

Osteoarthritis (OA) is the most prevalent rheumatic disease in Mexico. Treatment involves pharmacological and non-pharmacological strategies.
ObjectiveTo describe the factors associated with treatment of osteoarthritis in the urban and rural population of Nuevo León.
MethodsAnalysis of a cross-sectional study of patients with OA from a COPCORD study database. Univariate and multivariate analyses of the variables associated with treatment of OA.
ResultsWe included 696 patients with OA with an average age of 58 years (SD 14.1), 484 (69.5%) women. Pain with a visual analog scale (VAS) ≥4 was present in 507 (72.8%) patients. Functional disability was present in 133 (19%) patients and a mean HAQ of 0.37 (IQR 0.75) was found. The most frequent place of OA was knee in 356 (51.1%) patients; 259 (37%) patients already knew their diagnosis. The most employed treatments were non-steroidal anti-inflammatory drugs (289 patients, 58.5%). The variables associated with treatment were age >58 years (OR 1.3, 95% CI 1.0–1.5), female gender (OR 1.17, 95% CI 1.0–1.3), VAS pain ≥4 (OR 1.3, 95% CI 1.1–1.4), functional disability (OR 2.6, 95% CI 1.6–4.1), HAQ >0.375 (OR 1.9, 95% CI 1.5–2.4), and past diagnosis of OA (OR 5.1, 95% CI 3.3–8.0). In the multivariate analysis, VAS pain ≥4 (OR 1.9, 95% CI 1.2–2.8), kneeling disability (OR 3.15, 95% CI 1.3–7.4) and previous diagnosis of OA (OR 7.6, 95% CI 4.5–12.9) had statistical significance.
Conclusionfactors associated with treatment of OA are VAS pain ≥4, kneeling disability and previous diagnosis of OA.
La osteoartritis (OA) es la enfermedad reumática más prevalente en México. El tratamiento involucra intervenciones farmacológicas y no farmacológicas.
ObjetivoDescribir los factores asociados al tratamiento de osteoartritis en comunidades urbanas y rurales de Nuevo León.
MétodosEstudio transversal analítico de pacientes con OA, obtenido de la base de datos del estudio COPCORD. Análisis univariado y multivariado de las variables asociadas al uso de tratamiento.
ResultadosSe incluyó a 696 pacientes, edad media ± desviación estándar de 58 ± 14,1 años, 484 (69.5%) mujeres. El dolor con intensidad ≥ 4 en escala visual analógica (EVA) se presentó en 507 (72,8%) individuos. En 133 (19%) individuos se presentó limitación física, con una mediana en HAQ de 0,37 (RIQ 0,75). La localización más frecuente de OA fue rodilla en 356 (51,1%) pacientes; 259 (37%) individuos ya tenían el diagnóstico de OA. El tratamiento más empleado fueron los antiinflamatorios no esteroideos en 289 (58,5%) individuos. Las variables asociadas al uso de tratamiento fueron edad >58 años (OR = 1,3, IC del 95%, 1,0-1,5), género femenino (OR = 1,1, IC del 95%, 1,0-1,3), dolor con EVA ≥ 4 (OR = 1,3, IC del 95%, 1,1-1,4), limitación fisica (OR = 2,6, IC del 95%, 1,6-4,1), HAQ >0,375 (OR = 1,9, IC del 95%, 1,5-2,4) y antecedente de diagnóstico de OA (OR = 5,1, IC del 95%, 3,3-8,0). En el multivariado, el dolor con EVA ≥ 4 (OR = 1,9, IC del 95%, 1,2-2,8), la incapacidad para arrodillarse (OR = 3,1, IC del 95%, 1,3-7,4) y el antecedente de diagnóstico de OA (OR = 7,6, IC del 95%, 4,5-12,9) permanecieron significativos.
ConclusiónLos factores asociados al tratamiento de OA son EVA del dolor ≥ 4, la incapacidad para arrodillarse y el antecedente de diagnóstico de OA.
Osteoarthritis (OA) is a chronic, degenerative disease characterized by progressive loss of joint cartilage. It is the most common form of arthritis and causes pain, inflammation and joint damage. It can affect one or several joints or become generalized. Age of onset, affected joints and progression vary within each person and also according to the anatomical location.1
Prevalence depends on the employed definition for OA, age, gender and geographical location. Worldwide, approximately 10% of the population ≥60 years old have OA symptoms.2 In a COPCORD study of 5 regions in Mexico, the prevalence was 10.5%, while in the region of Nuevo León it was 17.3% (95% CI 16.2–18.4).3,4 It is more common in women and affects up to 80% of people >75 years.2
OA is the disease of the musculoskeletal system that causes more functional disability. The limitation and resulting functional impairment depend on the anatomical location, severity and, among other factors, of the daily activities and the professional and recreational individual needs.1
Treatment involves pharmacological and non-pharmacological strategies. Patient education about exercises and daily life activities, physiotherapy and/or occupational therapy, along with the use of analgesics are important.5 First line treatment involves acetaminophen and topical analgesics (i.e. Capsaicin), while non-steroidal anti-inflammatory drugs (NSAIDS) are recommended as second line options.6
The core treatment for OA, a combination of pharmacological and non-pharmacological treatment modalities, is mainly performed in primary care and although several clinical practice guidelines exist, diagnostic procedures, referrals, and use of treatment modalities observed in primary care tend to be inadequate.7 In a recent review that assesses the quality of care using quality indicators from or based on Assessing Care Of Vulnerable Elderly (ACOVE), the reported quality of care is still relatively low for OA (interquartile range 29–41%).8
The expense of treatment and the related work loss represent a significant economic burden.9 In our population, the factors associated with the treatment of OA are not known.
