
To describe the methodology, objectives, and initial data of the registry of young adult patients diagnosed with Juvenile Idiopathic Arthritis (JIA), JUVENSER. The main objective of the project is to know the sociodemographic and clinical characteristics, and disease activity of patients with JIA reaching the transition to adulthood.
Material and methodLongitudinal, prospective, multicentre study, including patients between 16 and 25 years old, with a diagnosis of JIA in any of its categories. The main objective is to determine the characteristics and activity of JIA in the young adult. It includes sociodemographic variables, clinical variables, disease activity and joint damage rates, data on the use of health resources, and treatments used. The total duration of the project will be 3 years. A cohort of 534 young adult patients was obtained.
ConclusionsThe JUVENSER registry will constitute a cohort of young adults with JIA, which will allow the evaluation of the clinical characteristics and response to treatment of patients with disease onset in childhood, moving to adult clinics.
Describir la metodología, los objetivos y exponer los datos iniciales del registro de pacientes adultos jóvenes con diagnóstico de Artritis Idiopática Juvenil (AIJ), registro JUVENSER, así como sus fortalezas y limitaciones. El objetivo principal del proyecto es conocer las características sociodemográficas, clínicas y la actividad de la enfermedad de pacientes con AIJ en el period de transición a la vida adulta.
Material y métodoEstudio longitudinal, prospectivo, multicéntrico que incluye pacientes adultos jóvenes, entre 16 y 25 años, con diagnóstico de AIJ en cualquiera de sus categorías, atendidos en consultas de reumatología de 16 centros hospitalarios españoles cuyo objetivo principal es determinar las características y la actividad de las AIJ en los primeros años de la vida adulta. Se diseñó un registro en el que se incluyeron variables sociodemográficas, variables clínicas, índices de actividad y daño articular, datos de la utilización de recursos sanitarios, y los fármacos y tratamientos utilizados. El periodo de reclutamiento fue de 27 meses y la duración total del proyecto serán 3 años. Se ha conseguido una cohorte de 534 pacientes adultos jóvenes.
ConclusionesEl registro JUVENSER constituirá una cohorte de pacientes adultos jóvenes con AIJ, que permitirá evaluar las características clínicas y respuesta a tratamiento de los pacientes con inicio de su enfermedad en edad pediátrica que llegan a las consultas de adultos. Se espera que la información recogida en las visitas suponga una amplia fuente de datos para futuros análisis.
Juvenile idiopathic arthritis (JIA) is the most common chronic rheumatic disease in paediatrics. The International League of Associations for Rheumatology (ILAR) established the standard diagnostic criteria for JIA,1–3 defining it as arthritis of unknown origin diagnosed in patients before the age of 16 and of at least six weeks’ duration. JIA is subdivided into 7 different subtypes: systemic, oligoarthritis (persistent or extended), polyarthritis (rheumatoid factor positive), polyarthritis (rheumatoid factor negative), psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis.
The Spanish National Health System (SNS) provides the framework guaranteeing health coverage for its citizens. Health management in its broadest concept, which includes planning, provision, and evaluation of services, is based on a decentralised model in the autonomous communities.
Transfer from paediatrics to primary care starts at15 years of age; however, patients with chronic diseases may continue in specialist paediatric care services, depending on the transition model implemented in these services. This transition model will be evaluated in this registry.
