

Non-Steroidal Anti-Inflammatory Drugs are the cornerstone in the treatment of acute and chronic pain due to inflammation in musculoskeletal conditions. Even though adverse side-effects are associated, their use is common in the elderly patients. Our aim is to determine the prescription trend of NSAIDs, the evaluation for gastrointestinal (GI) and cardiovascular (CV) risks, and the level of agreement with prescription guidelines.
MethodsWe conducted an observation and descriptive study in a general hospital geriatrics consultation.
ResultsFrom the 231 patients only 59 patients had a NSAIDs prescription. The most frequently prescribed was Acetaminophen, in 29(49.1%) patients, Celecoxib was prescribed in 11(18.6%) patients, Piroxicam in 5(8.4%) patients, Acetaminophen plus Celecoxib plus Omeprazole in 4 (6.7%), Acetaminophen plus Piroxicam in 2 (0.3%) patients, and Acetaminophen plus Diclofenac plus Celecoxib in 1 patient (1.6%). In the Framingham risk classification there were 160/231 (69.3%) patients in Very High Risk and 71/231 (30.7%) patients in High Risk. There were no patients in Low Risk. GI Risk: 79 patients (34.1%) had a peptic ulcer disease history. There were 55/231 (23.8%) in the High GI Risk classification, 102/231 (44.1%) in Intermediate GI Risk and 74/231 (32%) in the Low Risk. The level of agreement between the prescribed versus recommended NSAIDs according the CV and GI risks was measured with a contingence table and the kappa statistic of 0.37 p=0.001.
ConclusionThere is a low level of agreement between prescribed and recommended NSAID in elderly population.
Los medicamentos antiinflamatorios no esteroideos son la piedra angular en el tratamiento del dolor agudo y crónico debido a la inflamación en las afecciones musculoesqueléticas. Aunque los efectos secundarios adversos están asociados, su uso es común en pacientes de edad avanzada. Nuestro objetivo es determinar la tendencia de prescripción de los AINE, la evaluación de riesgos gastrointestinales (GI) y cardiovasculares (CV), y el nivel de acuerdo con las pautas de prescripción.
MétodosRealizamos un estudio descriptivo y de observación en una consulta de geriatría de un hospital general.
ResultadosDe los 231 pacientes, solo 59 pacientes tenían una prescripción de AINE. El más frecuentemente recetado fue acetaminofeno, en 29 (49,1%) pacientes, celecoxib se prescribió en 11 (18,6%) pacientes, piroxicam en 5 (8,4%) pacientes, acetaminofeno más celecoxib más omeprazole en 4 (6,7%), acetaminofeno más piroxicam en 2 (0,3%) pacientes, y acetaminofeno más diclofenaco más celecoxib en un paciente (1,6%). En la clasificación de riesgo de Framingham había 160/231 (69,3%) pacientes en muy alto riesgo y 71/231 (30,7%) pacientes en alto riesgo. No hubo pacientes en bajo riesgo. Riesgo gastrointestinal: 79 pacientes (34,1%) tenían antecedentes de enfermedad de úlcera péptica. Hubo 55/231 (23,8%) en la clasificación de riesgo GI alto, 102/231 (44,1%) en riesgo GI intermedio y 74/231 (32%) en riesgo bajo. El nivel de acuerdo entre los AINE prescritos versus los recomendados según los riesgos CV y GI se midió con una tabla de contingencia y el estadístico kappa de 0,37 p=0,001.
ConclusiónExiste un bajo nivel de acuerdo entre los AINE prescritos y recomendados en la población de edad avanzada.
