to long-standing indolent sacral ulcer and stage 3 kidney disease.
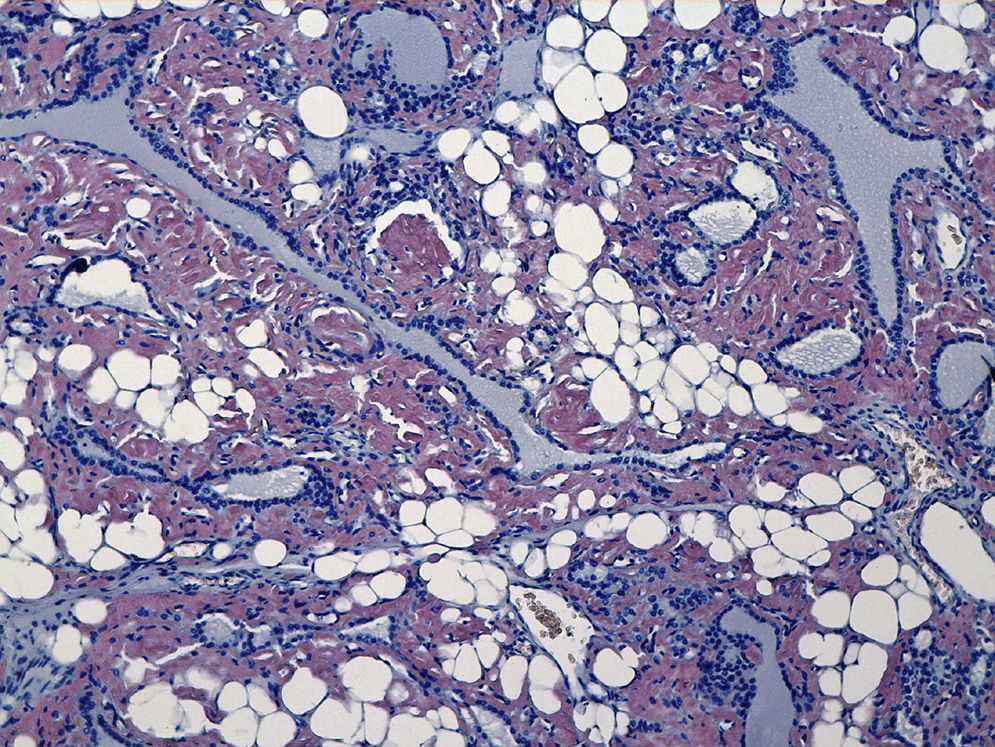
Amyloid goiter is defined as the presence of an extracellular amyloid-like material that produces clinical enlargement of the gland. These depositions show the characteristic Congo red staining (Fig. 1), and also exhibit green birefringence under polarized light microscopy.4,5
The clinical picture is characterized by a rapid, progressive increase in the thyroid volume and a bilobed structure, which is what makes surgery the treatment of choice in these patients.5,6
It is important to have previously ruled out a malignant process, such as anaplastic carcinoma or lymphoma. For this purpose, fine-needle aspiration biopsy of the goiter is a highly useful technique.5,6
The patients may develop symptoms related to the neighboring structures, such as dysphagia, dyspnea and/or dysphonia. Thyroid function is usually normal. However, in a minority of the cases, coexistence of hypothyroidism or hyperthyroidism is detected.7
Amyloidosis comprises a group of diseases characterized by deposition of a protein called amyloid in the extracellular matrix. The most common forms of systemic amyloidosis are primary, involving light chains, and secondary, due to chronic diseases.5,8 In autopsy studies, amyloid is found in the thyroids of 80% of the patients with secondary amyloidosis and 50% of those with the primary form.6
In conclusion, amyloid goiter should be suspected in those patients who have a long-standing, chronic inflammatory disease or process in whom rapid, progressive, bilobed growth of the thyroid gland is detected. Fine-needle aspiration biopsy will aid in establishing the definitive diagnosis and in ruling out other processes that could be malignant.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Cabrejas Gómez MC, González Cabrera N, Gómez González C, Bergara Elorza S. Bocio amiloide como manifestación inicial en amiloidosis sistémica. Reumatol Clin. 2015;11:404–405.


