





To identify barriers and facilitators in the implementation of quality standards in hospital day care units (HDCU) in rheumatology.
Materials and methodsWe analyzed appraisals of HDCU in terms of standards for structure, processes and results. The qualitative approach was conducted through 13 discussion groups created by rheumatology health professionals (7), nursing professionals (4) and HDCU patients (2). The recruitment of informants was done through purposive sampling, attending to variables that form the perceptions of the HDCU. Data analysis was performed using a descriptive-interpretive method.
ResultsThe specialization of the HDCU and specific training in rheumatology for nursing are perceived as the main facilitator for the implementation of standards. Conversely, the delay in the availability of medicines at the HDCU is identified as a barrier that prolongs patient stay and wastes resources. Differences in local regulations are perceived as a potential barrier to equitable access to medicines. The patients gave higher ratings to the care received than to structural variables or those related to process.
ConclusionsThe findings of this study suggest that improvements in the implementation of quality standards in HDCU may include three levels of action: the HDCU, the hospital and a third related to local regulations to access to medicines.
Identificar las barreras y los facilitadores en la implantación de estándares de calidad en las unidades de hospital de día (UHdD) reumatológicas.
Material y métodosSe analizaron las valoraciones sobre UHdD clasificadas en torno a estándares de estructura, procesos y resultados. La aproximación cualitativa se llevó a cabo mediante 13 grupos de discusión (GD) formados por profesionales de Reumatología (7), de Enfermería (4) y pacientes (2) de UHdD. La captación de informantes se realizó mediante muestreo intencionado atendiendo a variables que configuran las percepciones de las UHdD. El análisis de los datos se realizó siguiendo una perspectiva descriptiva-interpretativa.
ResultadosLa especialización de las UHdD monovalentes y la formación específica en Reumatología para Enfermería se perciben como los principales facilitadores para la implantación de estándares. Por el contrario, la demora en la disponibilidad de los fármacos en las UHdD se identifica como una barrera que prolonga la estancia de pacientes y desaprovecha recursos. Las diferencias en regulaciones locales se perciben como una posible barrera para el acceso equitativo a fármacos. El elemento mejor valorado por los pacientes fue la atención recibida, por encima de las variables estructurales o de proceso.
ConclusionesLos hallazgos de este estudio sugieren que las mejoras para la implantación de estándares de calidad en las UHdD pueden incluir 3 niveles de actuación: la propia UHdD, el centro hospitalario, y un tercero relacionado con regulaciones locales de acceso a fármacos.
The hospital day care unit (HDCU) has been defined as hospital care for a matter of hours, whether for diagnosis, clinical research and/or multiple examinations, as well as to administer treatments that cannot be carried out in the outpatient office, but that do not justify the need for admission to the hospital.1 In our setting, the HDCU arose in connection with the development of intravenous biological therapies. It has constituted an important therapeutic advance and results in a notable improvement in the prognosis of certain inflammatory rheumatic diseases. In its brief existence, the rheumatology HDCU has been found to be more effective and to improve the quality of life of the patient.2 Although the advantages of the implementation of the HDCU are evident,3 there is also a high index of agreement on the heterogeneity of its development and the need to introduce quality criteria specific for rheumatology that standardize its role in clinical practice.4
The existence of variability inevitably has adverse effects on patient care and, unnecessarily, wastes time and resources. If, moreover, we add a socioeconomic aspect like the one we confront, dominated by control of health spending, it is very much to the point to consider the evaluation of available resources to respond to the current forecast for an increase in chronicity in Spain.5
The recent VALORA project of the Spanish Society of Rheumatology (SER) detected heterogeneous functioning and certain variability in HDCU that cannot be explained only by the different complexity of the hospitals.6 However, there are no qualitative studies that approach the investigation of possible barriers and facilitators in the implementation of quality standards. This article focuses on identifying these factors within the framework of the VALORA project based on a qualitative approach.
Materials and MethodsThe VALORA project is a multicenter, cross-selective, descriptive study within the framework of the ÍCARO plan (http://icaro.ser.es/), the objective of which is to improve clinical practice through quality care.
