

We report a case of gonococcal arthritis in a patient with human immunodeficiency virus (HIV) infection and review 17 previously published cases; only one patient presented urethritis, and blood cultures were positive in one case. Gonococcal arthritis is rare in HIV-infected patients and is not usually associated with other symptoms. It should be considered in the differential diagnosis of acute arthritis in patients with HIV infection.
Presentamos un caso de artritis gonocócica en un paciente con infección por el virus de inmunodeficiencia humana (VIH) y revisamos los 17 casos previamente publicados en sujetos con infección por este virus; solo un paciente presentó uretritis y los hemocultivos fueron positivos en un caso. La artritis gonocócica es infrecuente en pacientes con infección por el VIH y suele presentarse de forma aislada. Debe incluirse en el diagnóstico diferencial de las artritis agudas en pacientes con infección por el VIH.
The prevalence of gonococcal urethritis in homosexuals with human immunodeficiency virus (HIV) infection ranges between 1.7% and 19%1 and the prevalence of asymptomatic gonococcal infection in this population is around 10%.2 Despite this high prevalence of gonococcal infection in homosexuals with HIV infection, there have been few reports of gonococcal urethritis. We present a new case and review those published until now.
Case ReportThe patient was a 65-year-old homosexual man with a 16-year history of HIV infection. He was undergoing regular follow-up and was receiving retroviral therapy with tenofovir, emtricitabine and neviirapine. He had a good adherence and tolerance and good immunovirological control (HIV viral load <20copies/mL and CD4+ lymphocytes at 870cells/μL). He presented with pain and inflammation of the left knee, which exhibited functional weakness, with no fever or other symptoms. On the physical examination, he reported pain on the mobilization of the knee, where there was a discreet effusion. The laboratory tests showed leukocytosis with 14,200cells/mL, 77% neutrophils, and C-reactive protein was 279mg/L. Magnetic resonance imaging showed joint effusion and synovitis with synovial thickening, especially in the suprapatellar synovial bursa. Arthrocentesis yielded a cloudy fluid with 24,000leukocytes/mL, predominantly polymorphonuclear, glucose level of 2mg/dL and proteins, 5.7g/dL. The culture produced Neisseria gonorrhoeae, which is sensitive to 3rd-generation cephalosporins and resistant to ciprofloxacin. The patient was treated with intramuscular ceftriaxone at 1g daily for 1 week, and his symptoms slowly resolved. The blood culture performed prior to the antibiotic therapy was negative. Three months before, he had been diagnosed as having early latent syphilis, which was treated with a dose of benzathine penicillin.
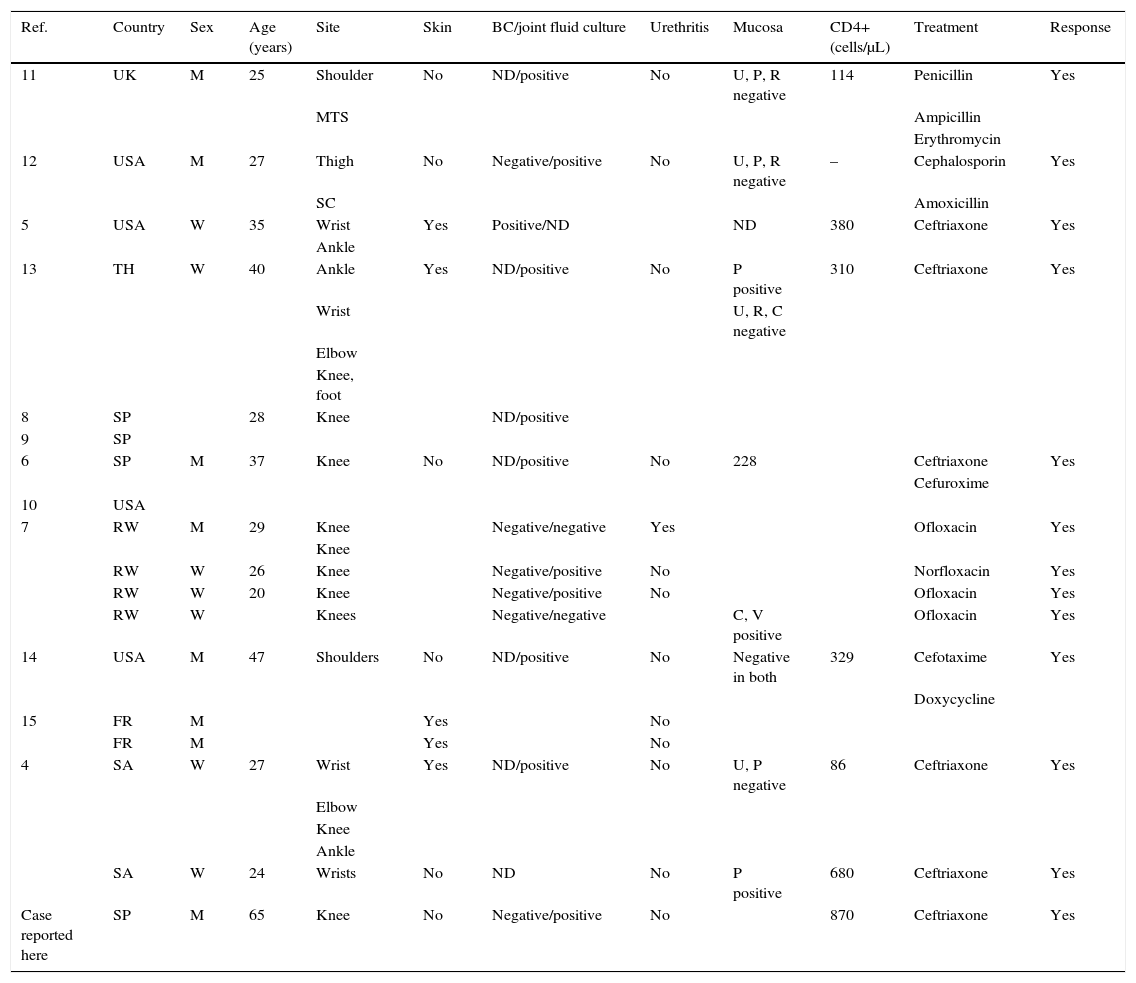
DiscussionGonococcal arthritis is generally produced by hematogenous dissemination of N. gonorrhoeae, although this bacterium is uncommon in patients with urethritis.3 The prevalence is estimated to be 0.5%–3%.3 In the general population, the disseminated infection predominates in women and both men and women very often have an asymptomatic infection of the mucosa.3 In the series of cases of gonococcal arthritis and HIV infection published to date4–15 (Table 1), blood cultures were positive in only 1 of the 7 cases in which they were performed and only 1 patient had urethritis. It is striking that the 65-year-old patient who we present here was the oldest of those reported. There is male predominance because HIV infection, except in Africa, mostly affects men. Four individuals had skin involvement, and asymptomatic mucosal infection was detected in 3 of the 7 patients in whom urethral, pharyngeal, rectal or cervicovaginal specimens were taken. Although the immunosuppression associated with HIV has been proposed to favor the development of disseminated gonococcal infection,7,8 most of the patients with HIV infection and gonococcal arthritis had a good immunological status.
