



The increasingly widespread off-label use of anti-tumor necrosis factor alpha (TNF-α) drugs has changed the therapeutic panorama of uveitis when topical or systemic treatment with corticosteroids and classic immunosuppressive drugs failed to control the disease.
Certolizumab pegol is an anti-TNF-α drug approved by the FDA for use in Crohn's disease in 2008, and for rheumatoid arthritis by the EMEA and FDA in 2009. Recently, a series of 7 cases of uveitis treated with certolizumab pegol was published. This is one of them.1
The case is a 33-year-old patient affected since 2003 by recurring episodes of acute alternating unilateral anterior uveitis and HLA-B27 positive spondyloarthropathy, the reason for which he was in treatment with infliximab at doses of 3mg/kg/body weight every eight weeks. Until 2004, he had suffered recurrent episodes of acute alternating unilateral anterior uveitis which came to be controlled with topical steroids. During this year the pattern of ocular involvement was changing, with anterior uveitis episodes becoming more frequent and associated with bilateral episcleritis/scleritis, while presenting the onset of digestive symptoms, being diagnosed with Crohn's disease after a colonoscopy and biopsy. Treatment was established, therefore, with oral prednisone azathioprine and infliximab and dosages increased to 5mg/kg/body weight every 6 weeks. In 2010 recurring ocular and intestinal flares lead to a change of anti-TNF drug to adalimumab 40mg weekly. After initial control, the patient presented a flare of uveitis and ileitis after one year. In October 2011 the uveitis unit switches the patient to a third anti-TNF drug, certolizumab pegol 400mg initial dose and 200mg every 2 weeks for maintenance, with negative Tyndall result and resolution of synechiae from the second dose, but without resolution of intestinal manifestations. He is admitted for an ileal resection surgery in January 2012. The biological treatment was suspended due to the surgery and the patient presents a severe flare of uveitis in the right eye (AV 0.5, synechiae, Tyndall 3+). The patient is treated with oral and topical corticosteroids. After surgery in February 2012, treatment with certolizumab pegol and azathioprine is resumed. The patient is currently inactive with good visual acuity (VA 1.0) and no flares up until March 2014 when a flare of unilateral uveitis which was controlled with topical treatment (Table 1).
Pattern of Uveitis and Treatments Received.
| 2003–2010 | 2010–2011 | 2012–2014 | |
|---|---|---|---|
| Uveitis pattern | URAAU | CAU | CAU |
| Anti-TNF-α | Infliximab | Adalimumab | Certolizumab |
| Immunosuppressive therapy | Azathioprine | Azathioprine | Azathioprine |
| Adjuvant treatment | Periocular infiltration oral corticosteroids | Periocular injections oral corticosteroids | Ileal resection |
URAAU, unilateral recurrent acute anterior uveitis; CAU, chronic anterior uveitis.
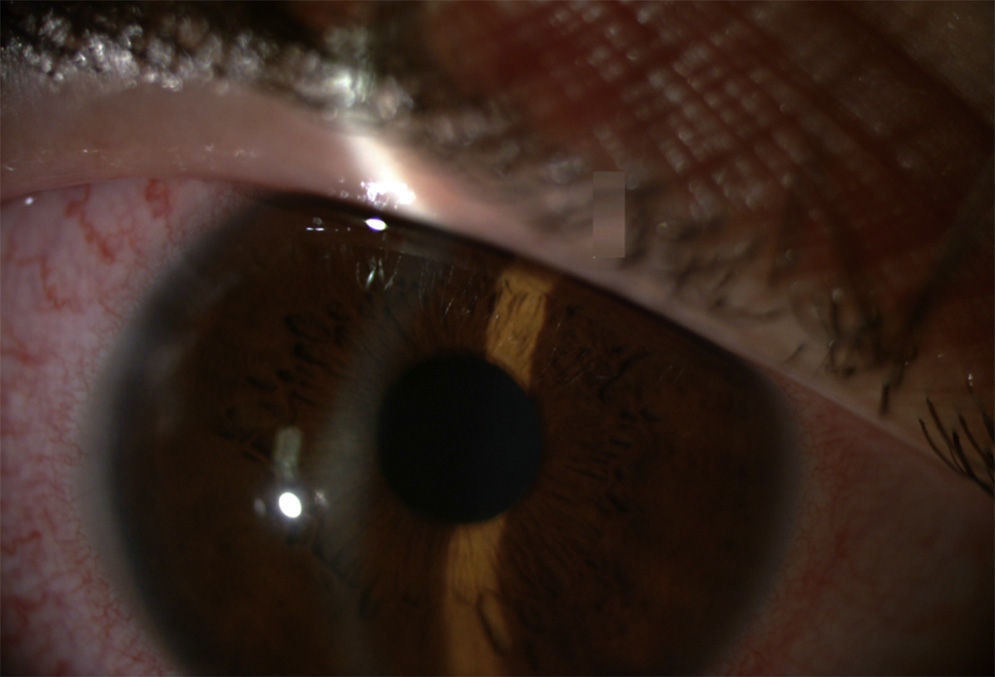
In some cases of anterior uveitis associated with spondyloarthropathies, systemic treatment is necessary to control inflammatory activity and flares (Fig. 1). Uveitis associated with Crohn's disease has somewhat different characteristics, leading to a more chronic form, sometimes more aggressive, and even middle and posterior eye involvement, unlike uveitis associated with ankylosing spondylitis.2 Among classical immunosuppressants used for treating anterior uveitis the literature suggests methotrexate3,4 and sulfasalazine as effective5 as well as anti-TNF-α drugs. However, due to high cost and off-label use, they are used as second line therapy. There are papers describing case series and isolated cases of patients with anterior uveitis treated with anti-TNF-α.6–9 Certolizumab Pegol is a pegylated anti-TNF drug without an Fc fragment. PEGylation involves the addition of polyethylene glycol as a ‘transporter’, which gives advantages from the pharmacokinetic point of view.10,11 This could explain its effectiveness when other anti-TNF drugs have failed.
Uveitis is a condition that can have serious consequences. Therefore, the capacity to use a new drug for treatment is very encouraging. Although studies are needed to confirm efficacy and safety, the therapeutic response in this patient suggests that certolizumab pegol could be an effective therapeutic alternative for these patients.
Please cite this article as: Maiz Alonso O, Blanco Esteban AC, Egües Dubuc CA, Martinez Zabalegui D. Efectividad del certolizumab pegol en el tratamiento de la uveítis anterior crónica asociada a enfermedad de Crohn y espondilitis anquilosante. Reumatol Clin. 2015;11:189–190.