This project integrates quantitative methods, the results of which have been previously reported,6 and the qualitative approach. This multimethod strategy responds to a dual purpose: to improve the production process of this research and to lend greater credibility to the outcome, by means of methodological triangulation.7
The present study focuses on the use of discussion groups (DG) as a suitable tool for the identification of barriers and facilitators, in this case, relative to the implementation of quality standards. The DG can be defined as a semistructured group interview, designed to investigate the common ground of a group of individuals who, found in a discursive situation, tend to offer “stereotypical” discourses characteristic of the circle to which they belong.8
The informants were selected from professionals of 89 centers of the 116 existing, who took part in the quantitative approach to the VALORA project. We collected information from all of the Spanish autonomous communities (AC)—except the Balearic Islands and Ceuta, neither of which provided data.
We established 13 DG, a sufficient number to achieve a priori the objectives of the investigation and theoretical saturation. Physicians and nurses who participated in the study were from 16 Spanish AC (with the exception of the Balearic Islands). The meetings of the DG were held in different well-communicated cities to facilitate participation, regardless of the home AC of the informants. The recruitment of informants was carried out by purposive sampling in accordance with criteria of maximum intragroup variability in terms of age, sex and group homogeneity according to professional categories. These criteria could configure the different perceptions in reference to the HDCU with respect to sex, age, years of practice in the specialty, geographic representativeness and years of training. The DG involving patients were incorporated into the study as a pilot experience and, for logistic reasons, were recruited in different centers only in the Community of Madrid, although they followed criteria regarding sex, age and disease duration.
