

Delayed diagnosis results in a worse prognosis in patients with psoriatic arthritis. Our objective is to determine the diagnostic delay, the specialties consulted and the referral points of patients with psoriatic arthritis in our environment.
Patients and methodsWe distributed a survey to members of the Spanish association Acción Psoriasis inquiring about the objectives of the study.
ResultsA total of 503 surveys were analysed. The diagnostic delay was 4.01 ± 1.42 years. The proportion of patients who had consulted, before diagnosis, primary care was 79.9%, traumatology 33.8% and the emergency department was 30.2%. The proportion of referrals that eventually led to diagnosis came from primary care in 29.3% of cases, traumatology 15.8% and the emergency department 3.5%.
Discussion and conclusionsThe delay in diagnosis far outweighs other European results. Emergency departments are an important transit point for these patients, but the proportion of referrals is very low. We believe that focusing on the importance of early diagnosis in this particular medical sector could resolve a large part of diagnostic delay.
El retraso diagnóstico condiciona un peor pronóstico en pacientes con artritis psoriásica. Nuestro objetivo es determinar el tiempo de retraso diagnóstico, las especialidades consultadas y los puntos de derivación de pacientes con artritis psoriásica en nuestro medio.
Pacientes y métodosDistribuimos una encuesta entre los miembros de la asociación española Acción Psoriasis indagando sobre los objetivos del estudio.
ResultadosSe analizaron 503 encuestas. El tiempo de retraso diagnóstico fue de 4,01 ± 1,42 años. La proporción de pacientes que habían consultado, antes del diagnóstico, con atención primaria fue del 79,9%, con traumatología, del 33,8% y por urgencias, del 30,2%. La proporción de derivaciones que finalmente condujeron al diagnóstico provinieron de atención primaria en el 29,3% de los casos, de traumatología en el 15,8% y de urgencias en el 3,5%.
Discusión y conclusionesEl retraso diagnóstico detectado supera extensamente otros resultados europeos. Los servicios de urgencias ocupan un lugar importante de tránsito de estos pacientes, sin embargo, la proporción de derivaciones es muy bajo. Entendemos que incidir en este gremio médico en particular sobre la importancia del diagnóstico precoz podría resolver gran parte del retraso diagnóstico.
Delayed diagnosis in psoriatic arthritis (PsA) is a widely recognised problem and is directly related to poorer functional prognosis of the disease.1
The Spanish Atlas de espondiloartritis axial 2017 study reported a global delayed diagnosis of spondyloarthritis of 4 years, and reported the different specialties consulted by the patients who were finally diagnosed with this group of diseases, which includes PsA. However, no break-down of data by specific type of spondyloarthritis was included.2
Due to the relationship this disease has with psoriasis, delayed diagnosis is lower to that of axial spondyloarthritis, but no specific data exist in Spain. The association of dermatologists has been the particular target of many efforts to develop early detection measures.3
A precise knowledge of the time of delay to diagnosis in PsA and the diagnostic pathway these patients follow until they are diagnosed would help to focus efforts on improving the early diagnosis of this disease.
The purpose of this study was to determine diagnostic delay, the specialties consulted prior to being referred and from where the referrals to rheumatology came from.
Material and methodsObservational, cross-sectional study based on a survey aimed at patients with PsA.
PatientsWe contacted the Acción Psoriasis association, a national patient organisation which includes people who have been diagnosed with psoriasis and PsA. The condition of the patient with PsA was a prerequisite to survey participation and was not checked up on, other than the express statement to this effect made by the participant.
The Acción Psoriasis association has an internal electronic messaging network with its members who are recognized by their diagnosis and this in turn is taken from information which each member provides when they become a member of the association.