Non-Steroidal Anti-Inflammatory Drugs (NSAID's) are the cornerstone in the treatment of acute and chronic pain due to inflammation in musculoskeletal conditions.1 Even though adverse side-effects are associated; including gastrointestinal, cardiovascular, renal, and hematological levels have been described.2–6
Treating pain in elderly patients is a complex task, because a “one-size-fits-all” approach is neither beneficial nor safe for this population.7 Particularly in these ages,6 NSAIDs are known to produce serious side-effects, at least twice more reactions than in the younger patient. Recent data show that most physicians are unaware of potential complications associated with cardiovascular and gastrointestinal systems.8
NSAID guidelines have been established to increase physician awareness of the complications associated with NSAID use; however, some physicians either do not recognize or do not adhere to such guidelines.9
The aim of the study to determine the prescription trend of NSAIDs, the evaluation for gastrointestinal (GI) and cardiovascular (CV) risks, and the level of agreement with prescription guidelines.
MethodsStudy designAn observational cross-sectional study was conducted.
Setting and participantsPatients both sexes older than 70 years, who attended for geriatric consultation at least in two times, with a complete clinical chart, during August to October 2015, in a Northern Mexican public hospital. The study was approved by local Ethics Committee with number R-2015-1906-28.
VariablesAge, gender, history of peptic ulcer disease or gastrointestinal bleeding, smoking status and heart diseases, prescribed NSAIDs, time of use and indication were recorded from clinical chart. Systolic blood pressure measurements, blood glucose level, total cholesterol and HDL cholesterol levels of the last 6 months also were recorded. Based on the GI and CV risks calculated from clinical information we established the recommended NSAID for every patient. We had three NSAID prescription options: Acetaminophen, Acetaminophen with Naproxen and Omeprazole, and Acetaminophen with Celecoxib and Omeprazole.
MeasurementsWe assessed the CV risk from patient characteristics: patient's age, diagnosis of systemic arterial hypertension and diabetes mellitus, active smoking, high cholesterol and low HDL of the last 6 months, left ventricular hypertrophy and ischemic heart disease history. And then we classified patients risk according to used the Framingham Risk tables1–3; uses a scoring method based on the following variables: age, sex, HDL–cholesterol, total cholesterol, systolic blood pressure, smoking (yes/no), diabetes (yes/no) and left ventricular hypertrophy. (HVI) (yes/no); With this we can calculate the coronary risk at 10 years that includes: stable angina, myocardial infarction (AMI) and coronary death. In addition, according to the experts, we rate the risk as a result that can be divided into Very high risk, High risk, Moderate and Low.
The GI risk was assessed from data of patient's clinical chart: upper or low gastrointestinal bleeding, peptic ulcer disease history, use of acetylsalicylic (ASA) acid was reviewed as part of their cardioprotective treatment, the use of antiplatelet/anticoagulants drugs, either alone or in combination with ASA and the use of proton-pump inhibitors (PPIs). And then we classified patient risk as high, intermediate o low GI risk.
Study sizeIn the three-month period analysis, we revised 430 files, were 199 were excluded for incomplete clinical file information.
Statistical methodsStatistical analysis was performed using the SPSS v23 program (IBM).Quantitative variables were described in means and standard deviation; categorical ones were described in frequencies and percentages. We elaborate cross-tables to establish concordance in NSAIDs prescription by kappa statistics.
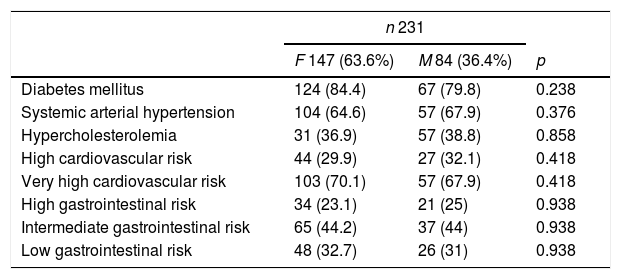
Results participantsFrom 430 files reviewed only 231 charts had CV, GI risk and other comorbidites data to be analyzed (Table 1). From the 231 patients, 180 (63.6%) were female with a mean age of 80.8 years (SD 8.04).Fifteen patients (6.5%) had null education, 14 patients (6.1%) had 4–6 years of education, and only 2 patients (0.9%) had more than 18 years of education. Fifty-two patients (22.5%) were married and 37 patients (16%) were widow.