The study variables were grouped into 3 blocks: structure, processes and results, according to previously defined standards.4 On the basis of these standards, we drafted an outline that was utilized for the good functioning of the DG, thus ensuring that all the study variables would be included in the sessions (see supplementary material in Appendix 2). All of the DG sessions were recorded and transcribed verbatim. The analysis of the data was carried out following a descriptive-interpretive perspective, that is, by means of the interpretation of the data obtained and the formulation of discourse analysis.9 For the treatment of texts and the development of the analysis plan we utilized Atlas.Ti 7.0 (http://atlasti.com/es/h).
All of the participants were volunteers and received no compensation of any kind. The participants were informed of the objectives and characteristics of the study and were asked to give their consent to participate and to grant permission for the recording of the sessions. Confidentiality and anonymity were guaranteed.
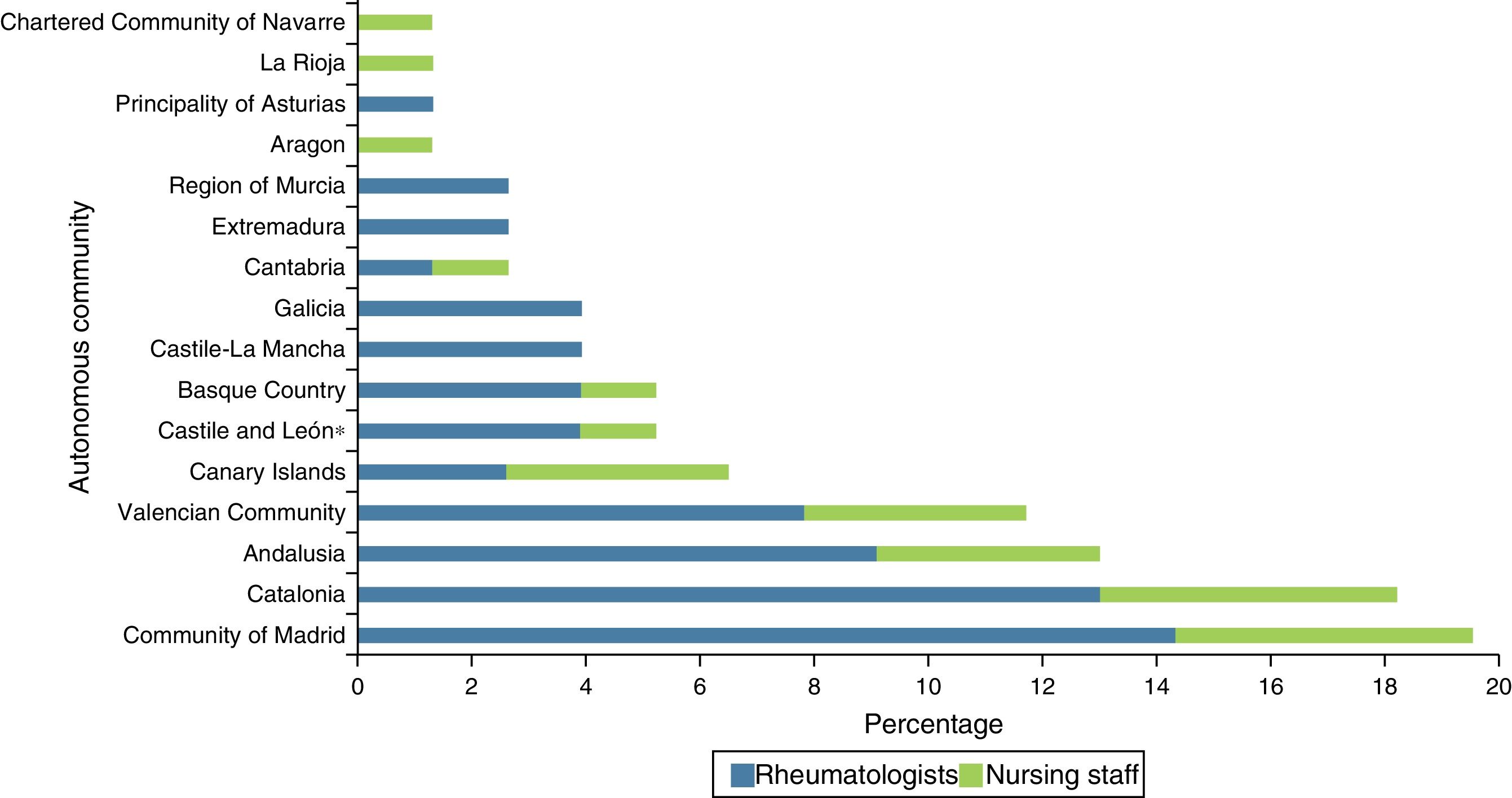
ResultsThe GD were held in May and June of 2012 and a total of 88 informants participated. The DG were configured according to the variables considered a priori in the design, except for the variable sex (Table 1). The distribution of the rheumatology and nursing professionals by AC is shown in Fig. 1.
Characteristics of the Informants Participating in the Rheumatology, Nursing and Patient Discussion Groups.
| Rheumatology | Nursing | Patients | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 (n=9) | Group 2 (n=6) | Group 3 (n=7) | Group 4 (n=9) | Group 5 (n=5) | Group 6 (n=10) | Group 7 (n=8) | Group 8 (n=5) | Group 9 (n=5) | Group 10 (n=6) | Group 11 (n=7) | Group 12 (n=6) | Group 13 (n=5) | |
| City | Madrid | Madrid | Valencia | Seville | Bilbao | Barcelona | Madrid | Madrid | Madrid | Seville | Barcelona | Madrid | Madrid |
| Age (years), median (IQR) | 46 (41–50) | 37.5 (35.5–37.5) | 45 (37–51.5) | 36.5 (31.75–45.25) | 49 (46–50) | 37 (34.25–41) | 44 (41.5–51.25) | 40 (31–48) | 52.5 (49–55.75) | 52 (46–60) | 40 (36–51) | 50.5 (43.5–62.75) | 62 (60–63) |
| Sex, women (%) | 55.55 | 50 | 42.86 | 44.4 | 40 | 70 | 37.5 | 100 | 80 | 66.67 | 85.71 | 83.33 | 40 |
| Experience (years), median (IQR) | 12 (10–12) | 7 (5.25–11) | 8 (7–11.5) | 6 (5–9) | 12 (12–13) | 7.5 (6–11) | 6.5 (4–6.5) | 3 (3–4) | 5.5 (4.5–6) | 4.5 (2.5–7.25) | 6 (3–11) | – | – |
| Disease duration (years), median (IQR) | – | – | – | – | – | – | – | – | – | – | – | 9.5 (9–11.5) | 20 (11–22) |
– not applicable; IQR, interquartile range (25th–75th percentiles).