SurveyA survey was created based on the platform Google Forms®. It was designed by a research team with help from a sociologist and 2 patients with PsA. The survey design followed the recommendations of the guide for design and performance of the surveys published by Burns et al. in 2008.4 Once it had been redacted, it was given for consideration to 6 Spanish speaking patients with PsA, who had completed secondary education and were not resident in Spain, so that observations on the survey could be obtained. These 6 patients were not linked to the Acción Psoriasis association and as they were not resident in Spain there was no probability of them having taken the survey. Their function was to adapt the questions of the survey to optimize comprehension.
The survey consisted of the following parts: 1) Presentation and authorisations, where the objectives of the survey were presented and permission was requested to use the data provided for scientific ends respecting the participant’s anonymity; 2) Demographic aspects including age, sex, educational level and autonomous community where the PsA was diagnosed; 3) Diagnostic history, where consultations of the different specialties were made, nominally and their frequency, and from where the referral to the rheumatologist occurred (here the month and year of symptom onset was included and the month and year of diagnosis), and 4) Other sections referring to disease evolution and medical control, which were not the purpose of this study.
The survey was designed in such a way that one could access it through a hyperlink sent to the electronic mail from a computer or an iOS® or Android® mobile telephone. The time required for compliance of all the parts of the survey was estimated at 15 min, and 5 min for the sections relating to this study. The strategy used to avoid duplication of surveys was to use the last 4 digits and letter from the national’s ID card or the letter and first 4 digits from the foreigner’s ID card.
Survey period and distributionThe survey was released by email in September 2018 and was open for 3 weeks. Throughout this time period 3 reminders were sent through the same system. Survey distribution was the responsibility of the patients association Acción Psoriasis, with members throughout Spanish territory, but without any homogenous distribution. We cannot therefore consider this was a random sample nor that it was necessarily representative from a geographical viewpoint.
Statistical analysisSurvey results were collected on a data processing sheet in Google Documents® and from there to a statistical processor. Numerical variables were expressed using central tendency and dispersion statistics, and nominal variables, using proportions.
ResultsSix hundred thirty-one emails were sent. The total of surveys completed and which were appropriate for analysis were 503 (79.7% response rate). Sixty two surveys were not included due to incomplete data, 10 because consent was refused and 2 because data were duplicated. In the other cases no response was obtained.
Participant characteristicsOut of the total valid surveys, 268 corresponded to male patients (51.7%) and 237 to female (45.8%). In 13 cases the sex of the participant was not stated. The average age ± standard deviation at the time of diagnosis was 48.9 ± 11.5 years. Patients came from all autonomous communities, with the most representative coming from the Community of Madrid (188), Catalonia (98), the Community of Valencia (65) and Galicia (50). With regards to education, distribution was as follows: secondary 157 (31.2%), vocational training 67 (13.3%), primary 86 (17.1%), incomplete secondary 34 (6.8%), university 93 (18.5%) and without response to question 66 (13.1%). Age at onset of symptoms was 39.5 ± 13.6 years. Mean time of delay between onset of painful symptoms and diagnosis was 4.01 ± 1.42 years. The age of the patients when diagnosed did not correlate with the delayed diagnosis time (Pearson coefficient .044, p = .328). There were no significant differences in diagnosis delay according to sex (t = .036, p = .971). The university level respondents had a delayed diagnosis of 3.44 ± 1.68 years, whilst the other levels (including omissions) had a delayed diagnosis of 4.14 ± 1.31 years (p < .001). Although the respondents were diagnosed in all the autonomous communities, there were no significant differences in the time of delay according to the place of diagnosis. In 431 patients (91.7%), the diagnosis of psoriasis preceded that of PsA.
Of the total respondents, 470 had psoriasis at the time of diagnosis (93.4%), 26 had no diagnosis of psoriasis (5.2%) and in 7 cases they did not respond to this question (1.4%).
