

Osteoarthritis is a chronic joint disease; isometric exercise leads to the development of mechanical work and isokinetic exercise leads to better joint mobility.
ObjectivesTo compare the effectiveness of isometric vs isokinetic therapeutic exercises in patients with knee osteoarthritis.
Materials and methodsQuasiexperimental study in a population of 45 to 75-year-old patients with a diagnosis of knee osteoarthritis. Group 1 (experimental) was put under isokinetic exercises and group 2 (control) under isometric exercises. The sample size was of 33 patients per group; the allocation to the experimentation or control group was nonrandom, but stratified by degrees of knee osteoarthritis. The effectiveness of the exercise was measured in three dimensions: muscle strength, joint range and pain. The intervention lasted eight weeks and the physical activity was carried out every third day. The statistical analysis included averages, standard deviation, percentage, χ2 test, z test for two populations, t test for two independent populations and twin t test.
ResultsThe analysis of muscle strength comparing the categories independently demonstrates differences at 8 weeks; 33.3% of the isokinetic exercise is in the normal category and 15.2% in the isometric exercise (P=.04). There was no difference of joint range between groups, despite finding a stage I range in 100.0% of the isokinetic group and 97.0% in the isometric (P>.05) group. Pain was milder in the isokinetic exercise group at 8 weeks (P=.01).
ConclusionsIsokinetic exercises have a greater effectiveness than isometric exercises for muscle strength and pain in patients with knee osteoarthritis. However, other studies with randomized designs are needed.
En el tratamiento de la artrosis se emplea tanto el ejercicio isométrico como el ejercicio isocinético, sin embargo, no queda claro cuál de los tipos de ejercicio es más eficaz en el manejo terapéutico.
ObjetivosComparar la eficacia del ejercicio terapéutico isométrico vs ejercicio terapéutico isocinético en pacientes con artrosis de rodilla.
Material y métodosEstudio cuasiexperimental en población 45 a 75 años de edad con diagnóstico de artrosis de rodilla. El grupo 1 (experimental) sometido a ejercicios isocinético y el grupo 2 (control) sometido a ejercicios isométricos. El tamaño de la muestra fue de 33 por grupo, la asignación al grupo de experimentación o control fue no aleatoria, pero se estratificó por grados de artrosis de rodilla. La eficacia del ejercicio se midió en tres dimensiones: fuerza muscular, rango articular y dolor. La intervención tuvo una duración de ocho semanas y la actividad física se realizó cada tercer día. El análisis estadístico incluyó promedios, desviación estándar, porcentajes, prueba de chi cuadrada, prueba de z para dos poblaciones, prueba de t para dos poblaciones independientes y prueba de t pareada.
ResultadosEl análisis de la fuerza muscular comparando las categorías de forma independiente demuestra diferencia a las 8 semanas, en la categoría normal se encuentra el 33,3% del ejercicio isocinético y el 15,2% del ejercicio isométrico (p=0,04). No se encontró diferencia del rango articular entre los grupos, no obstante, el rango articular fue grado I en el 100,0% del grupo isocinético y 97,0% del isométrico (p>0,05). El dolor fue menor en el grupo de ejercicio isocinético a las 8 semanas (p=0,01).
ConclusionesEl estudio sugiere que los ejercicios isocinéticos tienen una mayor efectividad que los ejercicios isométricos para la fuerza y dolor en el paciente con artrosis de rodilla. Son necesarios más estudios que confirmen estos resultados.