Comorbidities.
| n 231 | |||
|---|---|---|---|
| F 147 (63.6%) | M 84 (36.4%) | p | |
| Diabetes mellitus | 124 (84.4) | 67 (79.8) | 0.238 |
| Systemic arterial hypertension | 104 (64.6) | 57 (67.9) | 0.376 |
| Hypercholesterolemia | 31 (36.9) | 57 (38.8) | 0.858 |
| High cardiovascular risk | 44 (29.9) | 27 (32.1) | 0.418 |
| Very high cardiovascular risk | 103 (70.1) | 57 (67.9) | 0.418 |
| High gastrointestinal risk | 34 (23.1) | 21 (25) | 0.938 |
| Intermediate gastrointestinal risk | 65 (44.2) | 37 (44) | 0.938 |
| Low gastrointestinal risk | 48 (32.7) | 26 (31) | 0.938 |
From the 231 files reviewed, 88(38.1%) patients disclosed no pain in clinical chart; 89 (38.5%) reported diffuse pain, 32 (13.9%) reported osteoarthritis, 5 (2.2%) painful shoulder, 5 (2.2%) oncological pain; 4 (1.7%)diabetic neuropathy, 3 patients (1.3%) ulcers, 2(0.9%)post-fracture painful syndrome, 2(0.9%) gouty arthritis, and 1 (0.4%) tension headache.
Risk factorsCV Risk: 35 patients (15.1%) were active smokers, 63 patients (27.2%) had type 2 diabetic mellitus and 75 patients (32.4%) had hypertension. In the Framingham risk classification there were 160/231 (69.3%) patients in Very High Risk and 71/231 (30.7%) patients in High Risk. There were no patients in Low Risk.
GI Risk: 79 patients (34.1%) had a peptic ulcer disease history. There were 55/231 (23.8%) in the High GI Risk classification, 102/231 (44.1%) in Intermediate GI Risk and 74/231 (32%) in the Low Risk.
Pooled NSAIDs prescribedFrom the 231 patients only 59 patients had a NSAIDs prescription. The most frequently prescribed was Acetaminophen, in 29 (49.1%) patients, Celecoxib was prescribed in 11 (18.6%) patients, Piroxicam in 5 (8.4%) patients, Acetaminophen plus Celecoxib plus Omeprazole in 4 (6.7%), Acetaminophen plus Piroxicam in 2 (0.3%) patients, and Acetaminophen plus Diclofenac plus Celecoxib in 1 patients (1.6%).
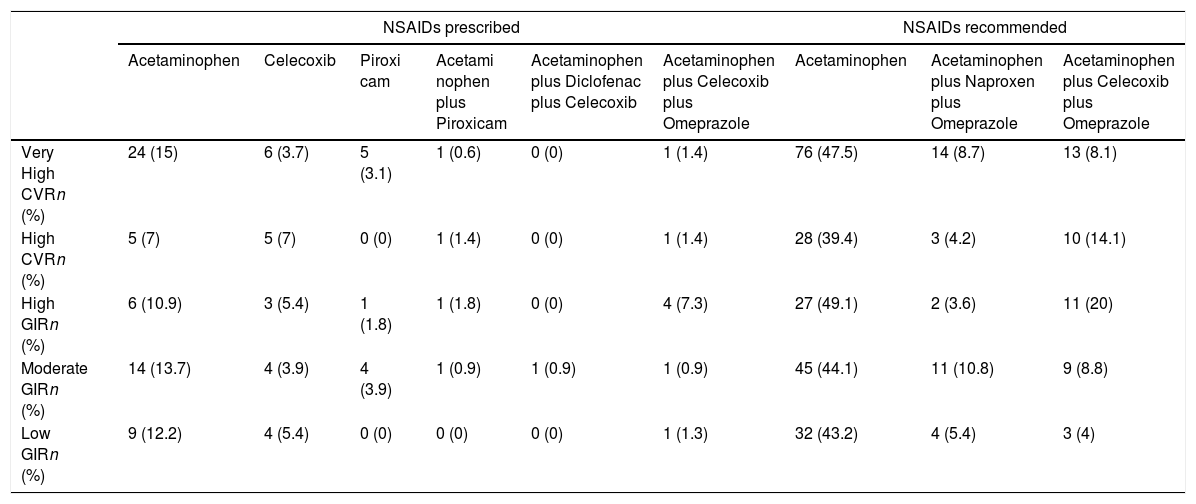
NSAID recommended by risk stratificationTable 2 Considering CV risk, in high risk patients (71/231), Acetaminophen was recommended in 28/71 patients (39.4%), Naproxen plus Omeprazole in 3/71 patients (4.2%), Naproxen plus Celecoxib in 10/71 patients (14.1%). And in very high risk patients (160/231), Acetaminophen was recommended in 76/160 patients (32.9%), Naproxen plus Omeprazole in 14/160 patients (6%), and Naproxen plus Celecoxib in 13/160 patients (5.6%).
