




Koebner's isomorphic phenomenon consists of the reproduction of lesions typical of a dermatosis in areas that have suffered prior trauma, identical both clinically and histopathologically to the pre-existing dermatosis.1,2 Its pathogenesis remains little known, and is probably multifactorial, although it has been suggested that capillary changes take place in the dermis that precede all the morphological changes.3 Although it is well known in conditions such as psoriasis or vitiligo, Koebner's phenomenon has been described in many other dermatoses.1 Because there are so few cases published in the literature, vasculitis is included in the group of diseases that manifest this phenomenon less frequently.1,4 We present a case of idiopathic leukocytoclastic vasculitis with a striking Koebner's phenomenon in areas of scratching.
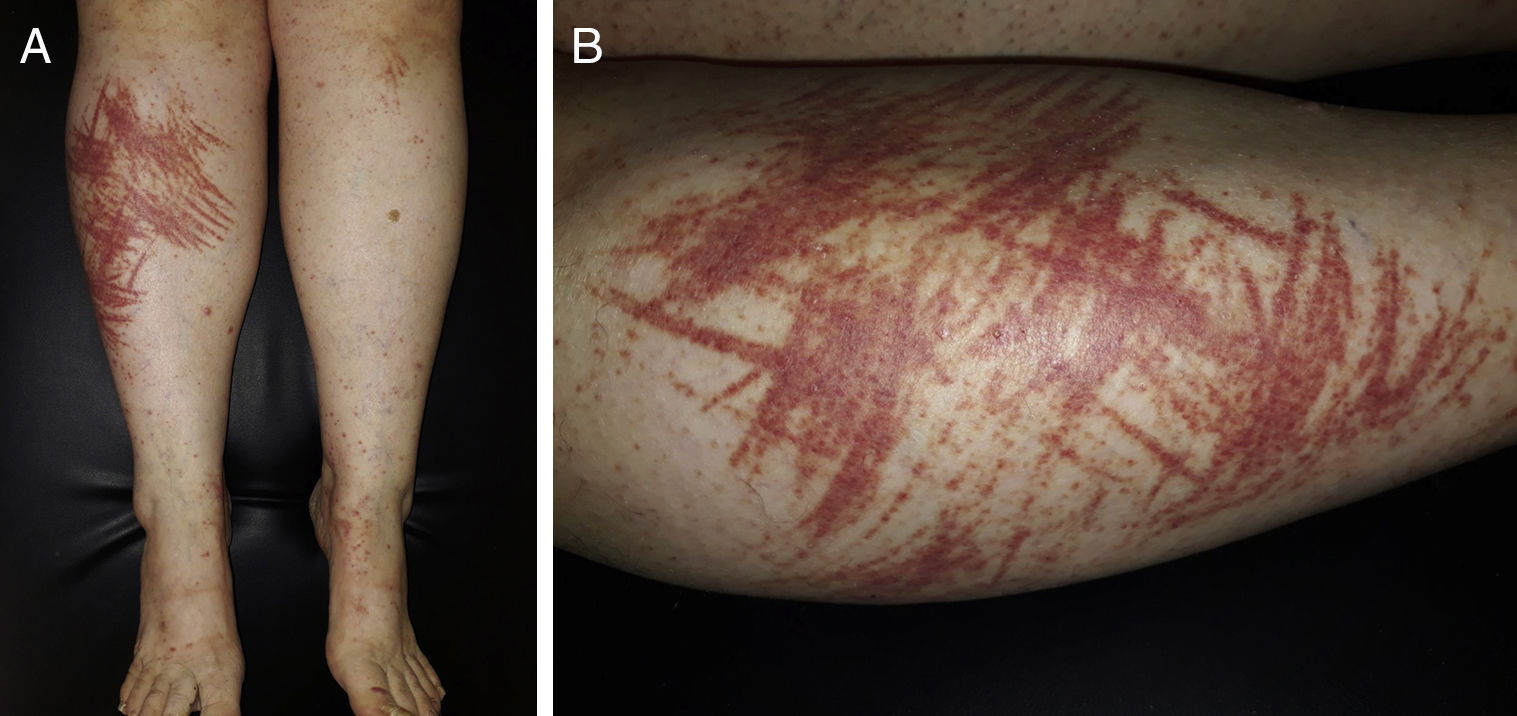
A 53-year-old woman, with no history of interest, consulted with a 3-day history of pruriginous erythematous-purpuric lesions on both lower limbs. The lesions were palpable, and did not disappear on diascopy. On both anterior pre-tibial surfaces they grouped and converged presenting a clear linear distribution, which was more intense on the right side (Fig. 1A and B). Although the patient admitted scratching due to her pruritis, there were no signs of abrasion. When her clinical history was taken she denied any intake of mushrooms or drugs. And she reported no gastrointestinal, respiratory tract, joint pain or other symptoms in previous days. A differential diagnosis was suggested between vasculitis or purpuric gloves and socks manifested as Koebner's phenomenon, and flagellate dermatitis. Peripheral blood, urine sediment analysis and chest x-ray showed no alterations, and autoimmune studies (ANA, ANCA, C3, C4 and CH50), and serologies (HBV, HCV and HIV) were negative. Skin biopsy reported leukocytoclastic vasculitis, and direct immunofluorescence study was negative.
Small-vessel leukocytoclastic vasculitis of the skin is mediated by a type III hypersensitivity reaction, and is due to the development of circulating immune complexes and their deposit in vessels of the superficial plexus, which causes inflammation and necrosis.5 There are many factors that can influence deposit of immune complexes in the vascular wall, such as the permeability of the vessels, the size and nature of the immune complex, hydrodynamic forces, etc.4,6 In the case of our patient, we believe that scratching was the trigger that activated deposit of immune complexes in the vessels of the superficial plexus of the damaged skin.
Despite the particular form of presentation of this case, with marked linear distribution of the lesions, leukocytoclastic vasculitis with Koebner's phenomenon was suggested as the first diagnostic option, given the analysis of the elementary lesion as a guide sign (palpable purpura that did not disappear on diascopy), the fact that the studies were normal, and that there was no history of mushroom intake.
We present a case of leukocytoclastic vasculitis with marked and infrequent Koebner's isomorphic phenomenon in areas of scratching. This case highlights the importance of detailed clinical history taking and analysis of elementary lesions, to guide a diagnosis of dermatosis with an atypical pattern of presentation.
Please cite this article as: Amores-Martín E, Iglesias-Sancho M, Fernández-Figueras MT. Vasculitis leucocitoclástica manifestada como fenómeno de Koebner. Reumatol Clin. 2020;16:308–309.