Dividing the patients into those who were diagnosed before 2 years (37 respondents) and the remainder of patients (466), we made comparisons in accordance with the definition of recent onset PsA,5 on their epidemiological and demographic traits. All the patients diagnosed early had previously had psoriasis, whilst in the other respondents, psoriasis was present in 360 (77.2%). The age at diagnosis of the same groups was 49.1 ± 11.76 and 46.25 ± 10.87, respectively (p = .548). The proportion of males in the early diagnosis group was 63.88% and in the others it was 53.96% (p = .25). In the group with an early diagnosis, the respondents with a university education were 58.33% of cases, whilst the other respondents with a university education were 14.97% (p < .001). Out of the 37 with an early diagnosis, 10 were made in the Community of Madrid, 9 in Catalonia, 5 in the Basque country and 4 in the community of Valencia.
Diagnostic historyThe number of different specialities consulted by the patients prior to the referral where the diagnosis was made was 2.0 ± 1.0.
One hundred and seventy five respondents (34.7%) had consulted 2 different specialties, 102 (20.2%) had consulted 3 and 33 (6.5%) 4, prior to being referred to the clinician who established the diagnosis.
Diagnosis of PsA was produced by a rheumatologist in 499 cases (99.3%), by an internal medicine specialist in 3 cases (.5%) and by a dermatologist in one case (.2%).
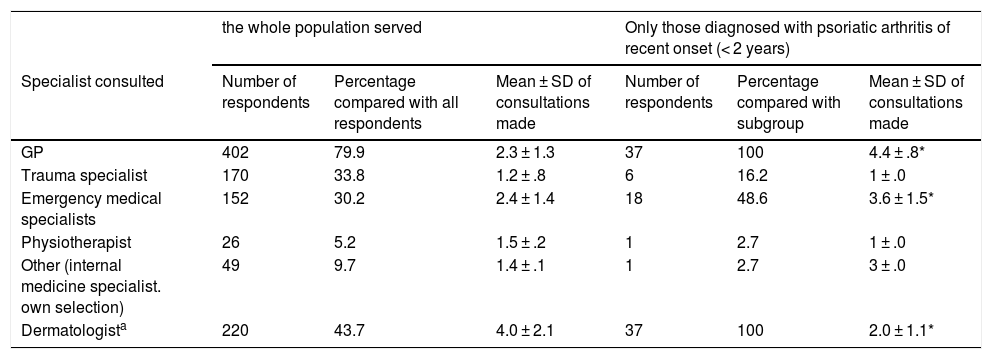
To the question “which specialists did you visit at least on one occasions due to pain which finally led to the diagnosis of psoriatic arthritis?” the responses were as follows: GP, 402 respondents (79.9%), trauma specialist, 170 respondents (33.8%), emergency department specialist, 152 respondents (30.2%). Table 1 provides a detail of the consultations to each specialty. In the group of respondents diagnosed during the first 2 years from onset of symptoms, there was a higher frequentation of primary care consultation (100% of respondents) and emergency department (48%) compared with the frequency of the diagnoses in more than 2 years (79.9%and 30.2%, respectively. The mean of consultations to these specialists was significantly higher in those who were diagnosed early: 4.4 ± .8 vs. 2.3 ± 1.3 in the case of primary care and 3.6 ± 1.5 vs. 2.4 ± 1.4 in the case of emergency department (p < .001).
Summary of the results of the consultation pathway to different specialities prior to the diagnoses of psoriatic arthritis.
| the whole population served | Only those diagnosed with psoriatic arthritis of recent onset (< 2 years) | |||||
|---|---|---|---|---|---|---|
| Specialist consulted | Number of respondents | Percentage compared with all respondents | Mean ± SD of consultations made | Number of respondents | Percentage compared with subgroup | Mean ± SD of consultations made |
| GP | 402 | 79.9 | 2.3 ± 1.3 | 37 | 100 | 4.4 ± .8* |
| Trauma specialist | 170 | 33.8 | 1.2 ± .8 | 6 | 16.2 | 1 ± .0 |
| Emergency medical specialists | 152 | 30.2 | 2.4 ± 1.4 | 18 | 48.6 | 3.6 ± 1.5* |
| Physiotherapist | 26 | 5.2 | 1.5 ± .2 | 1 | 2.7 | 1 ± .0 |
| Other (internal medicine specialist. own selection) | 49 | 9.7 | 1.4 ± .1 | 1 | 2.7 | 3 ± .0 |
| Dermatologista | 220 | 43.7 | 4.0 ± 2.1 | 37 | 100 | 2.0 ± 1.1* |
SD: Standard Deviation.