Osteoarthritis is a chronic joint disease that mainly affects the knee causing significant morbidity and loss of function.1,2 Its onset is around 40 years of age and it is estimated that over 80% of people over 55 have evidence of radiographic changes in the knee due to osteoarthritis. It has been estimated that the incidence has increased by the increase in life expectancy and it has been identified as a frequent cause for health services demand in patients over 65.3,4
The clinical features of knee osteoarthritis include chronic pain accompanied by muscle weakness and joint instability, associated with physical dependence and decreased quality of life leading to sleep disturbances, depression, physical inactivity, obesity, social isolation and polypharmacy with a significant economic impact.5–8
Rehabilitation treatment is based on strengthening and isometric and isokinetic exercises aimed at reducing pain, increasing the range of motion and muscle strength, the latter being essential in the short and long terms.9–11
Isometric exercise promote the development of mechanical work and in it, the amount of force exerted is equal to the amount of resistance, so the results are slow to appear.12,13
On the other hand, isometric, isokinetic exercise promotes joint mobility, described as chondroprotective by stimulating remodeling and repair.14 In isokinetic exercise, the speed of movement is controlled, allowing a maximum contraction at constant speed across the range of motion. For example, cycling generates heat and a physiological response locally manifested in the joint as a decrease of the inflammatory process by increasing the permeability of the membrane, thereby favoring substance exchange, particularly prostaglandins, which improves pain but with no gain in muscle strength.15–17
In clinical practice, rehabilitation of the knee in osteoarthritis is based on isometric exercise; however, the objective of this study is to examine the possibility of using isokinetic exercise and compare the efficacy of therapeutic exercise against isometric isokinetic exercise therapy in patients with knee osteoarthritis.
Materials and MethodsThis is a Quasi-experimental study conducted at the Department of Physical Medicine and Rehabilitation of the Regional General Hospital of the Mexican Social Security Institute in the city of Queretaro, Mexico. The study population included patients 45–75 years of age diagnosed with knee osteoarthritis, established according to the radiographic classification of Kellgren-Lawrence (grades I, II and III).18
Two study groups were defined, 1 (experimental) with treatment with isokinetic exercises and group 2 (control) with isometric therapeutic exercises.
The study included patients with a body mass index less than or equal to 39.9, with limitation for flexion and extension, muscle strength of 3–5 according to the Lovett scale and who signed informed consent. Those excluded were diagnosed with scheduled or performed knee arthroplasty, a lower extremity fracture of less than one year, drug treatment other than paracetamol and those with neurological and heart diseases that contraindicated exercise. Patients with rheumatoid arthritis and knee injury suffered outside the exercise program were also excluded.
The sample size (n=33 per group) was calculated using formula percentages for 2 people, with confidence level of 95% (Z alpha=1.64), test power of 80% (Z beta=0.84), expected effectiveness in the isokinetic exercise group was 70% and expected effectiveness of isometric exercise group was 40%.
Using a sampling list of the Physical Rehabilitation Service morning shift outpatients as framework, patients were invited to participate in the study, and the experimental or control group assignment was not random, but stratified by grades according to the radiographic knee osteoarthritis classification (Kellgren-Lawrence18); this means that when a patient was given a grade II OA he or she was assigned to the experimental group, and the next patient with grade II osteoarthritis was assigned to the control group and so on.
The sociodemographic variables studied included weight, height, age, sex and body mass index. The effectiveness of exercise was measured in three dimensions: muscle strength, joint range and pain.
- •
Muscle strength was assessed with the Lovett scale which includes the categories zero, trace, poor, fair, good and normal.19
- •
The joint range was evaluated in relation to flexion and extension according to the degrees of mobility,20 determined by a goniometer and included the following categories:
Flexion:
Grade 0 (greater than or equal to 110°=normal).
Grade I (more than 90° but less than 110°=mild).
Grade II (more than 60° but less than 90°=moderate).
Grade III (more than 30° but less than 60°=severe).
Grade IV (less than 30°=very severe).
Extension:
Grade 0 (from 0° to −5°).
Grade I (any degree of limitation from −6°).
- •
Pain was measured with the Index of Western Ontario and McMaster Universities (WOMAC)21 which includes a scale of 0–4, considering 0 as no pain and 4 as very severe pain. The evaluation includes 5 questions so the minimum value corresponds to 0 and the maximum to 20.
0=no pain
1=mild pain
2=moderate pain
3=severe pain
4=very severe pain
The intervention lasted eight weeks and physical activity was performed every third day in both groups.
The experimental group performed isokinetic exercises.
- a)
The activity took place every other day with sessions lasting 40min.
