




The beneficial effect of antimalarial drugs in the treatment of discoid lupus erythematosus (DLE) has been known since 1984, when Payne reported the efficacy of quinine.1 Chloroquine is employed in the treatment of cutaneous lupus erythematosus because of its photoprotective, anti-inflammatory and immunomodulatory effects.1 It has a good safety profile in the treatment of rheumatic diseases. However, on occasion, it produces adverse events (AE) that represent an unusual problem for clinicians. Severe AE are dose-dependent, and that which requires the greatest vigilance is retinal toxicity, although infrequent, because it can produce blindness. Nevertheless, gastrointestinal, neuropsychiatric and cutaneous AE are the most common causes for the discontinuation of antimalarial treatment.2
We report the case of a 61-year-old woman diagnosed with DLE who began to receive chloroquine at 150mg/day which she took for 2 years. It was discontinued when she developed blurred vision without retinopathy. The initial physical examination, when she was 64 years of age, revealed blackish spots in the mucosa of the inner lining of the cheeks and lips, accompanied by nail dyschromia (Fig. 1), without skin hyperpigmentation; she had cutaneous lesions on face and scalp characterized by erythema, scaling, corneal opacities and atrophy. She was diagnosed with chloroquine-induced hyperpigmentation, and DLE and treatment was begun with topical fluocinolone, azathioprine and the use of a sunscreen. When she was 66 years old, we observed remission of DLE, persistence of mucosal hyperpigmentation and a reduction in nail pigmentation (Fig. 1D).
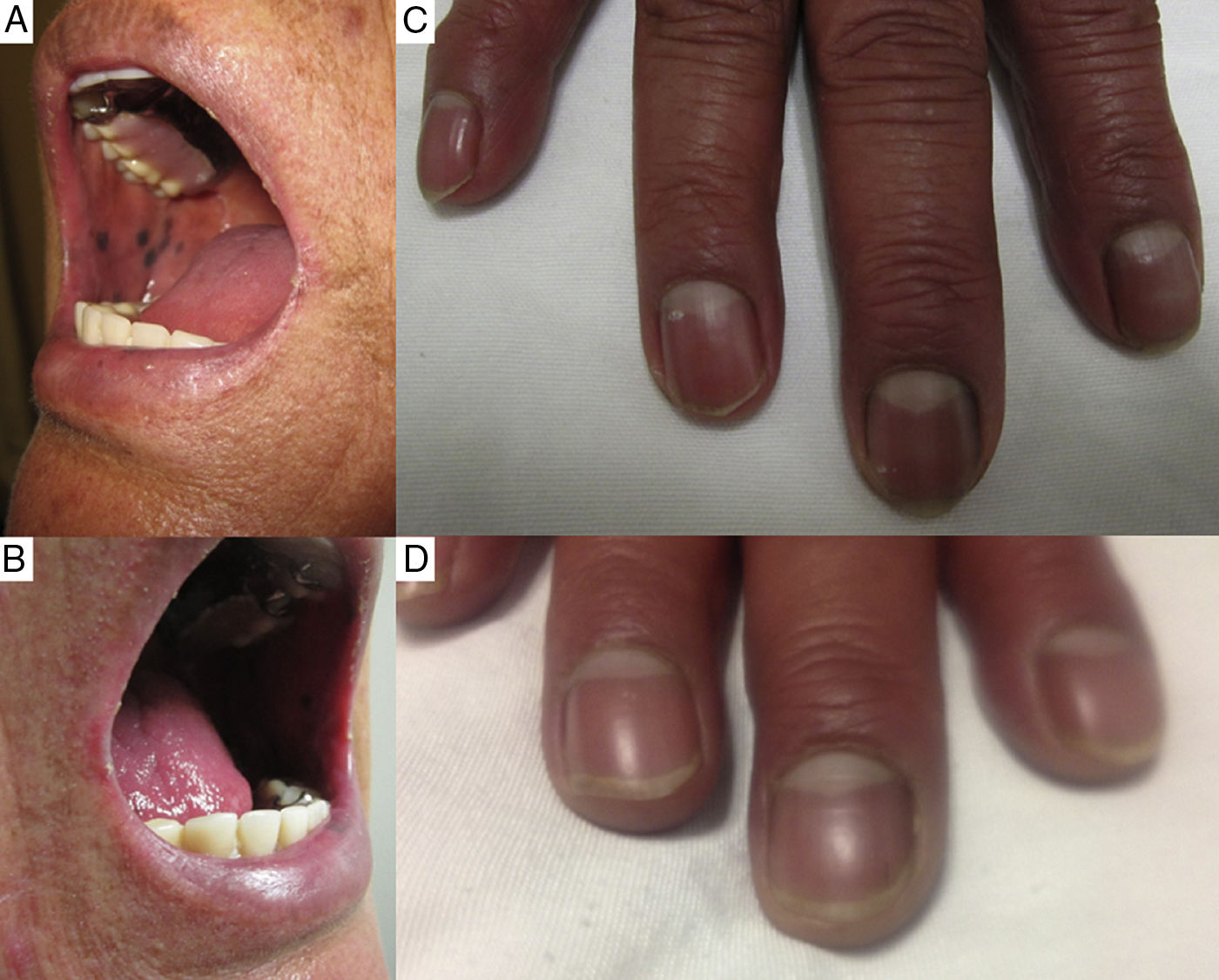
(A) and (B) The presence of hyperpigmented spots on the mucosa of the inner lining of the cheeks and lower lip, with well-defined borders. (C) Presence of brown-colored hyperpigmented bands in the area of the fingernails. (D) Decrease in the intensity of the pigmentation in the area of the fingernails (although it did not completely disappear) 3 years after discontinuing chloroquine.
