

To assess the relationship between muscle strength (Jama), and pain (VAS) levels with hand function (DASH) in patients with trapeziometacarpal osteoarthritis.
Cross-sectional study.
ParticipantsSample of 72 patients with osteoarthritis stage 2–3 (Eaton) and trapeziometacarpal osteoarthritis. Patients were recruited when they came to the Hand Surgery Unit.
MethodGrip strength, pinch, pain and hand function were measured, and correlation and regression coefficients between them were obtained.
ResultsFor function, the most significant model (R2=0.83) included pain and strength. But it is tip to tip pinch force which has a stronger relationship with DASH (standardized B: −57) questionnaire. Pain also influenced strength measured with the dynamometer but it was tip to tip pinch force that was the most affected.
ConclusionsFindings confirm that there is a significant correlation between function referred by the patient and variables that can be measured in the clinic such as grip strength and pinch. The correlation between pain intensity and function was also significant, but tip to tip pinch strength had the greatest impact on the function.
Establecer una posible relación entre la fuerza (Jamar), el dolor (EVA) y la capacidad funcional referida por el paciente (DASH) determinando en qué grado influyen unas en otras.
Estudio observacional transversal analítico.
ParticipantesMuestra de 72 pacientes que presentaban una artrosis trapecio metacarpiana grado 2-3 de Eaton. Los pacientes fueron reclutados cuando acudían a la Unidad de Cirugía de mano.
MétodoSe realizaron mediciones de fuerza de agarre, pinza, valoración del dolor y funcionalidad, y se establecieron las correlaciones entre cada una de ellas.
ResultadosEl modelo más significativo para la función (R2 =0.83) incluye la variable dolor y la fuerza. Pero es la fuerza punta contra punta la que presenta una mayor correlación con el cuestionario DASH (B-estandarizado: –57). Respecto al dolor, influye en todas las mediciones de fuerza realizadas con el dinamómetro, siendo también la fuerza de la pinza punta contra punta la que presenta una mayor correlación.
ConclusionesLos hallazgos corroboran que existe una correlación significativa entre la función referida por el paciente y variables que podemos medir en consulta, como la fuerza del puño y la pinza. Pero también esta correlación es significativa entre las variables función y dolor entre sí, pero es la pinza punta contra punta la que presenta una mayor asociación con el cuestionario DASH.
In the treatment of degenerative pathologies, where injuries evolution and treatment are prolonged in time, it is important to evaluate the results both quantitatively and qualitatively.
The thumb is key in the grasping function of the hand. Opposition is the most important kind of grasping function and it occurs in the trapeziometacarpal joint.
In trapeziometacarpal osteoarthritis, there is an anatomic and a functional component related to the performance of patients in their daily activities. Pain, rigidity and weakness are causes that reduce physical function,1–4 but the extent of influence of each of them is unknown.
Pain is the main reason why patients go to the doctor's office and the most influential factor that hinders the performance of daily tasks and activities requiring the opposition of the thumb.2 With good reason, pain reduction is the main objective in the treatment of trapeziometacarpal osteoarthritis in numerous studies,1,2,5 and it is defined as the most influential factor in function reduction. Regarding strength, numerous publications use the values of key pinch as a reference to assess postoperative success,6–8 but they do not determine the causes for which this pinch and not any other pinch is used, or if there are correlations between strength improvement and other variables such as, for example, functionality referred by the patient.
Pain and functionality could be summarized in only one concept: patient satisfaction. However, although the level of satisfaction referred by the patient could be influenced by environmental, social and occupational factors,3 the degree of pain and functional capacity could have an influence on the patient's satisfaction level, but the extent is unknown.
Based on consulted publications, we start from the hypothesis that pain intensity would be closely related to the dysfunction level perceived by the patient, but we are not aware of the influence on functionality of other clinical variables, such as grip strength or pinch, and the extent of influence of each of them, to establish objectives in the treatment of patients directly focused on the improvement of patient's function, and consequently, life quality.
The objective of this study was to assess the association degree among strength, pain and functional capacity in patients with stage 2–3 trapeziometacarpal osteoarthritis, as per Eaton's classification.
Materials and MethodsSample SelectionThe study was carried out with patients that visit the Hand Surgery Unit in Centro Tecan. After the X-ray control, those subjects diagnosed with Eaton9 stage 2 and 3 trapeziometacarpal osteoarthritis were derived to the Hand Therapy Unit in such Centre with a previously set appointment. Assessments were performed between June and December 2013.