Management of JIA poses a challenge to health systems and requires coordinated work between the different professionals involved, who must also provide patients with the available information on their disease.4 The transition from adolescence to adulthood is a critical time.5–7 The transition of chronically ill patients from childhood to adolescence and adulthood has been the focus of the Child-Friendly Healthcare Initiative (CFHI), under the auspices of the Department of Child and Adolescent Health and Development of the World Health Organization (WHO), the Royal College of Nursing (UK), the Royal College of Paediatrics and Child Health (UK), and UNICEF. This initiative recognises the importance of health services that monitor these patients and the informative and preventive health role they should play.8
The management of young adult patients diagnosed with JIA is not yet well defined. The available evidence on the use of biologic treatments for these patients is limited, in terms of both safety and efficacy.9–14 In general terms, biologic drugs have shown no safety problems in adolescence different to those known for adults. However, in organisational terms, complications in care and resource use have been identified in this group of patients.15 The Spanish Society of Paediatric Rheumatology has drawn up a consensus on the management of biologic drug use in adolescents.16
The correct treatment and management of JIA patients in the age of transition may be crucial to improve their quality of life. These patients face difficulties in relation to their integration into education, employment, and other activities that are normal for any adolescent.17–20 The impact of this group of diseases persists over time and influences the patient's quality of life, activity, comorbidities, and chronic damage.21–26
The limited information available on these patients during this stage of life, in relation to disease activity and structural damage, may be of interest as a basis to explain the development of complications and other associated problems. Hence the launching of the JUVENSER project, a registry of young adult patients diagnosed with JIA, whose main objective is to describe the socio-demographic and clinical characteristics and disease activity of patients with JIA reaching the transition stage to adulthood, and the progression and therapeutic management of patients diagnosed with JIA in childhood in Spain. This paper describes the methodology, objectives, and initial data of the project, as well as its strengths and limitations.
MethodologyGeneral designA longitudinal, prospective, multicentre study including six-monthly follow-up visits for the duration of the study fieldwork. The minimum number of visits will be 3 for the last patient included in the study, including one baseline and two six-monthly follow-up visits. There will be a maximum of 5 visits: one baseline visit and 4 six-monthly follow-up visits.
Reference populationYoung adult patients between 16 and 25 years of age diagnosed with any category of JIA, seen in rheumatology consultations in Spanish hospitals participating in the study.
Inclusion and exclusion criteria- 1
Inclusion criteria:
- -
Patients aged between 16 and 25 years at the time of inclusion in the registry.
- -
Patients diagnosed with any form of JIA.
- -
Patients presenting for the first time or under follow-up in a transition or adult rheumatology consultation.
- -
Patients agreeing to participate in the registry by signing the informed consent form.
- -
- 2
Exclusion criteria:
- -
Patients who, in the opinion of the investigator, would have difficulties in attending the visits or completing the questionnaires on their own.
- -
Patients who have not signed the informed consent form.
- -
All rheumatology services of public hospitals of the Spanish National Health System that treat young adult patients diagnosed with JIA were invited to participate through the usual communication channels of the Spanish Society of Rheumatology (SER). The heads of rheumatology services, or of the services on which the rheumatology units concerned depend, were aware of and agreed to their centres participating in the study.
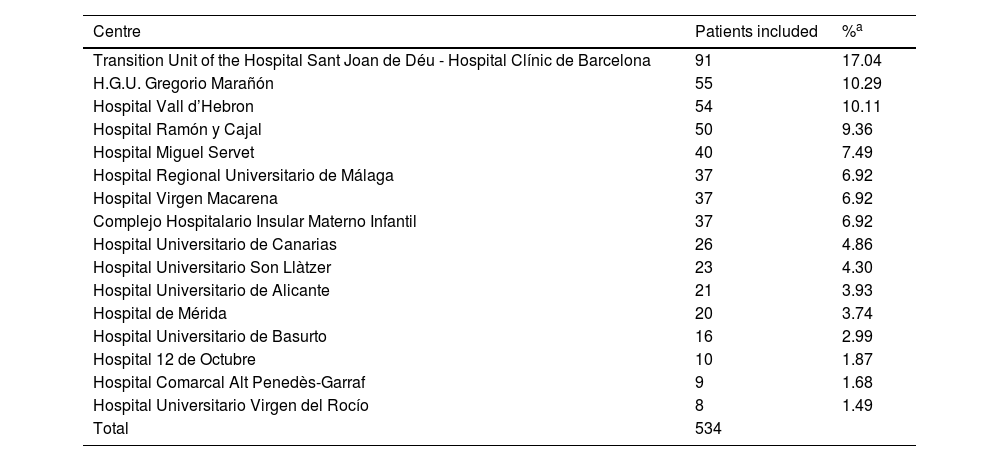
For the selection of participating centres, the head of the centre had to send the SER a formally signed document, commitment of the investigator, and complete a feasibility questionnaire reflecting the capacity to participate and recruit patients for the study, evaluated by the study's scientific committee (Table 1).