NSAID recommended by risk stratification.
| NSAIDs prescribed | NSAIDs recommended | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Acetaminophen | Celecoxib | Piroxi cam | Acetami nophen plus Piroxicam | Acetaminophen plus Diclofenac plus Celecoxib | Acetaminophen plus Celecoxib plus Omeprazole | Acetaminophen | Acetaminophen plus Naproxen plus Omeprazole | Acetaminophen plus Celecoxib plus Omeprazole | |
| Very High CVRn (%) | 24 (15) | 6 (3.7) | 5 (3.1) | 1 (0.6) | 0 (0) | 1 (1.4) | 76 (47.5) | 14 (8.7) | 13 (8.1) |
| High CVRn (%) | 5 (7) | 5 (7) | 0 (0) | 1 (1.4) | 0 (0) | 1 (1.4) | 28 (39.4) | 3 (4.2) | 10 (14.1) |
| High GIRn (%) | 6 (10.9) | 3 (5.4) | 1 (1.8) | 1 (1.8) | 0 (0) | 4 (7.3) | 27 (49.1) | 2 (3.6) | 11 (20) |
| Moderate GIRn (%) | 14 (13.7) | 4 (3.9) | 4 (3.9) | 1 (0.9) | 1 (0.9) | 1 (0.9) | 45 (44.1) | 11 (10.8) | 9 (8.8) |
| Low GIRn (%) | 9 (12.2) | 4 (5.4) | 0 (0) | 0 (0) | 0 (0) | 1 (1.3) | 32 (43.2) | 4 (5.4) | 3 (4) |
NSAID, non-steroidal anti-inflammatory drug; CVR, cardiovascular risk; GIR, gastrointestinal risk.
Considering GI risk, in high risk patients (55/231), Acetaminophen was recommended in 27/55 patients (49.1%), Naproxen plus Omeprazole in 2/55 patients (3.6%), Naproxen plus Celecoxib in 11/55 patients (20%); in moderate risk patients(102/231), Acetaminophen was recommended in 45/102 patients (44.1%), Naproxen plus Omeprazole in 11/102 patients (10.8%), Naproxen plus Celecoxib in 9/102 patients (8.8%); and for low risk patients (74/231), Acetaminophen was recommended in 32/74 patients (43.2%), Naproxen plus Omeprazole in 4/74 patients (5.4%), and Naproxen plus Celecoxib in 3/74 patients (4.0%). Chi square 7837, p=0.347.
Of the 231 patients evaluated, 172/231 (74.5%) patients who did not receive any medication. Of those 57/172 (33.1%) they had a high CVR and 115/172 (66.9%) had a very high CVR. Chi square 1.82, p=0.176.