The Principal Investigator, a hand therapist with more than 13 years of experience, carried out the assessments. Variables included in the study were: grip strength (kg), pinch force (kg), pain assessment (Visual Analogue Scale [VAS]) and function assessment with DASH10 Scale.
The sample contained 72 patients (59 women and 13 men) aged between 39 and 80 years old (mean±standard deviation, 59.97±8.36).
As no intervention is performed on the patients, the study approval by an Ethics Committee was deemed not necessary. It was indeed explained to patients that their data would be anonymously used for a study and they were provided with the Data Use Informed Consent Form.
Sample Selection CriteriaTarget population: old patients diagnosed with Eaton9 stage 2 and 3 trapeziometacarpal osteoarthritis. Patients with previous injuries in the same hand, that had associated pathologies, such as tenosynovitis or Dupuytren's disease, were excluded if they had been subject to surgical intervention in that hand or had been infiltrated for that reason during the last 6 months.
Study DesignAnalytical cross-sectional observational study.
ProcedureAssessments were always performed by the same assessor. In all cases, we followed the recommendations of the American Society of Hand Therapists,11 both in the patient's position and in the procedure.
We used the Jamar hydraulic hand dynamometer (position 2) to measure the grip strength and the pinch dynamometer for thumb opposition.12 In both cases, we obtained 3 measures and took as reference the mean of the 3 measurements.
Pain measurement was carried out with the universal scale, VAS, developed by Huskisson in 1974. The patient was asked to define the pain felt during the execution of daily activities, such as brushing his teeth, cooking, driving, etc.
To assess the function, we used the Spanish version of DASH13 questionnaire, strictly following the instructions of the authors. The questionnaire was provided to the patients once their personal data were filled on their medical record and before the muscular assessment was performed.
DASH InstrumentThe DASH was developed by the American Academy of Orthopaedic Surgeons and the Institute for Work and Health, Canada, to measure disability and symptoms related to the upper limbs and their musculoskeletal conditions; it is available in 27 languages.10 It is made up of a 30-items questionnaire, scored from 1 to 5. The greatest possible score is 100 and the minimum possible score is 30. Raw score is converted in a 0 to 100 scale, where 0 reflects the lack of disability (good functioning) and 100 reflects the highest level of disability (bad functioning).
If more than 10% of the items (3 questions) are not answered, it is not possible to estimate the DASH final score.
The clinimetric characteristics of the Spanish adapted version were studied first by Rosales et al.13 and subsequently by Hervás et al.,14 with a high test–retest reliability and internal consistency in both cases.
Pain AssessmentMusculoskeletal pain, more specifically its intensity, is generally measured by VAS.15 The VAS consists of a 100mm horizontal line, where the subject must make a vertical line cut reflecting his current situation between the point located closer to his left (no pain at all) and the point located closer to his right (highest unimaginable pain).
The VAS has well-established psychometric properties,15,16 is validated17 and reliable and sensitive to pain intensity changes.9,18,19
Statistical Treatment of DataThe analysis was focused on the search of significant correlations among pain clinical variables, physical disability degree and muscular strength.
The sample normality was confirmed through the Kolmogorov–Smirnov test.
Descriptive statistics was performed with measures of central tendency and dispersion of the study variables, and Pearson correlation coefficients were used for parametric samples. Correlation analyses were performed on pain and strength variables and DASH questionnaire results.
Subsequently, the associative value of the study variables was studied through several regression analyses to explain the DASH questionnaire. We used the “step to step” (Stepwise) procedure to search among all the possible explanatory variables those that better and more completely explain the dependent variable providing none of them is a lineal combination of the remaining ones. For the inclusion of variables in the model, probability had to be <0.5. We established the interpretation of the correlation coefficients as per Cohen: r<0.39 low relation; 0.4<r<0.69 moderate relation and r>0.7 high relation.16
The significance level was established at P=.05. Analyses were carried out with SPSS software for Windows, version 20.
ResultsThe sample contained 72 patients (59 women and 13 men) aged between 39 and 80 years old (mean±standard deviation, 59.97±8.36).
Table 1 shows a positive relation among the strength variables, where we can observe a positive correlation among all of them, but with a P value <.01 among the strength of the 3 kinds of pinch.