Participating centres and inclusion of patients in the JUVENSER registry.
| Centre | Patients included | %a |
|---|---|---|
| Transition Unit of the Hospital Sant Joan de Déu - Hospital Clínic de Barcelona | 91 | 17.04 |
| H.G.U. Gregorio Marañón | 55 | 10.29 |
| Hospital Vall d’Hebron | 54 | 10.11 |
| Hospital Ramón y Cajal | 50 | 9.36 |
| Hospital Miguel Servet | 40 | 7.49 |
| Hospital Regional Universitario de Málaga | 37 | 6.92 |
| Hospital Virgen Macarena | 37 | 6.92 |
| Complejo Hospitalario Insular Materno Infantil | 37 | 6.92 |
| Hospital Universitario de Canarias | 26 | 4.86 |
| Hospital Universitario Son Llàtzer | 23 | 4.30 |
| Hospital Universitario de Alicante | 21 | 3.93 |
| Hospital de Mérida | 20 | 3.74 |
| Hospital Universitario de Basurto | 16 | 2.99 |
| Hospital 12 de Octubre | 10 | 1.87 |
| Hospital Comarcal Alt Penedès-Garraf | 9 | 1.68 |
| Hospital Universitario Virgen del Rocío | 8 | 1.49 |
| Total | 534 |
The scientific committee of the project comprises the two principal investigators and 4 researchers who are members of the SER, experts in the field of paediatric rheumatology. The SER regulations for the selection of experts in strategic projects were followed to select the scientific committee.27
Contact with the investigators and signing of the investigator’s commitmentAll investigators collaborating in the study signed a commitment document outlining their roles and obligations.
Informed consentAn information document was drawn up to explain to the patient what the study consisted of and the terms of their collaboration. The informed consent document itself was also drawn up and signed by the patient.
Patients' informed consent is a prerequisite for their inclusion in the study.
Ethical aspectsThe study will be conducted in accordance with the principles of the latest version of the Declaration of Helsinki. Likewise, the international standards relating to the conduct of epidemiological studies, set out in the International Guidelines for Ethical Review of Epidemiological Studies (Council for the International Organizations of Medical Sciences-CIOMS-Geneva, 1991) and the recommendations of the Spanish Society of Epidemiology (SEE) on the review of the ethical aspects of epidemiological research, which state that this type of study must be submitted for review by an independent committee, will be followed.
The study was submitted for evaluation to the medical research ethics committees (CEim) of all the participating centres. The reference CEim was that of the principal investigator (PI).
Official approval was requested from the management to conduct the study in each hospital, as well as the signed commitment of the investigator responsible for data collection at the centre. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data shall be considered in the collection and handling of data.
Drafting of the investigator’s manualA manual was drawn up that describes all the fieldwork in detail, from how to recruit the sample, to how the tests included in each dimension should be conducted and how to complete the sections of the data collection booklet (DCB). The aim of this manual is to ensure homogeneous data collection.
Patient recruitment and data collectionCollection, database management, and quality controlOnce the patient has been selected, and they have signed their informed consent, the data are collected in an electronic format DCB through a single computer application for all participating centres. The SER research unit (UI-SER) will oversee the final analysis of the data.
Data collectionA person responsible for the registry has been appointed in each centre, who will also oversee collecting the patients' data and sign the aforementioned investigator's commitment.
Medical data will be obtained from the medical records, and directly by interviewing the patient during the consultation. Patients aged 16–25 years lost to follow-up, having been diagnosed with JIA in paediatric rheumatology units, will be contacted in writing and asked to participate in the registry, to collect their data retrospectively and to fill in a health questionnaire about their current clinical and functional status and other questions related to transition and follow-up in adult consultations.
An investigator’s manual was designed to facilitate data collection, as mentioned above, and a quick guide to the questions that will be asked to obtain the data on the day of consultation with the patient. Patients will be asked to complete the self-administered questionnaires included in the protocol.