There is a marked preference for the dedicated HDCU, especially if the workload is considered to be excessive. The 3 groups analyzed coincide in this option, although it is not perceived to be a determining factor of the quality of the care provided. There are other structural variables that were regarded to be relevant. The latter include the size of the center, availability of enough room to accompany the patient during the treatment, while ensuring privacy, the good condition of the installations and/or the suitability of the nursing offices.
In the multipurpose HDCU, the lack of permanent specialized personnel and the added difficulty in management are perceived as a barrier. To address this problem, we propose to concentrate the patients according to specialties on specific days of the week. This measure also helps to solve another barrier suggested by the patients with respect to sharing space in the HDCU with oncology, since the treatments administered for cancer are identified with those administered to them. Moreover, a specialized HDCU facilitates an integrated unit (assessment, analytical tests and procedure in a single visit).
One of the major factors leading to the success of HDCU pointed out by professionals, are the advanced skills required by the rheumatology nursing staff. Nursing professionals working in the HDCU are assumed to be more specialized and to have a greater knowledge of both the treatments and of the medical history and course of the patients. The major demand required of these professionals is not necessarily updated knowledge in rheumatology, but competence in the utilization of specific drugs and in the management of possible flares. In the discourses, 2 pathways are proposed for preparation: through clinical experience or by specific training. In general, there is a demand to promote the latter option, since current training resources are considered to be insufficient.
On the other hand, the coordination of the hospital pharmacy, especially the delay between prescription and administration of the drug, is perceived to be another great barrier. While the physical distance has an effect on the reception of medications, the temporal distance is perceived to be more concerning. A delay in the delivery on the part of the pharmacy impedes complying with the optimal sequence of the HDCU—admission, visit with a medical professional, laboratory tests, waiting, treatment, recovery and medical discharge—within schedule. In this respect, the hours of the HDCU, in most cases, are only during the morning. The immediate consequences for the patients are the prolongation of the stay or unnecessary admissions, whereas, for the health system, this means a reduction in the profitability of the infrastructures. To improve this situation, the norm is to implement a wide variety of operational protocols, depending on the needs and resources of each center. In general, given these circumstances, HDCU in which there is rapid access to drugs and/or that have an effective intranet are capable of attending to more patients within the same amount of time, without having to prolong its hours. In any case, the experiences that report that there are physicians on call in the hospital pharmacy during the afternoon shift substantially reduce delays in the delivery of medicines.
With respect to the above, there is also a generalized perception as to the limitations derived from regulations established locally or by the AC. The restrictions imposed by hospital commissions on the hour at which certain treatments can be administered are not always accepted by the professionals and require a special effort to make sure that the patient receives the prescribed treatment.
Processes in Rheumatology Hospital Day Care UnitsBoth professionals and patients are satisfied with the plan for admission and consider it important that the patients receive information worded in such a way that is adapted to their needs and level of knowledge. As a facilitator, it is recommended, that this information be accompanied by a phone number and electronic mail address for contact. The person accompanying the patient is considered to be a good recipient of the information, especially when the patients are underage or elderly.
The rheumatologist conveys information on the procedures, whereas health education is mostly provided by nursing professionals. Appropriate information is a key facilitator in reducing possible adverse situations. Likewise, it is considered important to offer data on the cost of drugs, and it is even proposed to employ tools like an informative health care bill.
References to informed consent (IC) are not always positive. On the part of professionals, its value is recognized as being a legal guarantee, however, it is not considered an effective means of communication since, on occasion, patients sign it without reading it or not understanding the document in its entirety. As a facilitator, we suggest that the form be given to patients during a previous visit so that they can sign it on the day the treatment is to begin, thus ensuring they have the necessary time to come to understand it. Other HDCU accompany these documents with adapted educative material.