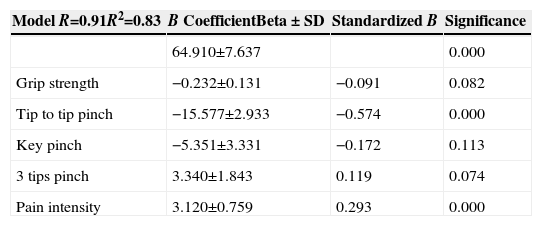
Model With DASH Questionnaire as Dependant Variable and Including the Functional Variables of Strength, Grip, Pinch and Pain Intensity.
| Model R=0.91R2=0.83 | B CoefficientBeta±SD | Standardized B | Significance |
|---|---|---|---|
| 64.910±7.637 | 0.000 | ||
| Grip strength | −0.232±0.131 | −0.091 | 0.082 |
| Tip to tip pinch | −15.577±2.933 | −0.574 | 0.000 |
| Key pinch | −5.351±3.331 | −0.172 | 0.113 |
| 3 tips pinch | 3.340±1.843 | 0.119 | 0.074 |
| Pain intensity | 3.120±0.759 | 0.293 | 0.000 |
Regarding the relation between pain intensity and the strength we measure with the dynamometers in practice, Pearson's bivariate correlation shows a negative correlation. The more intense the pain referred by the patient, the less strength reflected in the dynamometer. But the worst results in terms of strength at the same pain intensity are offered by the tip to tip pinch (P=−0.706).
If we consider all the variables, those answered by the patient himself in a questionnaire, the DASH in this case, and the ones we obtain through measurement tools, such as VAS and dynamometers, we prove that the functional capacity referred by the patient presents a negative association with all the variables of the study; this correlation is significant with P<.05 for the hand grip strength. The most significant association degree (P<.01) is found among the function and the pain variables and all the variables that measure strength, being the tip to tip pinch force the one that shows a greater negative association with the functionality degree referred by the patient (−0.880).
In the first regression analysis, we used the dysfunction degree measured by the DASH questionnaire as dependent variable. The functional variables of strength, grip and pinch and the pain variable, measured with the VAS scale, were included. This analysis results in R=0.91 and R2=0.83. The analysis contributes by 83% in the patient's dysfunction degree with a level of significance of P<.001.
By observing the contribution degree of each of the variables to the model, we can see how tip to tip pinch force with a standardized B −0.57 (P=.00) and pain intensity with a standardized B −0.29 (P=.00) significantly contribute to the analysis.
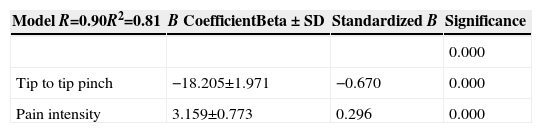
We performed a second regression analysis where, keeping the result of DASH questionnaire as dependent variable, tip to tip pinch force and pain intensity were used as predicting variables. Results show R=0.90 and R2=0.81 (Table 2). These 2 variables represent 81% of the results of the DASH questionnaire by themselves. Tip to tip pinch shows a standardized B coefficient=0.67, and pain intensity measured with the VAS scale shows a standardized B coefficient=−0.29.
Model With DASH Questionnaire as Dependant Variable and Including the Functional Variables of Tip to tip Pinch Force and Pain Intensity.
| Model R=0.90R2=0.81 | B CoefficientBeta±SD | Standardized B | Significance |
|---|---|---|---|
| 0.000 | |||
| Tip to tip pinch | −18.205±1.971 | −0.670 | 0.000 |
| Pain intensity | 3.159±0.773 | 0.296 | 0.000 |
The findings prove there is a significant correlation between the function referred by the patient and the variables we can measure in practice, such as fist and pinch strength. But this correlation is significant also between the variables function and pain, i.e., between the DASH result and the VAS scale, or in other words, there is a significant high correlation between pain and dysfunction. We have found a significant correlation (Pearson coefficient) between pain and the results obtained in the DASH questionnaire. These 2 variables are strongly related in trapeziometacarpal osteoarthritis. The greater the pain, the greater the disability referred by the patient. This justifies the conclusions of MacDermid et al.12 study, where it was confirmed that one of the main objectives in the treatment was pain reduction, as this was the most influential variable in the dysfunction of patients.