Being OA the most frequent joint disease and because of the functional disability it causes, we aimed to describe which are the most employed therapeutic resources and their associated factors in our population.
MethodsWe performed a secondary analysis of the database coming from the Community Oriented Program for the Control of Rheumatic Diseases (COPCORD) Study (previously published).4 Briefly, this was a cross-sectional, phase I COPCORD study of an adult population ≥18 years, conducted between August 2008 and June 2009 on a representative sample of the State of Nuevo León, México. The COPCORD questionnaire10 was employed to identify patients who reported having either current (last 7 days) or past musculoskeletal pain (MSK), not related with trauma and with a Visual Analog Scale (VAS) ≥1 to be considered for medical examination. Subjects with a suspected rheumatic disease were evaluated in the community by certified rheumatologists to establish a clinical diagnosis. For the detection of OA and using the criteria of MSK pain with a VAS ≥1, the COPCORD questionnaire has a sensitivity of 51.8% and specificity of 78%.11
Out of 4713 participants who completed the COPCORD questionnaire, 2634 participants referred non-traumatic MSK pain. Eight hundred and fifteen met the clinical diagnosis of OA, out of which 696 (14.8%) patients had information about the anatomical location of OA and were chosen for analysis.
The considered variables, which were acquired from the COPCORD questionnaire, were the socio-demographic characteristics, self-reported comorbidities (diabetes mellitus, arterial hypertension, dyspepsia, hyperlipidemia, varicose veins, obesity, cardiac disease, depression, anxiety, tabaquism and alcoholism) and employment according to the National Institute of Statistics and Geography (INEGI) classification; characteristics of current and past pain, affected body parts and a total VAS pain on a 0–10 scale; functional capacity including the presence of disability, adaptation and Health Assessment Questionnaire (HAQ); diagnosis and anatomical location of OA; type, number and prescriber of the employed treatments. Additionally, a cutoff of pain on VAS ≥4 was also considered for analysis, according to a previous report of patients with symptomatic OA and current or past disability.10
Statistical analysisOf the considered variables, a descriptive analysis was performed. Continuous variables were reported as average and standard deviation or means and interquartile range, depending on distribution, with a previous testing for normality (Kolmogorov–Smirnov test). Categorical variables were reported as frequencies and percentages.
For the univariate analysis, the population was divided between those who did and those who did not received treatment and all the mentioned variables were analyzed. To establish statistical significance, the student t test or the Mann Whitney U test were used for the continuous variables. For categorical variables, contingency 2×2 tables and chi-square test were performed, likewise, odds ratio and 95% confidence intervals were made.
For the multivariate analysis, a regression logistic analysis of all the variables with statistical significance was performed, considering statistical significance p<0.05. Statistical package SPSS 20 was used.
The Ethics Committee of the Hospital Universitario “Dr. José Eleuterio González” of the University of Nuevo León approved the protocol, registry RE13-012. According to local regulations, a post hoc analysis does not require specific authorization.
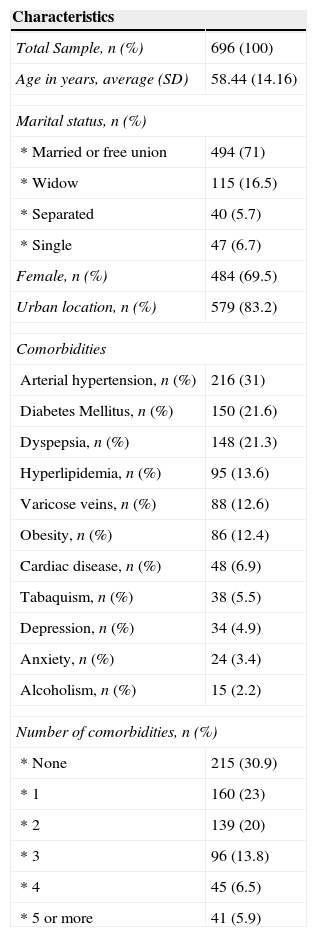
ResultsSix hundred ninety six patients were included, with an average age of 58 years (SD 14.1), 484 (69.5%) were women, 579 (83.2%) patients were living in urban areas and 494 (71%) reported being married or cohabitating, 115 (16.5%) widow, 40 (5.7%) separated and 47 (6.7%) were single.