A visit will be considered closed when all the data from the history at the visit, complementary tests, and self-administered questionnaires have been entered.
CodingEach centre will be automatically designated a code. In addition, each patient will have an assigned code, the consecutive number of patients included in each centre, which will be preceded by the centre’s code.
None of the project’s data tables, the table used for the analysis or for the annual reports, will contain patient identification data, just the assigned codes. Only the data managers will know to which patient each code corresponds, and only according to the terms specified in the confidentiality section.
The first patient was included on 18 September 2020 and recruitment is expected to be completed in January 2023, with an effective inclusion period of 27 months, with six-monthly follow-up visits for each patient.
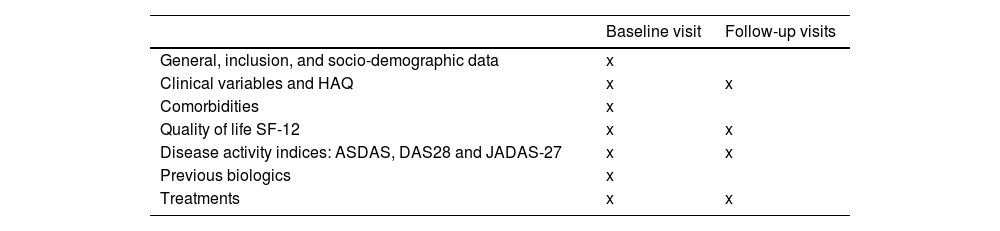
Variables and measurementsThe aim of the study is to determine the characteristics and activity of JIA in early adulthood using validated and widely used scales. Table 2 shows the measurements taken at each visit.
Summary of variables collected at each visit of the JUVENSER registry.
| Baseline visit | Follow-up visits | |
|---|---|---|
| General, inclusion, and socio-demographic data | x | |
| Clinical variables and HAQ | x | x |
| Comorbidities | x | |
| Quality of life SF-12 | x | x |
| Disease activity indices: ASDAS, DAS28 and JADAS-27 | x | x |
| Previous biologics | x | |
| Treatments | x | x |
ASDAS: Ankylosing Spondylitis Disease Activity Score; DAS28: Disease Activity Score; HAQ: Health Assessment Questionnaire; JADAS-27: Juvenile Arthritis Disease Activity Score; SF-12: Short Form 12 Health Survey.
Socio-demographic data such as current age, sex, race, patient origin, ILAR category at disease onset, age at diagnosis, years of disease course, presence of rheumatoid factor (RF), anti-citrullinated peptide antibodies (anti-CCP), antinuclear antibodies (ANA), and HLA-B27 are collected.
In addition, follow-up visits also record the patient's status in the study, whether the patient remains active or has dropped out of the registry, and the reason for dropping out.
Clinical variablesNumber of painful and swollen joints and entheses, patient/physician visual analogue scale (VAS) of disease activity (0–10), quality of life scale, SF-12, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), HAQ (Health Assessment Questionnaire), and recording of extra-articular manifestations (ocular, gastrointestinal, skin involvement). Recording of degree of disability, the patient's comorbidities using the Charlson index, and related diseases is also proposed.
Activity indices and joint damageThe activity indices used in adult patients are used to assess the activity, development, and progression of the disease. The JADAS (Juvenile Arthritis Activity Score) index has shown limitations for the assessment of adults with JIA,31 and therefore we opted to include the JADAS27 and attempt to assess its potential usefulness in the age range of the patients under study. We shall also use the activity scores used in adult patients: DAS28 for oligoarticular, polyarticular, and psoriatic arthritis JIA and ASDAS for the axial forms of psoriatic arthropathies and arthritis-enthesitis.
Use of resourcesOf interest will be variables related to resources that study participants may have used at the time of the visit: date of first visit to the adult rheumatology clinic, number of medical visits to the rheumatology service in the last year.