The number of respondents represents the number of subjects who declared they had consulted at least on one occasion the specialty corresponding to joint pain, except in the case of the dermatologist, where they included the consultations programmed by diagnosis or follow-up of psoriasis. The consultation mean expresses the average of the amount of times the respondent stated they had attended consultation of the corresponding specialty.
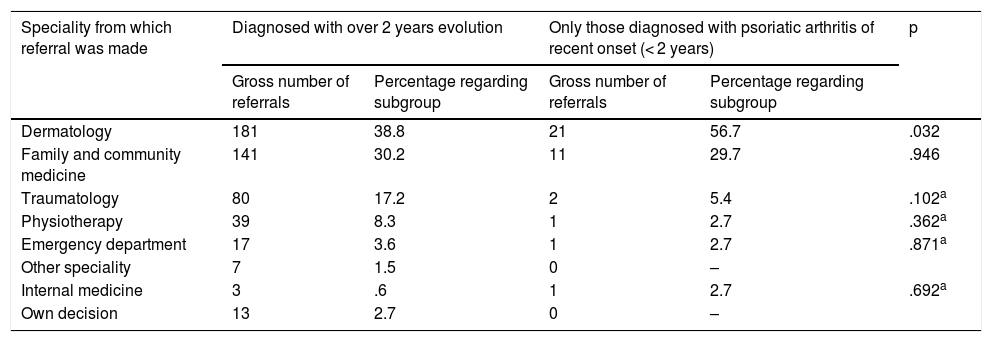
The referrals which finally led to the diagnosis of PsA came from dermatology in 202 cases (39%), primary care in 152 cases (29.3%) and the emergency services in 18 cases (3.5%). Table 2 details all the referral points recognised in the survey according to whether they were diagnosed before or after the 2 years of evolution of joint symptoms. With exception from the proportion of referrals from dermatology (38.8% of the referrals after 2 years vs. 56.7% of early referrals, p = .032), no speciality showed any statistically significant differences.
List of specialities from where the referral was made which finally led to the diagnosis of psoriatic arthritis.
| Speciality from which referral was made | Diagnosed with over 2 years evolution | Only those diagnosed with psoriatic arthritis of recent onset (< 2 years) | p | ||
|---|---|---|---|---|---|
| Gross number of referrals | Percentage regarding subgroup | Gross number of referrals | Percentage regarding subgroup | ||
| Dermatology | 181 | 38.8 | 21 | 56.7 | .032 |
| Family and community medicine | 141 | 30.2 | 11 | 29.7 | .946 |
| Traumatology | 80 | 17.2 | 2 | 5.4 | .102a |
| Physiotherapy | 39 | 8.3 | 1 | 2.7 | .362a |
| Emergency department | 17 | 3.6 | 1 | 2.7 | .871a |
| Other speciality | 7 | 1.5 | 0 | – | |
| Internal medicine | 3 | .6 | 1 | 2.7 | .692a |
| Own decision | 13 | 2.7 | 0 | – | |
We observed a delayed diagnosis of PsA of around 4 years from the onset of symptoms, less striking in the population with university studies, although without differences between sexes and not correlated with age. We also identified a high frequentation of patients, prior to PsA diagnosis, from a consultation about which there were no previous data: the emergency departments. At the same time, very poor referral had been determined of patients from these units.