Four hundred eighty one (70%) had any comorbidity, being arterial hypertension the most frequent in 216 (31%) patients, followed by diabetes mellitus in 150 (21.6%) and dyspepsia in 148 (21.3%) patients. Almost half of the patients had two or more comorbidities (Table 1).
Baseline demographic characteristics.
| Characteristics | |
|---|---|
| Total Sample, n (%) | 696 (100) |
| Age in years, average (SD) | 58.44 (14.16) |
| Marital status, n (%) | |
| * Married or free union | 494 (71) |
| * Widow | 115 (16.5) |
| * Separated | 40 (5.7) |
| * Single | 47 (6.7) |
| Female, n (%) | 484 (69.5) |
| Urban location, n (%) | 579 (83.2) |
| Comorbidities | |
| Arterial hypertension, n (%) | 216 (31) |
| Diabetes Mellitus, n (%) | 150 (21.6) |
| Dyspepsia, n (%) | 148 (21.3) |
| Hyperlipidemia, n (%) | 95 (13.6) |
| Varicose veins, n (%) | 88 (12.6) |
| Obesity, n (%) | 86 (12.4) |
| Cardiac disease, n (%) | 48 (6.9) |
| Tabaquism, n (%) | 38 (5.5) |
| Depression, n (%) | 34 (4.9) |
| Anxiety, n (%) | 24 (3.4) |
| Alcoholism, n (%) | 15 (2.2) |
| Number of comorbidities, n (%) | |
| * None | 215 (30.9) |
| * 1 | 160 (23) |
| * 2 | 139 (20) |
| * 3 | 96 (13.8) |
| * 4 | 45 (6.5) |
| * 5 or more | 41 (5.9) |
Six hundred thirty eight (91.7%) persons had a job at the moment of the interview. Housekeeping (33%), sales workers (19%) and craft workers (9.8%) were the most common occupations and only 1.6% of the patients were unemployed or retired.
Five hundred and two patients (85.1%) had pain in the last 7 days at the moment of the interview, with a mean VAS pain of 6 (IQR 3); 507 (72.8%) patients had a VAS pain ≥4. Hundred and four (14.9%) patients mentioned past pain, with a mean VAS of 6 (IQR 4.8); 79 (75%) persons had VAS pain ≥4.
One hundred and thirty-three (19.1%) persons reported functional disability and a mean HAQ of 0.375 (IQR 0.7) was found. Of the 696 patients, 207 (29.7%) informed not adapting to their symptoms.
The most common places of pain were: hand in 181 (26%) patients, knee in 179 (25.8%), shoulder in 86 (12.4%) and elbow in 36 (5.2%) persons; the least frequent were spine, hips, knee and ankle, accounting for ≤2% of the total population.
By the time of the interview, 259 (37%) patients already knew their diagnosis. During the medical examination, the most common places of OA were knee in 356 (51.5%) patients, followed by hand in 224 (37%) persons; 93 (13%) had generalized OA. The least common sites of OA were spine, shoulder, hips and ankles.
Four hundred and ninety four patients (71%) reported having treatment for OA, of whom 412 (83.4%) were employing only one type of treatment, 56 (11.3%) two and 26 (5.3%) persons were using ≥3 types. In 77% of the population the main prescriber was a physician, and in up to 65.3% the main provider was the National Institute of Social Service (Instituto Mexicano del Seguro Social, IMSS). Hundred and thirteen (22.5%) patients used self-prescribed treatment.
NSAIDS were the most commonly used pharmacologic treatment, reported by 289 (58.5%) persons; diclofenac being the most frequent and used by 198 (68.5%) patients. Analgesics were utilized by 100 (20.2%) patients, being acetaminophen the most commonly employed in 73 (77%) individuals. With treatment, 434 (87.9%) patients reported benefit. Physical therapy, surgery and alternative medicine were reported by 37 (7.5%), 25 (5.1%) and 17 (3.4%) persons, respectively. Conversely, when self-prescribed treatment was compared to treatment given by a physician, we observed more utilization of NSAIDS by physicians (231/289, 79.9%) and of analgesics by self-prescribers (35/100, 35%).