Published Cases of Gonococcal Arthritis in Patients With Human Immunodeficiency Virus.
| Ref. | Country | Sex | Age (years) | Site | Skin | BC/joint fluid culture | Urethritis | Mucosa | CD4+ (cells/μL) | Treatment | Response |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 11 | UK | M | 25 | Shoulder | No | ND/positive | No | U, P, R negative | 114 | Penicillin | Yes |
| MTS | Ampicillin | ||||||||||
| Erythromycin | |||||||||||
| 12 | USA | M | 27 | Thigh | No | Negative/positive | No | U, P, R negative | – | Cephalosporin | Yes |
| SC | Amoxicillin | ||||||||||
| 5 | USA | W | 35 | Wrist | Yes | Positive/ND | ND | 380 | Ceftriaxone | Yes | |
| Ankle | |||||||||||
| 13 | TH | W | 40 | Ankle | Yes | ND/positive | No | P positive | 310 | Ceftriaxone | Yes |
| Wrist | U, R, C negative | ||||||||||
| Elbow | |||||||||||
| Knee, foot | |||||||||||
| 8 | SP | 28 | Knee | ND/positive | |||||||
| 9 | SP | ||||||||||
| 6 | SP | M | 37 | Knee | No | ND/positive | No | 228 | Ceftriaxone | Yes | |
| Cefuroxime | |||||||||||
| 10 | USA | ||||||||||
| 7 | RW | M | 29 | Knee | Negative/negative | Yes | Ofloxacin | Yes | |||
| Knee | |||||||||||
| RW | W | 26 | Knee | Negative/positive | No | Norfloxacin | Yes | ||||
| RW | W | 20 | Knee | Negative/positive | No | Ofloxacin | Yes | ||||
| RW | W | Knees | Negative/negative | C, V positive | Ofloxacin | Yes | |||||
| 14 | USA | M | 47 | Shoulders | No | ND/positive | No | Negative in both | 329 | Cefotaxime | Yes |
| Doxycycline | |||||||||||
| 15 | FR | M | Yes | No | |||||||
| FR | M | Yes | No | ||||||||
| 4 | SA | W | 27 | Wrist | Yes | ND/positive | No | U, P negative | 86 | Ceftriaxone | Yes |
| Elbow | |||||||||||
| Knee | |||||||||||
| Ankle | |||||||||||
| SA | W | 24 | Wrists | No | ND | No | P positive | 680 | Ceftriaxone | Yes | |
| Case reported here | SP | M | 65 | Knee | No | Negative/positive | No | 870 | Ceftriaxone | Yes |
BC, blood culture; C, cervix; FR, France; M, man; MTS, metatarsus; ND, not done; P, pharynx; R, rectum; RW, Rwanda; SA, South Africa; SC, sternoclavicular; SP, Spain; TH, Thai; U, urethra; UK, United Kingdom; USA, United States; V, vagina; W, woman.
The diagnosis of gonococcal arthritis requires a high index of suspicion and, aside from blood culture and joint fluid culture, it is necessary to take urethral, pharyngeal, rectal and cervical specimens, as well as from possible skin lesions; the treatment of choice is based on 3rd-generation cephalosporins. An emerging problem is an increase in the decline in susceptibility and resistance to ceftriaxone.3
ConclusionsDespite the high prevalence of gonococcal infection among homosexuals with HIV infection, gonococcal arthritis is uncommon. There must be a high index of suspicion and include it in the differential diagnosis of acute arthritis in patients with HIV infection, especially in those at risk for sexually transmitted infections.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of InterestThe authors declare they have no conflicts of interest.
Please cite this article as: Sena Corrales G, Mora Navas L, Palacios Muñoz R, García López V, Márquez Solero M, Santos González J. Artritis gonocócica en pacientes con infección por el virus de la inmunodeficiencia humana. Revisión de la literatura. Reumatol Clín. 2017;13:39–41.