Our study was based on the information obtained through a self-completion questionnaire and email distribution which was also circumscribed to an environment of subjects who were members of a specific patent association. Therefore, we cannot infer that our results are necessarily applicable to the PsA population of patients in Spain. Given that the main variable was delayed diagnosis time, the bias of memory could have played a major role in the survey, bearing in mind that respondents were asked about the month and year of symptoms onset. Other biases relating to the use of surveys, such as extreme response, social acceptance and configured characteristics, were considered when they were created to minimize them through recommended techniques of writing6,7 and the omission of questions with ordinal scales or open-ended responses.
In keeping with the Danish PsA register, delayed diagnosis of this disease in the year 2000 was of 56 months and in 2011 this fell to 3–4 months, with the change being recognition of the importance of early diagnosis.8 In a recent study in the United Kingdom a mean delay in the presentation of the patient to primary care consultation of 26 weeks was observed, together with a mean delay in time of referral to a specialist of 4 weeks.9 Indirectly, the American MAPP10 study determined a drop between the diagnosis of PsA and that of psoriasis of around 7 years, with an approximate delayed diagnosis of 5 years. In Spain, in keeping with the data from the 2017 Atlas de espondiloartritis axial, delayed diagnosis in patients with spondiyoarthritis in general (including PsA) was 8.53 years, with a median of 6 years.2 Furthermore, over half of the patients had been diagnosed with a 6 year delay and a quarter with over a 12 year delay.
The specific relationship between psoriasis and PsA has served to intensify training in ways of guiding suspected diagnoses and for early referral from the dermatologist using management guidelines, action protocols and even indications for diagnostic probability.3,11–13 However, no specific data on reduction in referral time for patients who are finally diagnosed with PsA are available. With the exception of the dermatologists, the Atlas de espondiloartritis axial in Spain reports that prior to the diagnosis of this disease, most consultations due to symptoms which finally led to the diagnosis came from primary care and trauma department consultations (88.5% and 71.6%, respectively). Although in the atlas there are no explicit details on visits to emergency departments, these appear to be included in the section on “others” (24.4%).
In one recent Spanish study it was determined that 14% of all emergency diagnoses are related to the musculoskeletal system and that 20% of them consulted due to axial pain.14 It is therefore not surprising that these units are attended by patients who in a future will be diagnosed with spondyloarthritis.
It is of note that there is no other study in which patients who attend emergency departments have been specifically questioned as to why, and therefore we were unable to establish any comparisons.
Other findings of interest in our study are as follows: for one part, the relatively large proportion of early diagnoses in the group of respondents with university education compared with the other respondents and the distribution of these patients mainly in larger cities in Spain. The socioeconomic level, access to health and academic level of the population has demonstrated an association with the diagnosis of early rheumatoid arthritis and with the severity of its activity in previous studies.15–17 Although our survey was not designed to discriminate between levels of access to different degrees of healthcare complexity, the results exposed seem to be in line with the trend towards early PsA diagnosis in more educated population groups and who those residing in cities.
ConclusionsOur study outlines 2 problems to be highlighted in the PsA diagnosis: for the one part, delayed diagnoses which widely exceeds that estimated in the Danish DANBIO register and is positioned around that reported by the American MAPP survey; and on the other, the idea that in our emergency departments there is a large medical group whom patients who are finally diagnosed with PsA have previously consulted and from whom very few referrals are made.
The determination of a medical group which is highly consulted and from which very little referral is made flags up the need to direct concerted efforts to training, similar to those directed at primary care and dermatology, with the purpose of aiding referral and early diagnosis.
Conflict of interestsThe authors have no confliction interests to declare.
Please cite this article as: Guillen Astete CA, Gaite Gonzalez I, Zurita Prada PA, Urrego Laurin C. Retraso y recorrido diagnóstico de pacientes con artritis psoriásica en España. Reumatol Clin. 2021;17:525–529.