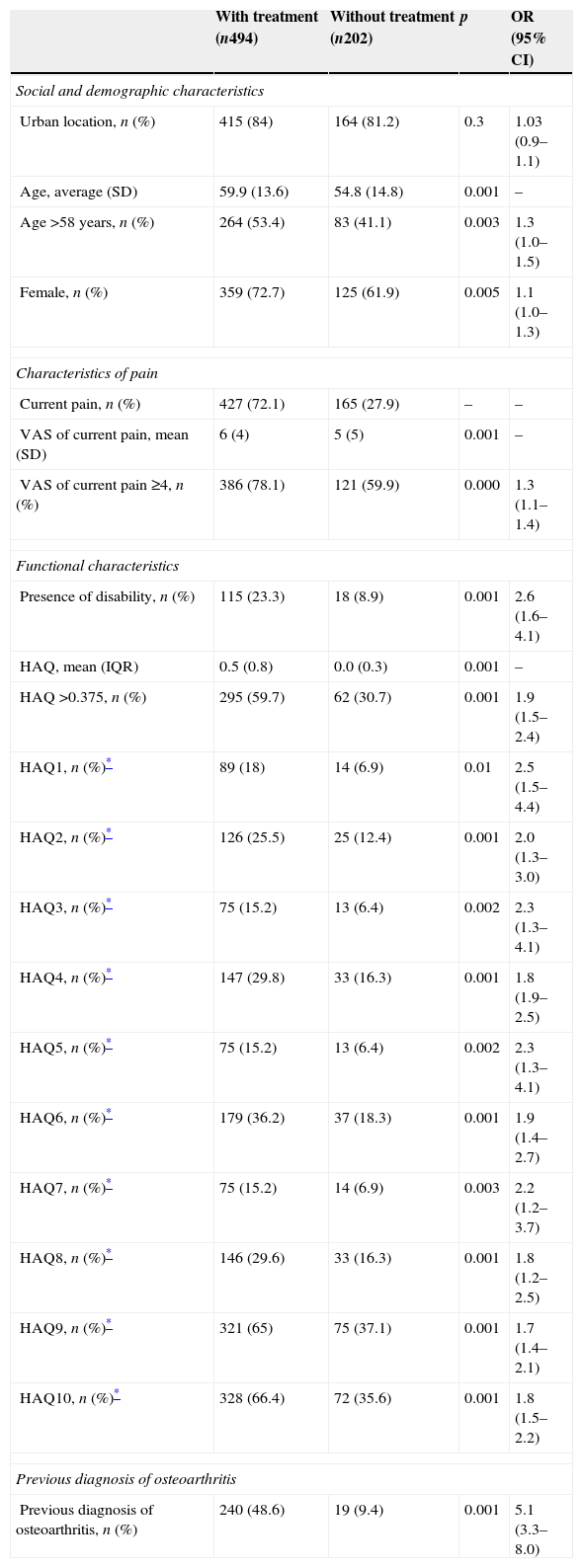
On the univariate analysis between those who received and those who did not receive treatment, age >58 years, female gender, VAS pain ≥4, functional disability, mean HAQ score and previous knowledge of OA diagnosis were statistically significant (Table 2). Of the comorbidities, varicose veins (OR 1.7, 95% CI 95 1.0–2.8) and hyperlipidemia (OR 1.6, 95% CI 95 1.0–2.6) were the only two related to the use of treatment, while marital status, occupation, past pain and symptom adaptation did not reach statistical significance (data not shown).
Univariate analysis between the groups who did/did not received treatment.
| With treatment (n494) | Without treatment (n202) | p | OR (95% CI) | |
|---|---|---|---|---|
| Social and demographic characteristics | ||||
| Urban location, n (%) | 415 (84) | 164 (81.2) | 0.3 | 1.03 (0.9–1.1) |
| Age, average (SD) | 59.9 (13.6) | 54.8 (14.8) | 0.001 | – |
| Age >58 years, n (%) | 264 (53.4) | 83 (41.1) | 0.003 | 1.3 (1.0–1.5) |
| Female, n (%) | 359 (72.7) | 125 (61.9) | 0.005 | 1.1 (1.0–1.3) |
| Characteristics of pain | ||||
| Current pain, n (%) | 427 (72.1) | 165 (27.9) | – | – |
| VAS of current pain, mean (SD) | 6 (4) | 5 (5) | 0.001 | – |
| VAS of current pain ≥4, n (%) | 386 (78.1) | 121 (59.9) | 0.000 | 1.3 (1.1–1.4) |
| Functional characteristics | ||||
| Presence of disability, n (%) | 115 (23.3) | 18 (8.9) | 0.001 | 2.6 (1.6–4.1) |
| HAQ, mean (IQR) | 0.5 (0.8) | 0.0 (0.3) | 0.001 | – |
| HAQ >0.375, n (%) | 295 (59.7) | 62 (30.7) | 0.001 | 1.9 (1.5–2.4) |
| HAQ1, n (%)* | 89 (18) | 14 (6.9) | 0.01 | 2.5 (1.5–4.4) |
| HAQ2, n (%)* | 126 (25.5) | 25 (12.4) | 0.001 | 2.0 (1.3–3.0) |
| HAQ3, n (%)* | 75 (15.2) | 13 (6.4) | 0.002 | 2.3 (1.3–4.1) |
| HAQ4, n (%)* | 147 (29.8) | 33 (16.3) | 0.001 | 1.8 (1.9–2.5) |
| HAQ5, n (%)* | 75 (15.2) | 13 (6.4) | 0.002 | 2.3 (1.3–4.1) |
| HAQ6, n (%)* | 179 (36.2) | 37 (18.3) | 0.001 | 1.9 (1.4–2.7) |
| HAQ7, n (%)* | 75 (15.2) | 14 (6.9) | 0.003 | 2.2 (1.2–3.7) |
| HAQ8, n (%)* | 146 (29.6) | 33 (16.3) | 0.001 | 1.8 (1.2–2.5) |
| HAQ9, n (%)* | 321 (65) | 75 (37.1) | 0.001 | 1.7 (1.4–2.1) |
| HAQ10, n (%)* | 328 (66.4) | 72 (35.6) | 0.001 | 1.8 (1.5–2.2) |
| Previous diagnosis of osteoarthritis | ||||
| Previous diagnosis of osteoarthritis, n (%) | 240 (48.6) | 19 (9.4) | 0.001 | 5.1 (3.3–8.0) |
Health Assessment Questionnaire (HAQ), Interquartile range (IQR), Visual analog scale (VAS), Osteoarthritis (OA).