Patients consider the treatment received to be satisfactory, this being one of the most appreciated variables on the part of professionals. The HDCU are proposed to be an advantage as compared to other services, as they permit providing greater attention to the patient and offering a more personalized relationship.
Quality plans are designed by the hospital and do not always adapt specifically to rheumatology HDCU. We mention, for example, the use of identification bracelets, that are not always considered a priority in comparison with other standards in the care process in the HDCU, such as those based on waiting times, comfort and the possibility of being accompanied. Likewise, we point out that these and other variables that influence perceived quality, such as waiting for access to the HDCU or delays in the delivery of drugs, may by derived from other support services that have nothing to do with the HDCU.
With respect to protocols, they are perceived as a tool that contributes to improving the quality of the service and treatment administration, especially in the multipurpose HDCU or those in which there is no rheumatologist assigned to the HDCU. The current situation of budget adjustments is another regulatory barrier that varies from one AC to another, and does not always enable the application of the initially designed protocols.
Results in the Rheumatology Hospital Day Care UnitsThe satisfaction perceived in the quality of care is always positive, regardless of how it is recorded. When evaluating quality, 2 scenarios are proposed, depending on the care workload. In those in which it is high, mechanisms are set up, like suggestion boxes or complaint forms; whereas, in those in which the demand is lower, there are systems of evaluation carried out periodically by means of satisfaction surveys. The management considers that results that are positive in terms of perceived quality, in both scenarios, are more effective than claims made by the personnel of the center. On the other hand, the needs of the patients do not always coincide with the needs projected by the nursing staff on their behalf; rather than the comfort of the nursing office or waiting times, patients are concerning about aspects such as the quality of the food or the upholstery of the chairs.
Finally, processes of external certification are not considered indispensable, since considerable resources are devoted to obtaining and implementing them, and they are not maintained over time. It was found that the implication and interests of the professionals in this aspect differ from those of the management.
DiscussionThe present report and its contributions prove to be novel in that they deal with the identification of barriers and facilitators for the effective implementation of quality standards from a qualitative perspective. The enhancement of the dimensions of the study by means of methodological triangulation7 constitutes an added value that helps to achieve a better understanding of the reality of the HDCU, completing and extending the contributions of the quantitative investigation of the VALORA project.6 On the other hand, it is the first qualitative approach to the HDCU at the level of the Spanish state.
One of the major findings was the high level of agreement concerning the facilitating role of specialization. First, due to the preference of dedicated HDCU over multipurpose units, which comes into contradiction with the current trend in which the number of multipurpose HDCU continues to grow and now amounts to more than 90% of those existing at the state level.6 Second, due to the coincidence in the need for specific training and preparation of a nursing staff in rheumatology, referred to both by physicians and nurses. However, in the quantitative approach to the VALORA project,6 less than half of the nursing staff stated they had some type of specific training in rheumatology. This demand is not new. Although Ivorra et al. mentioned this lack in 2010,10 the resources provided for training have not increased, the offer on the part of hospitals is limited and the options are reduced to the training facilitated by drug companies or by the SER.
Another key result derives from the discrepancies detected in the quantitative study when the coordination with the hospital pharmacy is evaluated. Whereas in the DG, the emerging discourses focused on the delay between drug prescription and its administration as one of the major barriers detected, the quantitative study reported a coordination that was efficient in 88% of the centers,6 since the authors utilized a broader concept that encompassed electronic prescription, vial optimization and the use of efficient medication, together with an acceptable delay.
A third discrepancy is related to the complexity of the center. Although this was not considered one of the variables when organizing the DG, the discourses of the informants did mention differences in function depending on whether the HDCU belonged to a regional, general or major hospital or with a complex. In contrast, in the quantitative study, in reports in which the results were stratified according to this pattern, only a few variables showed significant differences.6
With respect to key documents, there is consistency in the failure to utilize IC forms and the lack of standard work procedures (SWP). The quantitative study also reveals that 48% of the HDCU had no SWP.6 This idea reinforces the need to employ established protocols and implement new ones whenever those existing are inadequate, with special attention to multipurpose HDCU.