- b)
The program included bicycling for 10min periods with 5min of rest.
- c)
The position of the seat is raised as high as possible for less knee flexion.
- d)
The resistance was gradually increased, starting with one kg and increasing 350g per week up to 3kg.
The control group performed isometric exercises.
- a.
The activity took place every other day.
- b.
Standing with the leg extended, 10 sets of 10 contractions and relaxations of the thigh with a duration of 5s each were carried out; there within 45s of rest was allowed between each set.
- c.
Sitting on the floor with two rolled towels under the thigh and toes pointing upward, the patient underwent contraction of the knee and put pressure on the back of the leg directed at the floor, a position that was maintained for 5s followed by relaxation and a return to the original position, this activity was repeated 10 times and then starting a new series on the opposite leg; between each set there was a time for rest of 45s.
- d.
Standing with the hip in abduction and the knee in flexion, with the contralateral leg in a neutral position, 10 repetitions were performed with rest between sets; this was repeated with the opposite leg.
- e.
To increase the work on the hip abductors and encourage hamstring stretching, the patient underwent ankle extension at 10°, maintained for 5s and then gently release without tilting the pelvis. This exercise was divided into two phases each reaching a different degree of elevation of the pelvis.
- f.
Standing exercises were conducted for the toes, inward and then outward for 5s and repeated 10 times, done also with the limb contralateral.
- g.
Standing with the ankle and knee in flexion, performed with hip extension to stretch the quadriceps was also carried out.
The statistical analysis included means, standard deviations, percentages, χ2 test for two populations, z and t tests for two independent populations and paired t-test.
ResultsIn the experimental group (isokinetic) there were 96.6% females, average age 59.00 years, weight 66.03kg, 153.63 cm height and body mass index of 28.00. In the control group (isometric exercise) 91.2% were female, average age 58.12 years, weight 70.12 kg, 156.79 cm height and body mass index 28.56. The comparison of these variables between groups revealed no statistically significant difference (P>.05), except in size (P=.025).
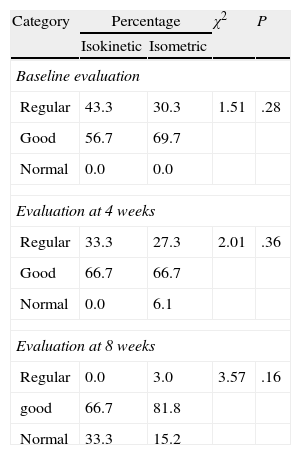
MuscleThe baseline strength was similar in both groups (P=.28), this similarity was maintained in the evaluation at 4 (P=.36) and 8 weeks (P=.16) (Table 1). However, it increased over time in both groups. At baseline, in the category of normal strength, there were no patients and at 8 weeks, the isokinetic group 33.3% reported normal strength and the isometric group 15.2% also reported normal strength.
Comparison of Strength Between Isokinetic and Isometric Groups at Baseline, 4 and 8 Weeks From the Intervention.
| Category | Percentage | χ2 | P | |
| Isokinetic | Isometric | |||
| Baseline evaluation | ||||
| Regular | 43.3 | 30.3 | 1.51 | .28 |
| Good | 56.7 | 69.7 | ||
| Normal | 0.0 | 0.0 | ||
| Evaluation at 4 weeks | ||||
| Regular | 33.3 | 27.3 | 2.01 | .36 |
| Good | 66.7 | 66.7 | ||
| Normal | 0.0 | 6.1 | ||
| Evaluation at 8 weeks | ||||
| Regular | 0.0 | 3.0 | 3.57 | .16 |
| good | 66.7 | 81.8 | ||
| Normal | 33.3 | 15.2 | ||
χ2 test.