Ungrouped HAQ: HAQ1 Dress. HAQ2 Get in and out of bed. HAQ3 Lift a glass to your mouth. HAQ4 Walk outdoors on flat ground. HAQ5 Wash and dry your entire body. HAQ6 Bend down to pick up clothing from the floor. HAQ7 Turn regular faucets on and off. HAQ8 Get in and out of a car. HAQ9 Squatting. HAQ10 Kneeling.
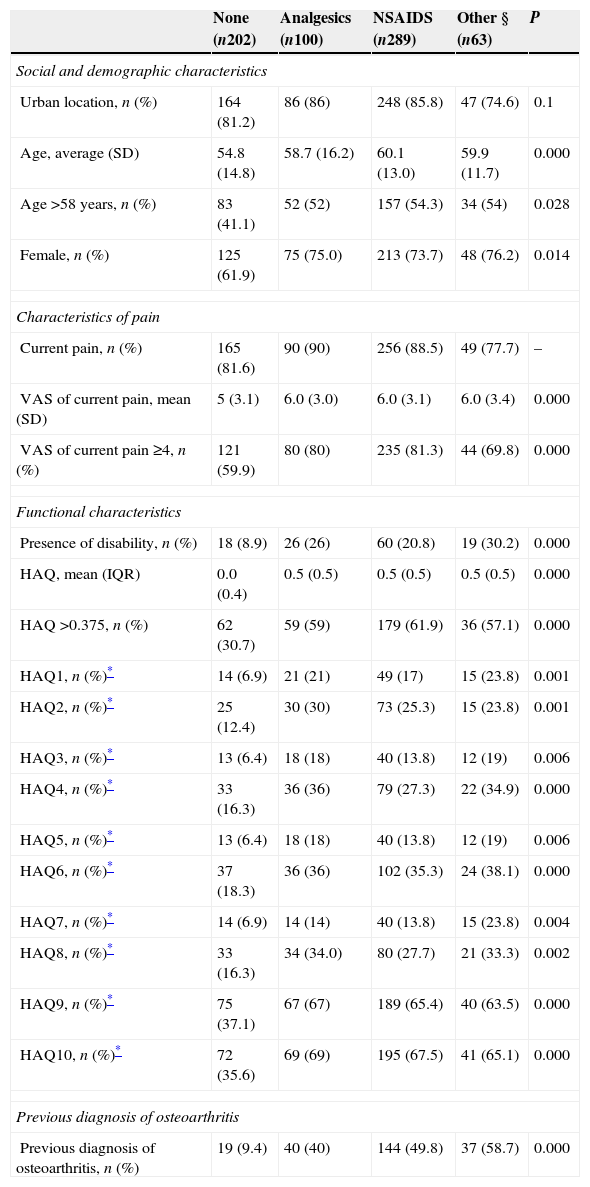
On the univariate analysis of the different treatments, NSAIDS were the most commonly used type, being statistical significant in age >58 years, female gender, VAS pain ≥4 (current or past), functional disability, HAQ >0.375 and previous knowledge of OA (Table 3). Of the comorbidities, the presence of diabetes mellitus and hyperlipidemia were also associated with the type of used treatment (p=0.007 and p=0.008, respectively).
