






Avascular carpal bone necrosis is a relatively infrequent condition which generally involves the semilunar bone (Kienböck's disease)1; the scaphoid can be affected with less frequency, something called Preiser's disease. Generally, these abnormalities of bone perfusion are mainly due to trauma, prolonged use of corticosteroids,2 chemotherapy,3 systemic disease2 or scaphoid hypoplasia.2,4
A 42-year-old businessman, with no prior history of trauma or other problems, came to the clinic due to pain and swelling of the left wrist for the past 5 months. He had self-medicated with non-steroidal anti-inflammatory drugs (NSAID), showing a partial response. A month after the onset of symptoms, he presented similar findings on the right wrist. Physical examination showed mild pain and swelling of both wrists, with range of motion mildly limited due to pain; negative Finkelstein maneuver bilaterally. Laboratory test results including blood count, liver and renal function tests, as well as serum calcium, phosphorus, vitamin D3 and parathyroid hormone were all normal. Rheumatoid factor, antinuclear antibodies (HEp-2), lupus anticoagulant and IgG and IgM anticardiolipin antibodies were negative, as was serology for human immunodeficiency virus. He additionally underwent a bone densitometry that was normal (T score L1–L4, 0.5; T score femoral neck, 1).
Carpal X-rays showed bilateral scaphoid bone rarefaction, with marked sclerosis and severe degenerative signs (Fig. 1), this lesion was confirmed on magnetic resonance imaging (MRI). These findings were compatible with bilateral osteonecrosis (ON), leading to the diagnosis of bilateral, idiopathic Preiser's disease, upon not finding any associated pathology (Fig. 2A and B).

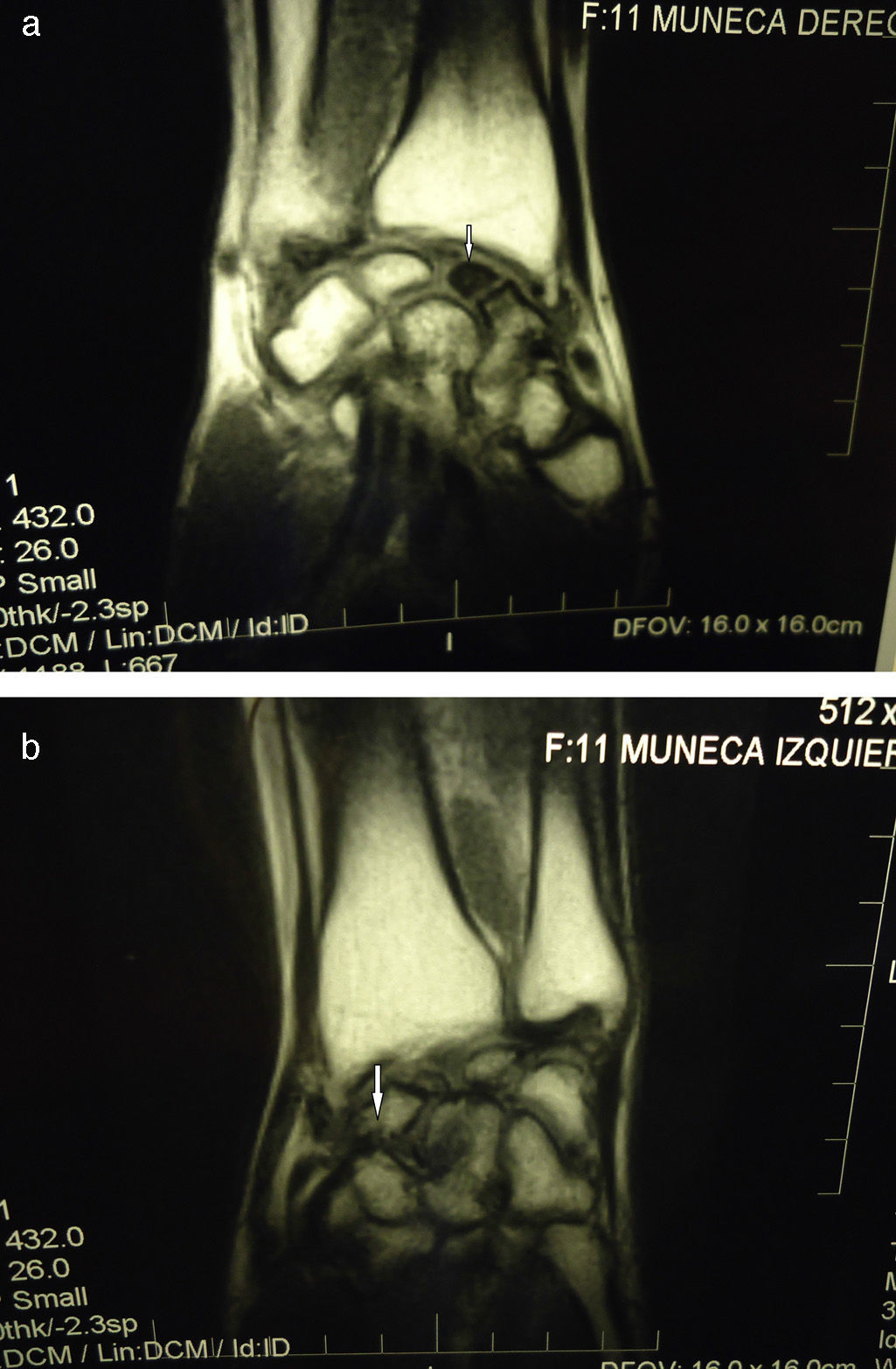
(A) Coronal MRI T1WI (TR 432, TE 26). Right scaphoid fracture with necrosis of the proximal fragment, markedly hypointense (arrow), with chronic degenerative changes due to instability. (B) Coronal MRI T1WI (TR 432, TE 26). Fracture of the left scaphoid bone without consolidation or changes in the signal pattern of the proximal fragment, with degenerative changes due to instability (arrow).
The traumatology department suggested bilateral carpal surgery but the patient rejected the proposal and is currently treated with NSAID and repose orthesis, with symptom improvement.
In 1910, Preiser5 described 5 patients with a scaphoid fracture that evolved to avascular necrosis with time, with trauma being the cause in these cases; the term Preiser's disease is frequently used also for idiopathic ON.