Other studies providing similar evidence in relation to pain include Wajon and Ada,2 Rogers and Wilder,20 Garfinkel et al.,21 Boustedt et al.,22 Thiele et al.,23 Weiss and Lasayo,24 Day et al.25 and Michlovitz et al.5
Among the studies consulted, those carried out by Kadzielski et al.26 and MacDermid et al.,27 and those of Goldfarb and Stern28 show a high significance level (P<.001) between function and pain. Barthel et al.29 also established a relation between pain reduction and the functional variables, determining that pain reduction improved physical function in general and strength. Besides, Bijsterbosch et al.30 developed a study to determine the possible impact of pain at the metacarpophalangeal and interphalangeal level in osteoarthritis and dysfunction. As in our study, their conclusion was that pain was the most influential factor in dysfunction; however, even if it implies the use of the thumb, the studied pathology is not the target of our study.
Regarding strength improvement, based on our results, we can confirm that there is a significant correlation among all the strength variables. This correlation is positive among the grip strength and the 3 kinds of pinch, being high between the tip to tip pinch, 3 tips and key pinch. But in the multiple regression analysis, tip to tip pinch force is the only strength variable that shows a significant association in the analysis, where the DASH was used as dependant variable. There are numerous published studies where key pinch instead of tip to tip pinch is used as the result variable in functional improvement to assess the success of certain surgical interventions, possibly under the belief that key pinch is the most commonly used by the patient during daily activities.6–8 We cannot establish a relation between the results in these studies and our results as they use a different measurement tool and the key pinch variable as a tool to improve the patients function after the surgical intervention, without considering other variables that could possibly influence the function, such as pain. They neither justify why they use the key pinch instead of any other type of pinch to establish the patient's improvement.
Other authors have found in their studies relations of many clinical and functional variables among each other. Bain et al.,31 Mandl et al.,32 Goldfarb and Goldfarb28 or MacDermid et al.27 established a relation among the patient's strength, joint range and dysfunction level but with a great variety in correlation coefficients ranging from 0.11 to 0.71 for strength and 0.19 to 0.6 for joint range. We have not found studies stating a relation between function and joint range in patients with osteoarthritis at the trapeziometacarpal level, so we have not included this variable in our study.
Based on the results derived from this study, we could conclude that the objectives of the conservative treatment should be focused on searching for strategies to improve hand pain with Eaton stage 2–3 trapeziometacarpal osteoarthritis, aiming at improving the function with the strength work and paying special attention to tip to tip pinch force. Besides, in our clinical practice, assessing pain intensity and measuring tip to tip pinch force, we could have an idea of the dysfunction level of the patient without having to complete a self-questionnaire, which sometimes could be filled incorrectly due to comprehension difficulties or personal interests of the patient.
However, these conclusions shall be taken under consideration due to the limitations of the study. On the one hand, the measurement was taken only once per patient, which makes the results less valid. These preliminary results could be applicable if future research lines studied the effect they might have on the study variables, especially on function, tip to tip pinch work and pain reduction. On the other hand, we must consider the possible selection bias during sampling, as patients were selected when they went at the doctor's office with pain on the base of the thumb and only one Investigator determined if they met the inclusion criteria for the study.
The results of this preliminary study give us an idea of the “key points” to assess in a patient with Eaton stage 2 or 3 trapeziometacarpal osteoarthritis before and after treatment to better simplify and objectify our daily clinical practice. However, it will be necessary to carry out subsequent studies to extrapolate these results to the entire population presenting this degenerative pathology in the thumb base. Control/cohort case studies would help us to determine if working on the pinch force and pain intensity variables, the patient's functionality and, consequently, life quality improve.
Ethical ResponsibilitiesProtection of persons and animalsAuthors state that the proceedings followed conformed to the ethical standards of the Responsible Committee on Human Experimentation and according to the World Medical Association and the Declaration of Helsinki.
Data confidentialityAuthors declare that they have complied with the site protocols about the publication of patient data.
Right to privacy and informed consentAuthors have obtained the informed consent from the patients and/or subjects referred to in the article. This document is in possession of the corresponding author.
Conflict of InterestNo conflicts of interest are declared.
We thank Dr. Miguel Cuadros for his support and collaboration in this work.
Please cite this article as: Cantero-Téllez R, Martín-Valero R, Cuesta-Vargas A. Contribución de la fuerza y el dolor en la función del paciente con artrosis trapecio metacarpiana. Estudio transversal. Reumatol Clin. 2015;11:340–344.