Univariate analysis of the employed treatment.
| None (n202) | Analgesics (n100) | NSAIDS (n289) | Other § (n63) | P | |
|---|---|---|---|---|---|
| Social and demographic characteristics | |||||
| Urban location, n (%) | 164 (81.2) | 86 (86) | 248 (85.8) | 47 (74.6) | 0.1 |
| Age, average (SD) | 54.8 (14.8) | 58.7 (16.2) | 60.1 (13.0) | 59.9 (11.7) | 0.000 |
| Age >58 years, n (%) | 83 (41.1) | 52 (52) | 157 (54.3) | 34 (54) | 0.028 |
| Female, n (%) | 125 (61.9) | 75 (75.0) | 213 (73.7) | 48 (76.2) | 0.014 |
| Characteristics of pain | |||||
| Current pain, n (%) | 165 (81.6) | 90 (90) | 256 (88.5) | 49 (77.7) | – |
| VAS of current pain, mean (SD) | 5 (3.1) | 6.0 (3.0) | 6.0 (3.1) | 6.0 (3.4) | 0.000 |
| VAS of current pain ≥4, n (%) | 121 (59.9) | 80 (80) | 235 (81.3) | 44 (69.8) | 0.000 |
| Functional characteristics | |||||
| Presence of disability, n (%) | 18 (8.9) | 26 (26) | 60 (20.8) | 19 (30.2) | 0.000 |
| HAQ, mean (IQR) | 0.0 (0.4) | 0.5 (0.5) | 0.5 (0.5) | 0.5 (0.5) | 0.000 |
| HAQ >0.375, n (%) | 62 (30.7) | 59 (59) | 179 (61.9) | 36 (57.1) | 0.000 |
| HAQ1, n (%)* | 14 (6.9) | 21 (21) | 49 (17) | 15 (23.8) | 0.001 |
| HAQ2, n (%)* | 25 (12.4) | 30 (30) | 73 (25.3) | 15 (23.8) | 0.001 |
| HAQ3, n (%)* | 13 (6.4) | 18 (18) | 40 (13.8) | 12 (19) | 0.006 |
| HAQ4, n (%)* | 33 (16.3) | 36 (36) | 79 (27.3) | 22 (34.9) | 0.000 |
| HAQ5, n (%)* | 13 (6.4) | 18 (18) | 40 (13.8) | 12 (19) | 0.006 |
| HAQ6, n (%)* | 37 (18.3) | 36 (36) | 102 (35.3) | 24 (38.1) | 0.000 |
| HAQ7, n (%)* | 14 (6.9) | 14 (14) | 40 (13.8) | 15 (23.8) | 0.004 |
| HAQ8, n (%)* | 33 (16.3) | 34 (34.0) | 80 (27.7) | 21 (33.3) | 0.002 |
| HAQ9, n (%)* | 75 (37.1) | 67 (67) | 189 (65.4) | 40 (63.5) | 0.000 |
| HAQ10, n (%)* | 72 (35.6) | 69 (69) | 195 (67.5) | 41 (65.1) | 0.000 |
| Previous diagnosis of osteoarthritis | |||||
| Previous diagnosis of osteoarthritis, n (%) | 19 (9.4) | 40 (40) | 144 (49.8) | 37 (58.7) | 0.000 |
Non-steroidal anti-inflammatory drugs (NSAIDS), Health Assessment Questionnaire (HAQ), Interquartile range (IQR), Visual analog scale (VAS), Osteoarthritis (OA).
Ungrouped HAQ: HAQ1 Dress. HAQ2 Get in and out of bed. HAQ3 Lift a glass to your mouth. HAQ4 Walk outdoors on flat ground. HAQ5 Wash and dry your entire body. HAQ6 Bend down to pick up clothing from the floor. HAQ7 Turn regular faucets on and off. HAQ8 Get in and out of a car. HAQ9 Squatting. HAQ10 Kneeling.
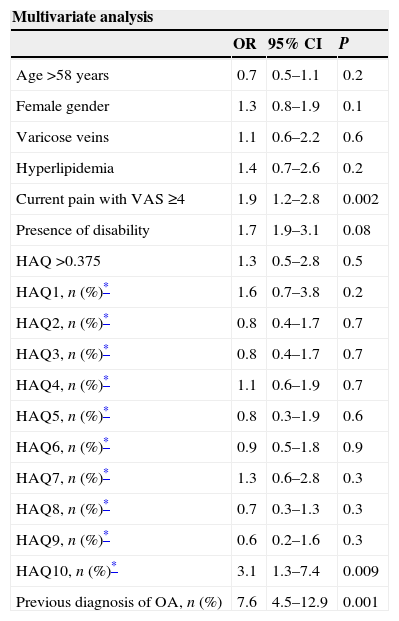
On the multivariate logistic regression analysis, VAS pain ≥4, kneeling disability (HAQ) and previous knowledge of OA diagnosis were the factors associated with treatment of OA (Table 4).