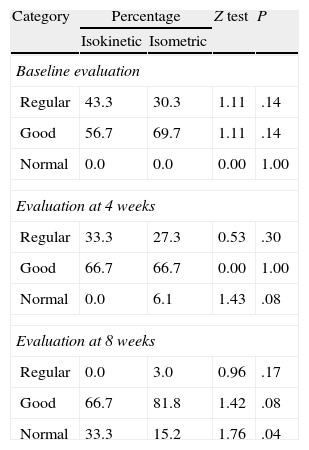
Strength analysis comparing the categories identified independently statistically significant difference in its evaluation at 8 weeks in the normal category; in this case the percentage of patients in the isokinetic exercise group was higher (33.3%) than the percentage of patients in the isometric exercise group (15.2%). Table 2 shows the results for each category.
Comparison of Strength Between the Isokinetic and Isometric Groups by Category at Baseline, 4 and 8 Weeks From the Intervention.
| Category | Percentage | Z test | P | |
| Isokinetic | Isometric | |||
| Baseline evaluation | ||||
| Regular | 43.3 | 30.3 | 1.11 | .14 |
| Good | 56.7 | 69.7 | 1.11 | .14 |
| Normal | 0.0 | 0.0 | 0.00 | 1.00 |
| Evaluation at 4 weeks | ||||
| Regular | 33.3 | 27.3 | 0.53 | .30 |
| Good | 66.7 | 66.7 | 0.00 | 1.00 |
| Normal | 0.0 | 6.1 | 1.43 | .08 |
| Evaluation at 8 weeks | ||||
| Regular | 0.0 | 3.0 | 0.96 | .17 |
| Good | 66.7 | 81.8 | 1.42 | .08 |
| Normal | 33.3 | 15.2 | 1.76 | .04 |
Z test for two populations.
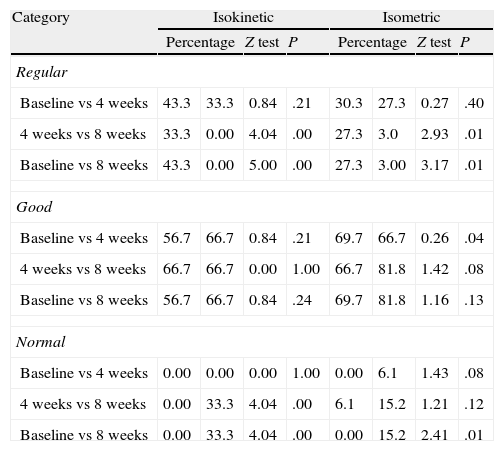
Analysis by category within the isokinetic exercise group revealed statistically significant differences between the percentage of patients with regular strength evaluated at 4 and 8 weeks and baseline and 8 weeks. This same behavior was seen for the group of isometric exercises, however, the difference was more important in the first group. When the analysis was done for the normal category in the isokinetic group, statistical differences were observed in the comparison of 4 and 8 weeks and at baseline and 8 weeks; in this case the isometric exercise group differences were present when comparing baseline and 8 weeks. Table 3 presents the information.
Comparison of Strength by Category in Each of the Groups (Isokinetic and Isometric Exercises).
| Category | Isokinetic | Isometric | ||||||
| Percentage | Z test | P | Percentage | Z test | P | |||
| Regular | ||||||||
| Baseline vs 4 weeks | 43.3 | 33.3 | 0.84 | .21 | 30.3 | 27.3 | 0.27 | .40 |
| 4 weeks vs 8 weeks | 33.3 | 0.00 | 4.04 | .00 | 27.3 | 3.0 | 2.93 | .01 |
| Baseline vs 8 weeks | 43.3 | 0.00 | 5.00 | .00 | 27.3 | 3.00 | 3.17 | .01 |
| Good | ||||||||
| Baseline vs 4 weeks | 56.7 | 66.7 | 0.84 | .21 | 69.7 | 66.7 | 0.26 | .04 |
| 4 weeks vs 8 weeks | 66.7 | 66.7 | 0.00 | 1.00 | 66.7 | 81.8 | 1.42 | .08 |
| Baseline vs 8 weeks | 56.7 | 66.7 | 0.84 | .24 | 69.7 | 81.8 | 1.16 | .13 |
| Normal | ||||||||
| Baseline vs 4 weeks | 0.00 | 0.00 | 0.00 | 1.00 | 0.00 | 6.1 | 1.43 | .08 |
| 4 weeks vs 8 weeks | 0.00 | 33.3 | 4.04 | .00 | 6.1 | 15.2 | 1.21 | .12 |
| Baseline vs 8 weeks | 0.00 | 33.3 | 4.04 | .00 | 0.00 | 15.2 | 2.41 | .01 |
Z test for two populations.