Drugs and treatments usedThis section includes the main pharmacological treatments: disease-modifying drugs (DMARDs) and/or biologics used since diagnosis with the start and end dates of each and the main pharmacological and non-pharmacological treatments being used at the time of inclusion in the registry. Information is collected on non-steroidal anti-inflammatory drugs (NSAIDs), corticoids, intra-articular and periarticular infiltrations, non-biological DMARDs, biological drugs, treatment, or prophylaxis of osteoporosis.
Statistical considerationsSample sizeGiven the wide variability of epidemiological information available on this patient group in Europe, the limited evidence available on the reference population, and the fact that the objectives of the study do not include a priori hypothesis testing, it is not considered necessary to establish a sample size. All patients meeting the inclusion criteria during the open recruitment period will be included.
The 2-year objective was to reach a sample of 450 patients in active follow-up, assuming a possible loss to follow-up of 10%.
Analysis planAt the end of each study year (from the second study year onwards) an annual report with the main findings will be produced. Descriptive analyses of socio-demographic variables, clinical variables, patient progression (disease activity indices), and use of treatments and resources available in the database will be prepared. Medians and interquartile ranges will be obtained for continuous quantitative variables, while qualitative variables will be described by frequencies (percentage).
Quality control of the databaseThere will be annual online monitoring. Every year, the consistency of all new data recorded in the data collection platform will be reviewed, with special attention to variables that collect information related to the objectives of the study.
Visit remindersPeriodic (every 3 months) reminder emails and on project status are sent to all participating schools over the inclusion period. In addition, a reminder e-mail is sent systematically from the electronic DCB to the investigators at each centre, notifying them on a date close to (in the month prior to the theoretical date) when the visits are scheduled, to ensure that the visits take place and patient information is collected.
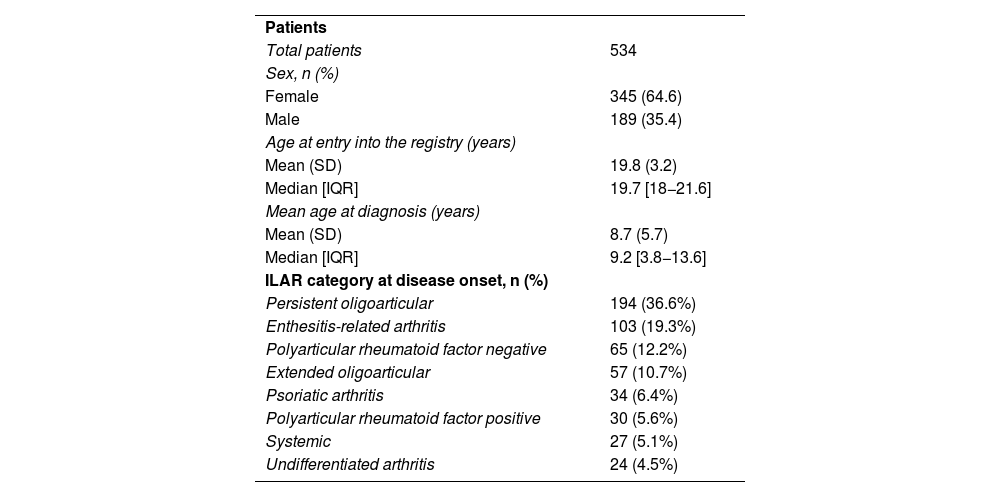
ResultsA total of 534 patients were recruited. Of these, 64.6% were women, with a mean age of 19.8±3.2 years. In terms of disease onset according to ILAR criteria, the most frequent categories are persistent oligoarticular form (36.3%) followed by enthesitis-related arthritis (19.3%) (Table 3).