Multivariate analysis of the variables associated with treatment.
| Multivariate analysis | |||
|---|---|---|---|
| OR | 95% CI | P | |
| Age >58 years | 0.7 | 0.5–1.1 | 0.2 |
| Female gender | 1.3 | 0.8–1.9 | 0.1 |
| Varicose veins | 1.1 | 0.6–2.2 | 0.6 |
| Hyperlipidemia | 1.4 | 0.7–2.6 | 0.2 |
| Current pain with VAS ≥4 | 1.9 | 1.2–2.8 | 0.002 |
| Presence of disability | 1.7 | 1.9–3.1 | 0.08 |
| HAQ >0.375 | 1.3 | 0.5–2.8 | 0.5 |
| HAQ1, n (%)* | 1.6 | 0.7–3.8 | 0.2 |
| HAQ2, n (%)* | 0.8 | 0.4–1.7 | 0.7 |
| HAQ3, n (%)* | 0.8 | 0.4–1.7 | 0.7 |
| HAQ4, n (%)* | 1.1 | 0.6–1.9 | 0.7 |
| HAQ5, n (%)* | 0.8 | 0.3–1.9 | 0.6 |
| HAQ6, n (%)* | 0.9 | 0.5–1.8 | 0.9 |
| HAQ7, n (%)* | 1.3 | 0.6–2.8 | 0.3 |
| HAQ8, n (%)* | 0.7 | 0.3–1.3 | 0.3 |
| HAQ9, n (%)* | 0.6 | 0.2–1.6 | 0.3 |
| HAQ10, n (%)* | 3.1 | 1.3–7.4 | 0.009 |
| Previous diagnosis of OA, n (%) | 7.6 | 4.5–12.9 | 0.001 |
Health Assessment Questionnaire (HAQ), Visual analog scale (VAS), Osteoarthritis (OA).
Ungrouped HAQ: HAQ1 Dress. HAQ2 Get in and out of bed. HAQ3 Lift a glass to your mouth. HAQ4 Walk outdoors on flat ground. HAQ5 Wash and dry your entire body. HAQ6 Bend down to pick up clothing from the floor. HAQ7 Turn regular faucets on and off. HAQ8 Get in and out of a car. HAQ9 Squatting. HAQ10 Kneeling.
COPCORD was designed as a lowcost low-infrastructure model and was to be carried out in three successive stages: collect population data in a house-to-house survey to gather epidemiological data about rheumatic diseases (stage 1), educate community and identify risk factors (stage 2), and implement control and preventive strategies (stage 3). Darmawan previously reported that, according to their epidemiological data, it was apparent that primary health care of patients with rheumatic disease was nonexistent or inadequate, and this was complicated by self-medication in developing countries.12 Plenty of treatment resources and methods, including ethnic and local indigenous therapies, have been reported by COPCORD surveys. To our knowledge there are no studies that, using the COPCORD protocol, describe from the patients’ perspective the factors associated with the use of treatment in OA.
This study was performed on a representative sample of the State of Nuevo León, Mexico. Information was obtained by the application of the COPCORD questionnaire to identify all persons with musculoskeletal pain, either past or current, of which, a subgroup of patients with clinical diagnosis of OA was analyzed to find the factors associated with treatment. We found that the factors associated with treatment of OA were VAS pain ≥4, kneeling disability (HAQ) and previous knowledge of OA diagnosis.
Pain is the main symptom of osteoarthritis; however, it is subjective and hard to measure. The visual analog scale is a useful tool and it is very effective to measure the intensity of osteoarthritis pain.13,14 VAS pain with an intensity ≥4 has been associated to the need for medical attention in patients with musculoskeletal disease, and the perception of the patient with respect to pain is an important predictor for seeking medical attention.15,16 Furthermore, compared to those who do not seek medical attention, those who do have a more severe disease and higher disability.17 Likewise, in our study, VAS pain ≥4 was a variable associated with treatment. Even if it can be anticipated that the higher the pain the higher the likelihood of using treatment, it is more the compilation of physical, social and psychological aspects the ones related to the need for treatment, either prescribed by a physician or self-prescribed.17 Moreover, the knees and the hands were the most common sites of pain, which is similar to a previous study, and these are the most used joints and the anatomic regions with more prevalence of OA.18
In our population, only 19.1% had functional disability, which could have also been an explanation for not seeking medical attention. Besides, most patients reported being well adapted to their symptoms since only 29.7% stated otherwise, this being another important factor related to treatment, although this was not statistical significant. In a recent study performed by Burgos-Vargas et al. in patients with knee OA, only a small proportion of the patients lost their jobs because of the disease, and only 4% were unable to do any physical activity.19
On the other hand, activities that require kneeling for prolonged time are associated risk factors for the development of OA and are also related with higher joint cartilage damage.20,21 Accordingly, there is an association among these activities and the presence of symptomatic OA.22 Nevertheless, the features and location of knee pain are different between patients, reinforcing the diversity of the disease. Functional disability is higher in those patients with generalized knee pain, mainly in activities that require kneeling.23 By such reason, the kneeling disability found in these study could explain the relationship of these variable with the use of treatment.