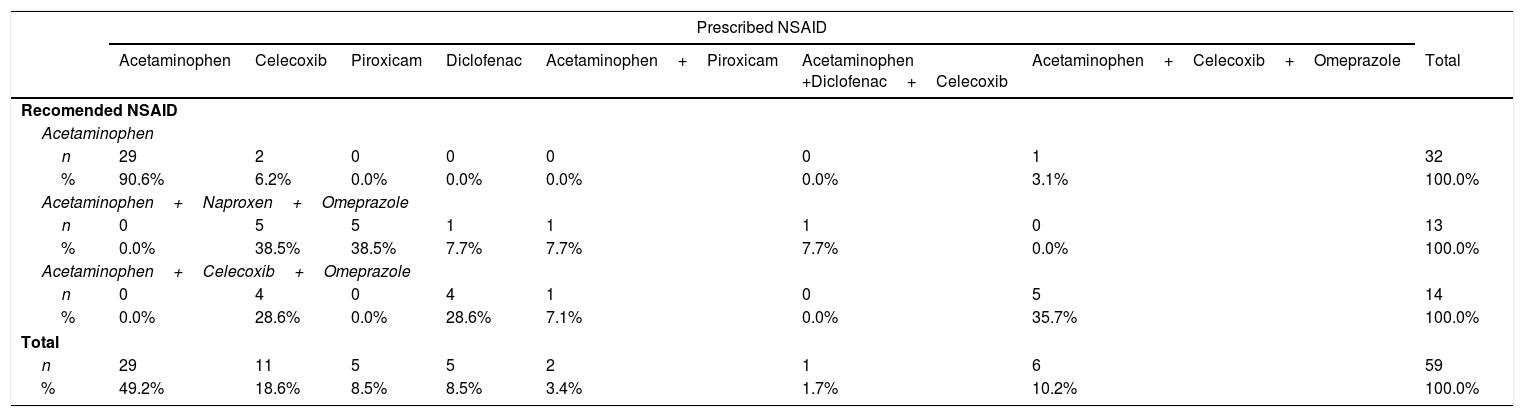
AgreementThe level of agreement between the prescribed versus recommended NSAIDs according the CV and GI risks was measured with a contingence table and the kappa statistic of 0.37 p=0.0001, Chi square75.45. See Table 3.
Prescribed vs Recommended NSAIDs according the Cardiovascular risk and Gastrointestinal risk.
| Prescribed NSAID | ||||||||
|---|---|---|---|---|---|---|---|---|
| Acetaminophen | Celecoxib | Piroxicam | Diclofenac | Acetaminophen+Piroxicam | Acetaminophen +Diclofenac+Celecoxib | Acetaminophen+Celecoxib+Omeprazole | Total | |
| Recomended NSAID | ||||||||
| Acetaminophen | ||||||||
| n | 29 | 2 | 0 | 0 | 0 | 0 | 1 | 32 |
| % | 90.6% | 6.2% | 0.0% | 0.0% | 0.0% | 0.0% | 3.1% | 100.0% |
| Acetaminophen+Naproxen+Omeprazole | ||||||||
| n | 0 | 5 | 5 | 1 | 1 | 1 | 0 | 13 |
| % | 0.0% | 38.5% | 38.5% | 7.7% | 7.7% | 7.7% | 0.0% | 100.0% |
| Acetaminophen+Celecoxib+Omeprazole | ||||||||
| n | 0 | 4 | 0 | 4 | 1 | 0 | 5 | 14 |
| % | 0.0% | 28.6% | 0.0% | 28.6% | 7.1% | 0.0% | 35.7% | 100.0% |
| Total | ||||||||
| n | 29 | 11 | 5 | 5 | 2 | 1 | 6 | 59 |
| % | 49.2% | 18.6% | 8.5% | 8.5% | 3.4% | 1.7% | 10.2% | 100.0% |
NSAID, non-steroidal anti-inflammatory drug.
We found approximately 37% of agreement in the NSAIDs prescription compared with safe prescription recommendation.9,10 Pham et al. evaluated the presence of cardiovascular diseases and how they modified the NSAIDs prescription according to national guidelines of prescription in US; they found that one third of visits involving NSAIDs prescription included a CV disease. They concluded that there is a partial implementation of the prescription guidelines in the analyzed cohort. In 2010 Lanas et al., evaluated the GI and CV risks to determine the NSAIDs prescription, they found that 15.5% of patients presented a high-risk profile, both GI and CV, and it did not altered the NSAIDs prescription.11 Al Khaja et al.12 made an audit of prescriptions issued to 2090 elderly patients (≥65 years) with hypertension or diabetic hypertension in primary care. They found a 13.5% of patients receiving NSAIDs, most frequently diclofenac instead of naproxen; and the gastro-protection was suboptimal indicated in 33.3% patients.