On the other hand, a constant in studies on quality, including the present report, is the correlation of a personalized relationship with treatment adhesion, which is particularly important in chronically ill patients. As has been shown, HDCU strengthens bonds with the patients and favors this confidence. However, if a close relationship with the health care staff is a major factor in generating this trust,11 knowledge and communication skills are necessary factors for conveying security to patients. Again, specific training would strengthen these capabilities.
If we focus on the discourse of the patients, we can point out their general satisfaction with the care they receive. However, we can synthesize 2 specific demands. One is related to the fear of the discontinuation of medications with which they are satisfied and whose cost they know, a fear influenced by the socioeconomic context in which the study was conducted. The other finding is a preference for dedicated HDCU, linked to the stigma of a possible identification of drugs to treat cancer with those prescribed to them.
One of the strengths of this study is that is involves DG with patients who evaluated the HDCU. The integration of the perspective of the patients introduces interesting points of view, such as the divergence between the satisfaction of the patients perceived by the professionals and real patient satisfaction. However, the quantitative study reveals that only 21% of the centers carry out evaluations of patient satisfaction,6 an essential source of information; in fact, patient perspective is being increasingly taken into account in planning and evaluation.2
We wish to point out that, although we applied a methodology suitable for the objectives. The present report has certain limitations. First, DG do not always succeed in bringing together the appropriate theoretical number of participants to guarantee a group configuration and productive capacity.12 Likewise, sex parity is only achieved in the general calculation of a rheumatology DG, but it was not possible for nursing. Women participated more than men, exceeding the distribution by sexes proposed by the Spanish 2011 Labor Force Survey.13 Another limitation to be pointed out is the experience of including patient DG. Although this is of interest, it was limited to 2 DG and to a specific territorial setting. Thus, it should be made more extensive in similar studies in the future.
In short, the qualitative analysis enabled us to study in depth the limitations and the opportunity for improving the implementation of quality standards in the HDCU. These can include 3 levels of action. The first would be attributable to the characteristics of the HDCU itself, where the major facilitator has to do with specialization and the preference for a dedicated HDCU. The second depends on the type of hospital to which the unit belongs, where the lack of efficient coordination with other services that increase the delay in the times from drug prescription to its administration that is perceived to be the major barrier. Finally, a third level would be related to the particular features and the regulatory framework of each AC.
Lastly, in line with other reports published by the SER, this study supports the efforts of that society to improve the quality of the care received by rheumatology patients.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FinancingThe Spanish Foundation for Rheumatology (FER), with funds granted by Roche to finance the ÍCARO plan. The company did not participate in the design of the project or intervene in the conclusions or the writing of the final report or the present manuscript.
Conflict of InterestThe authors declare they have no conflicts of interest in relation to the present article.
The authors of this article with to express their thanks to the patients and nursing and rheumatology professionals who participated in the discussion groups for their interest and involvement in the subject of the study.
We also want to thank Estíbaliz Loza Santamaría for her participation in the design of the study.
Pilar Plana Macarulla, Esther Álvarez, Jennifer de la Torre, Pilar Pérez Ayuso, Laura Cano García, Sagrario Bustabad, Hector Corominas i Macías, María Victoria Hernández, José Andrés Román Ivorra, José Luis Marenco, Carlos Fernández López, María Montoro, Federico Navarro Sarabia, Laura Nuño, Eva Pérez Pampín, Joaquín Belzunegui, Carlos Marras, Concha Delgado and Javier Ballina.

Composition of the scientific committee of the VALORA project available in Appendix A.
Please cite this article as: Martín Martínez MA, Zaragoza Gaynor GA, Martínez Fernández C, Gobbo Montoya M, García-Vicuña R, en representación del Comité científico del proyecto VALORA. Barreras y facilitadores en la implantación de estándares de calidad en las unidades de hospital de día reumatológicas. Análisis cualitativo del proyecto VALORA. Reumatol Clin. 2018;14:196–201.