Age and gender are among the risk factors for the development of OA. In our study, the mean age was >50 years and was more common in women, similar to the prevalence reported worldwide.24,25 Interestingly, living in an urban or a rural area was not associated with treatment. Marital status and occupation were not associated with treatment of OA either.15
The relationship between comorbidities and OA has been widely described. It has been reported that up to 53% of patients have arterial hypertension and OA.26 In Mexico, in a study at a hospital setting, the prevalence of arterial hypertension and diabetes mellitus in OA patients was 35% and 15%, respectively.27 In our study, even though some comorbidities were associated with treatment in the univariate analysis, in the multivariate logistic regression analysis no comorbidity reached statistical significance. It is worth mentioning that the prevalence of arterial hypertension and diabetes mellitus in this study was 31% (n216) and 21.6% (n150), respectively, and these were also the most common comorbidities. Indeed, the influence of comorbidities in the elderly population has been described, were the more the comorbidities the higher the probability of not having social activities, which may impact the search for medical attention or treatment.28
In this analysis, the two most frequent locations of OA were the knee (51.1%) and the hand (32.2%), according to the clinical definition and without the use of imaging, which could have underestimated the final prevalence. However, being OA of the hand and the knee the ones causing most of the disability in the population, the identification of modifiable risk factors is necessary for the development of strategies to reduce the burden of the disease.
When it comes to the selection of treatment, guidelines recommend acetaminophen as first line option for low to moderate OA, since it has very few side effects, drug interactions or contraindications and it is considered “safe” and “cheap” by patients and physicians.29 NSAIDS are regarded as second line treatment when pain relief is not achieved with acetaminophen; however, they are associated with side effects such as dyspepsia and renal toxicity.6 The use of certain drugs (i.e. Angiotensin-converting enzyme inhibitors for arterial hypertension) increases the risk of severe side effects.30,31 In spite of these considerations, the most employed treatment in our population, as reported by participants, were NSAIDS, being diclofenac the most frequently prescribed. Moreover, there was a higher trend for the use of NSAIDS compared to analgesics or other treatment options regardless of comorbidities, including diabetes mellitus and hypertension. We acknowledge that the proposed guidelines are established to aim therapeutic decisions for physicians and health care providers, nonetheless, with the use of strategies such as the COPCORD questionnaire a real-life approach to the patients’ point of view and inclination towards prescribed drugs can be attained. As such, NSAIDS were prescribed by physicians, which might reinforce the need to offer training modules to update the medical community of the first level of attention and prevent possible complications related to treatment, along with reducing the economic burden of the treatment of such chronic diseases, as well as improve the communication towards the patient.
Another important consideration is the low number of patients receiving physical therapy, a well-known standard of treatment for OA,32 which could be related to the lack of facilities and qualified personnel in the community. On the other hand, since pain and joint stiffness can hinder a person's daily life activity, it is important to consider that the majority of patients described feeling better with the employed treatment (87.9%).
As previously mentioned, the information was gotten by means of the COPCORD questionnaire and as such, the information comes directly from the patient. Because of the design of the COPCORD strategy, it is practically impossible, when it comes to treatment, to verify the information given by the patient with every physician prescription. Also, when it comes to occupation, the burden and activities of the job realized by every person included in the study were not established. Moreover, there are other important factors related to OA like body mass index, menopause, occupation, daily life and leisure activities, family history, joint alignment, among others that could not be obtained because they were not included in the questionnaire, which are weaknesses of the study.22,33 Nevertheless, it is important to emphasize that the COPCORD study was done in a stratified (by region), balanced, and random sample of subjects representative of Nuevo León, a state with a population of 4653 millions as of 2010, and patients were evaluated at their homes by certified rheumatologists. Population samples using the COPCORD protocol include a higher proportion of patients with minor changes, which would be less likely to produce symptoms. Moreover, the COPCORD questionnaire provides information of the therapeutic conduct from the patients’ perspective and in real life.
In conclusion, the factors associated with treatment of Osteoarthritis in the urban and rural communities of Nuevo León are VAS pain ≥4, kneeling disability (HAQ) and previous knowledge of OA diagnosis. Finally, it is necessary to perform an investigation that allows us to know how to detect and improve the treatment of patients in a timelier manner and at an earlier OA stage. Besides, the knowledge of this type of patterns may improve the delivery of medical attention to such prevalent diseases like OA.
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Source of financingCONACYT-Salud 2007-C01 69765.
Conflict of interestNone.
The authors would like to thank the National Council of Science and Technology (CONACYT) who provided the economical support for the study. CONACYT-Salud 2007-C01 69765.
Special thanks to the Group of Epidemiological Study of Muscle-skeletal Joint Diseases (GEEMA, spanish abbreviation): Peláez-Ballestas I, Sanin LH, Moreno-Montoya J, Alvarez-Nemegyei J, Burgos-Vargas R, Garza-Elizondo M, Rodríguez-Amado J, Goycochea-Robles MV, Madariaga M, Zamudio J, Santana N, Cardiel-Ríos MH, Cuervo GE.