The scaphoid bone's blood perfusion is delivered through branches of the radial artery, which enters the bone on its proximal side; any alteration in the perfusion at this level may generate bone ON.6
Generally, patients present with insidious and progressive pain lasting months to years on the dorsoradial aspect of the wrist. Upon examination there may be inflammation, movement limitation and loss of strength; these symptoms mainly occur on the dominant side.6 In our patient, symptoms presented bilaterally, although its onset was on the non-dominant side.
In accordance with the radiological findings, the lesion might be staged using the Lanzetta and Herbert classification, as modified by Kalainov7; according to this scale, our case presented bilaterally with a stage IV lesion (collapse, fragmentation and periscaphoid osteoarthritis) (Table 1).
Staging of Preiser's Disease.
| Stage | Radiological findings |
| I | Normal X-ray. Abnormal findings on magnetic resonance. Positive bone scan |
| II | Proximal pole sclerosis of the scaphoidGeneralized osteoporosis |
| III | Fragmentation of the proximal scaphoid pole with/without pathological fracture |
| IV | Periscaphoid collapse, fragmentation and osteoarthritis |
Treatment is controversial6; non surgical measures consist of physiotherapy and kinesiotherapy, immobilization, NSAID and, occasionally, steroid infiltration.7,8 Multiple surgical approaches may be used in these cases, among which carpectomy of the proximal row is included,9 proximal scaphoid excision with a silastic replacement,10,11 radial styloidectomy with bone debridement and implant,10 total wrist arthroplasty,12 large and semilunar bone fusion or scaphoid debridement with vascularized bone implant.7 Revascularization procedures are performed in those cases with necrosis but without degenerative changes, while more aggressive treatments (proximal row carpectomy of the wrist) are indicated in patients who already have osteoarthritic changes.6,13
Our patient rejected surgical treatment and is currently in physiokinetic therapy, NSAID on demand, allowing him to perform activities of daily living with mild discomfort.
In conclusion, Preiser's disease is an infrequent cause of carpal pain that must be considered in patients who do not improve with common treatment, with the objective of performing a MRI in the early stages of disease.
We wish to thank Dr. Daniel Forlino, of the Resistencia radiological clinic, for his help in the interpretation of images.
Please cite this article as: Got J, Cavallasca JA. Necrosis avascular bilateral del escafoides (enfermedad de Preiser), una causa infrecuente de dolor de muñeca. Reumatol Clin. 2014;10:418–419.