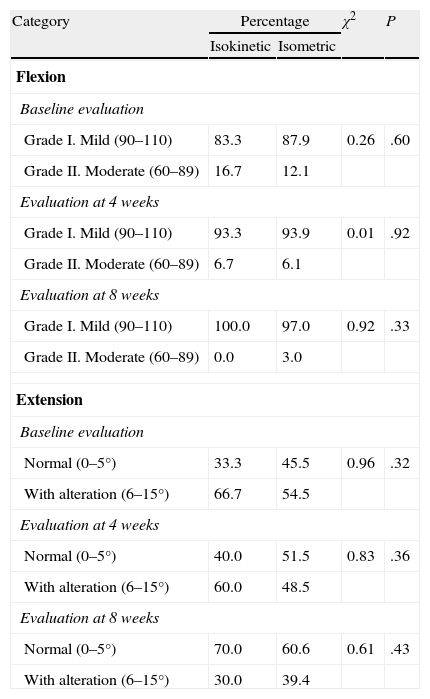
In both groups, more than 80% of patients were placed in Grade I at baseline, and the isokinetic group reached 100.0% at 8 weeks, while the isometric group reported 97.0%. However, in the three assessments (baseline, 4 weeks and 8 weeks) there were no statistically significant differences (P>.05). Table 2 presents the percentage of patients according to the degree of flexion. This same behavior was found for extension in the assessment at 8 weeks in the isokinetic exercise group, 70.0% was found in the normal category and 60.6% in the isometric exercise group, also ranking in this group (P=.43). Table 4 shows the percentage by group and classification.
Comparison of the Joint Range in Flexion and Extension Between Isokinetic and Isometric Groups at Baseline, 4 and 8 Weeks From the Intervention.
| Category | Percentage | χ2 | P | |
| Isokinetic | Isometric | |||
| Flexion | ||||
| Baseline evaluation | ||||
| Grade I. Mild (90–110) | 83.3 | 87.9 | 0.26 | .60 |
| Grade II. Moderate (60–89) | 16.7 | 12.1 | ||
| Evaluation at 4 weeks | ||||
| Grade I. Mild (90–110) | 93.3 | 93.9 | 0.01 | .92 |
| Grade II. Moderate (60–89) | 6.7 | 6.1 | ||
| Evaluation at 8 weeks | ||||
| Grade I. Mild (90–110) | 100.0 | 97.0 | 0.92 | .33 |
| Grade II. Moderate (60–89) | 0.0 | 3.0 | ||
| Extension | ||||
| Baseline evaluation | ||||
| Normal (0–5°) | 33.3 | 45.5 | 0.96 | .32 |
| With alteration (6–15°) | 66.7 | 54.5 | ||
| Evaluation at 4 weeks | ||||
| Normal (0–5°) | 40.0 | 51.5 | 0.83 | .36 |
| With alteration (6–15°) | 60.0 | 48.5 | ||
| Evaluation at 8 weeks | ||||
| Normal (0–5°) | 70.0 | 60.6 | 0.61 | .43 |
| With alteration (6–15°) | 30.0 | 39.4 | ||
χ2 test.
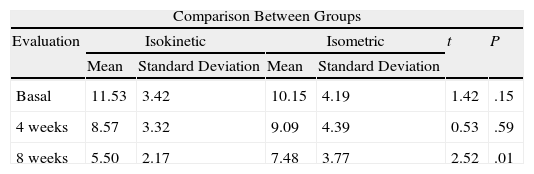
Pain was similar in both groups (isokinetic and isometric) at baseline and at 4 weeks and in the third measurement, performed at 8 weeks, there was a statistically significant difference (P=.01). Table 5 shows the values reported in each evaluation. A comparison of pain within the exercise groups demonstrated a statistically significant decrease from week 4; it was more important in the isokinetic exercise group (Table 5).