Baseline characteristics of patients included in JUVENSER.
| Patients | |
| Total patients | 534 |
| Sex, n (%) | |
| Female | 345 (64.6) |
| Male | 189 (35.4) |
| Age at entry into the registry (years) | |
| Mean (SD) | 19.8 (3.2) |
| Median [IQR] | 19.7 [18−21.6] |
| Mean age at diagnosis (years) | |
| Mean (SD) | 8.7 (5.7) |
| Median [IQR] | 9.2 [3.8−13.6] |
| ILAR category at disease onset, n (%) | |
| Persistent oligoarticular | 194 (36.6%) |
| Enthesitis-related arthritis | 103 (19.3%) |
| Polyarticular rheumatoid factor negative | 65 (12.2%) |
| Extended oligoarticular | 57 (10.7%) |
| Psoriatic arthritis | 34 (6.4%) |
| Polyarticular rheumatoid factor positive | 30 (5.6%) |
| Systemic | 27 (5.1%) |
| Undifferentiated arthritis | 24 (4.5%) |
ILAR: International League of Associations for Rheumatology; IQR: Interquartile Range; SD: Standard Deviation.
This paper describes the objectives and methodology of the JUVENSER registry, and the general epidemiological data on recruitment. This registry involves the creation of a Spanish multicentre cohort of patients diagnosed with JIA in young adulthood, with a prospective 3-year follow-up.
Rheumatic disease in adolescence is the third most frequent reason for consultation in primary care at this age. One third of JIAs and 15%–20% of systemic lupus erythematosus begin in adolescence,21 and often continue into adulthood.
The transition to adulthood in JIA patients is of vital importance to maintain treatments in early adulthood. In a German cohort, only 41% of patients at the age of 20 years maintained the JIA diagnosis they had at the age of 16 years. The main reasons may be drug indications approved for use in adulthood, ease of coding in adult registries, or simply misclassification.22
The treatment of patients with paediatric rheumatic diseases has evolved in recent years, improving survival and quality of life. Nevertheless, 46% of 50 patients surveyed had poor adherence to treatment as measured by medication satisfaction questionnaires.28
Glerup et al.29 conducted an 18-year follow-up of 434 patients diagnosed with JIA in its different categories, with a mean age of 24±4.4 years, in the current biologic era. In this cohort, 46% of patients had ongoing disease activity as measured by JADAS71, 15% (66 patients) were on active treatment with synthetic DMARDs, and 19% (84 patients) were on biologics. Thirty-three percent of the cohort was in medication-free remission. In long-term follow-up studies prior to the introduction of biologic therapy as part of JIA treatment, Selvaag et al.30 found remission rates of 59% and fewer patients with active disease (33%), although these findings may be because clinical activity was not evaluated in half the patients, but assessed by self-administered clinical activity questionnaires.
A strength of this work is that the JUVENSER registry will prospectively follow young adults according to a research protocol. Follow-up visits are scheduled every six months for all patients, and the initial duration of the study is 3 years. The registry variables are standardised, and the data will be strictly monitored. We have sought to determine the degree of disease activity in the process of transition and transfer from paediatric to adult rheumatology consultations, and the extent of damage, drug use, comorbidities, disability, and quality of life using validated indices and questionnaires to assess disease status.
Our study also has a number of limitations. This cohort does not include patients from all autonomous communities. In terms of the design and objectives of the registry, the sample was not intended to be nationally representative. Another limitation could be selection bias, not including patients in clinical remission. For budgetary reasons, the initial design of this study includes only 3 years of follow-up, a short period to accurately analyse the evolution of functionality, sustainability of response to treatments, and some complications of the disease and its treatments.
ConclusionsThe JUVENSER registry is a cohort of young adults, diagnosed in paediatric age, recruited in Spanish rheumatology services. This project, promoted by the SER on paediatric-onset rheumatic diseases, will enable us to evaluate the clinical characteristics and treatments during the transfer from paediatric to adult rheumatology consultations. We hope that this will help us to understand and improve the care of active adult-onset JIA patients.
FundingJuvenser is funded by Sanofi Genzyme. Neither company participated in the study design, data collection or analysis, or the writing of this article.
Conflict of interestsThe authors have no conflict of interests to declare.
We would like to thank all the members of the UI-SER for their support and dedication to this project, particularly Federico Díaz-González, director of the UI-SER and Silvia Herrera, UI-SER financial manager, for their support in the search for funding for this project, Fernando Sánchez-Alonso, statistician of the UI-SER, and Susana Hernando, UI-SER Project administrative manager.