Due to its avidity for melanin-containing cells in the skin and retina, chloroquine can produce skin, nail and scleral pigmentation.3 Its concentration can be 20–200,000-fold greater than the serum level and it can remain in the skin for up to 6 or 7 months after the treatment has been discontinued.1,4 As in our case, the visual disturbance due to corneal deposits is a reversible AE. It results in blurred vision and colored halos that the patient sees around lights. It is detected in up to 90% of the patients who take chloroquine, and has no direct relationship to the retinopathy.1
The most widespread mucocutaneous AE are xeroderma (63%), skin hyperpigmentation (29%–33%) and pruritus (28%).4 Less common sequelae are mucosal hyperpigmentation (5%–7%), nail dyschromia (0%–7%) and hyperpigmentation of the hair (0%–7%).4,5 Skin hyperpigmentation is characterized by a bluish-gray or dark brown pigmentation on the face, neck, forearms and legs, and the AE is considered reversible as it remits after the treatment is discontinued.1,6 Some authors consider that skin hyperpigmentation may be a marker of a higher risk of retinopathy.7 Nail dyschromia can produce a blue, brown or gray pigmentation of the nails that does not move distally with the growth of the nail. The discontinuation of the drug results in a decrease in the intensity of the pigmentation, although it often does not completely disappear.1,3
In the region of the mucosa there are pigmented areas of bluish-gray or bluish-black color, of varying size and generally well limited. It is considered to be a reversible AE, and while there may only be a decrease in the pigmentation or it may persist, it is not associated with a retinopathy.7,8 In most cases, only the hard palate is involved and, as it does not affect the soft palate, there is a line of demarcation.4,7,8 There is no explanation of why it only affects the hard palate.7 The involvement of the oral and labial mucosa has rarely been reported.7,9 However, a study conducted in Brazil,4 that demonstrated a high prevalence of mucocutaneous AE, reported a greater involvement of the oral mucosa than of the palate.
The cause of mucocutaneous hyperpigmentation is not very clear. It could be related to the accumulation of hemosiderin and/or melanin.8,10
Please cite this article as: Horta-Baas G. Hiperpigmentación de la mucosa oral y discromía ungueal inducida por cloroquina. Reumatol Clin. 2018;14:177–178.