Comparison of Pain Between the Isokinetic and Isometric Groups at Baseline, 4 and 8 Weeks From the Intervention.
| Comparison Between Groups | ||||||
| Evaluation | Isokinetic | Isometric | t | P | ||
| Mean | Standard Deviation | Mean | Standard Deviation | |||
| Basal | 11.53 | 3.42 | 10.15 | 4.19 | 1.42 | .15 |
| 4 weeks | 8.57 | 3.32 | 9.09 | 4.39 | 0.53 | .59 |
| 8 weeks | 5.50 | 2.17 | 7.48 | 3.77 | 2.52 | .01 |
| Comparison in the Exercise Groups | ||||||||
| Category | Isokinetic | Isometric | ||||||
| Mean | T test | P | Mean | T test | P | |||
| Baseline vs 4 weeks | 11.53 | 8.57 | 6.51 | .00 | 10.15 | 9.09 | 2.03 | .05 |
| 4 weeks vs 8 weeks | 8.57 | 5.50 | 9.69 | .00 | 9.09 | 7.48 | 4.56 | .00 |
| Baseline vs 8 weeks | 11.53 | 5.50 | 5.46 | .00 | 10.15 | 7.48 | 5.85 | .00 |
T test for two independent populations.
T test for paired populations.
Mean is estimated on a scale from 0 to 20.
The management of osteoarthritis of the knee has evolved from the immobilization of the joint to therapeutic exercise currently recommended in clinical guidelines, without specifying a particular type of exercise, but aiming to prevent high impact exercise.22–24 In medical practice, the prescription of isometric exercises that prevent the movement of the knee is recommended; however, the possibility also exists for the performance of isokinetic exercise on a stationary bike with resistance, for the large muscle groups, together with movement of the knee. Faced with this dilemma, there is an obligation to perform an evaluation of the efficacy between the two therapeutic behaviors (isokinetic and isometric), hence the importance of this article.
The design corresponds to a quasi-experimental study; it is true that one of the characteristics of these designs is not randomization into experimental or control groups, but there is no question of its validity for demonstrating causality. In addition, the recognition that the allocation of the groups is based on stratification of the degree of osteoarthritis of the knee and the sequence of presentation of patients eliminates biases that might exist if the researcher had directly assigned patients to groups.
One of the instruments used in the study is the WOMAC index, used to assess pain, and the rest of paragraphs (B and C) evaluating the stiffness of the knee being removed since they are based on the patient's subjective perception. To evaluate stiffness, a goniometer was used for degrees of flexion and extension, as a more objective measure of joint mobility.
The purpose of exercise to ensure stability and progress of the lower extremities in the literature is reported in groups of patients undergoing rehabilitation, with improvement occurring after 4 weeks of starting the program. This behavior was also found for muscle strength and pain in the study when the analysis was performed within each group of exercises. However, the study aimed to find the difference between groups at 8 weeks into the program. What we can comment on this is that the isokinetic exercise program is an option for the management of patients with osteoarthritis of the knee, which coincides with reports in the literature.25,26,27,28
We can also say that isokinetic exercises do not have a better performance than isometric exercises regarding joint range; however, it should be clear that the purpose is not to achieve full recovery of the joint arc at all costs, but in this case to achieve functionality.
In conclusion, this study suggests that isokinetic exercises are more effective than isometric exercises for gaining strength and relieving pain in patients with knee osteoarthritis. However, it is necessary to understand that the differences found in this study are small, and there is a need for other studies with randomized designs and larger sample sizes to confirm these results.
Conflict of Interest StatementThe authors have no disclosures to make.
Please, cite this article as: Rosa UH, et al. Comparación de la eficacia ejercicio terapéutico isocinético vs isométrico en pacientes con artrosis de rodilla. Reumatol Clin. 2012;8(1):10–14.