We found that in the geriatric consultation CV and GI risk profile was evaluated in nearly half of patient files eligible for the study. Because of the patient age-group there were no CV low-risk patients. Thus, making the lack of awareness of the CV risk profile more preoccupant. In the GI risk evaluation, the lack of using proton-pump inhibitors as a protective measure was one of the major determinants of the risk, even though the peptic and GI bleeding history reported.
Among the most prevalent diagnoses related to the NSAIDs prescription were diffuse pain and osteoarthritis. The clinical diagnoses were not evaluated, but just the inflammatory processes are prone to the use of NSAIDs. Diffuse pain has not inflammatory component, it could be part of aging-process, sarcopenia and lack of mobility, which is common in elderly patients and must be treated with Acetaminophen. In the inflammatory processes the choice is Diclofenac, but our population has predominance of High and Very High Cardiovascular Risk, so we must switch to Naproxen as a first-line NSAID, or in cases of High Gastrointestinal Risk change for Celecoxib, both accompanied by Acetaminophen and PPIs. In the other diagnoses, the use of Acetaminophen as the NSAID of choice is recommended, and more specifically in cases of Oncological pain, post-fracture pain syndrome and diabetic neuropathy, NSAIDs will not alleviate their condition, as it has neuropathic rather than inflammatory components, so that the use of NSAIDs should be controlled in these patients, since pain itself may favor overuse of NSAIDs and it is essential to explain to family members and patients themselves that gastrointestinal risks are increased in case of using NSAIDs in large doses. In these patients should be assessed the quality of life on the function, so they are candidates for management with drugs such as antiepileptics, gabapentin and pregabalin that are better tolerated in the elderly.
Acetaminophen with Naproxen and Omeprazole was not used as recommended combinations, although it has been proven in multiple studies to be effective in Inflammatory-based conditions such as Osteoarthritis and that presents less adverse effects in patients with Cardiovascular Risk, both High and Very High, is recommended in case of having intermediate and low gastrointestinal risk due to its good tolerance accompanied by PPIs. Opondo et al. reported that the overall proportion of NSAID prescriptions to the elderly with co-prescription of gastro-protective medication was 43%.13
In contrast, these patients were prescribed Piroxicam, Celecoxib, Diclofenac and their combinations between them and Acetaminophen. We understand that the guidelines for the treatment of many diseases based on inflammation recommend diclofenac as the first line, or piroxicam as a second line medication, but taking into account the basic pathologies of our patients, the average life's pain in elderly patients of drugs and their inhibitory function of prostaglandins, these drugs should be avoided, due to the high risk of high and low Gastrointestinal Bleeding, as well as Cardiovascular complications such as Acute Myocardial Infarction and Atherothrombotic events due to a decrease in the protective effect of ASA.
Patient perception also is important, because the over-the-counter (OTC) nature of most NSAIDs, patients continue taking medication without recognizing the risk.14
OTC NSAIDs are used by almost one-third of the general population. In the high-risk patients selected, one in eight patients used an OTC NSAIDs.15 OTC NSAIDs are widely available and are commonly taken without the knowledge of the prescriber.16
Patients also are unaware of the risks. Older adults who use NSAIDs may be unaware of potential risks. Counseling older adults may reduce potentially inappropriate use and increase patient risk awareness. Pharmacists can improve their role in recognizing and counseling patients on NSAIDs.17
NSAIDs should not be used indiscriminately for non-inflammatory osteoarthritis or musculoskeletal injuries, particularly in the elderly patient, in whom alternative, less toxic therapy should be sought.18
We did not explore the co-medications. The frequent co-prescription of medications which may cause detrimental interactions in elderly chronic NSAID users adds to safety concerns regarding this widely prescribed class of drugs.19
With the above and when interpreting the correlation of the use of NSAIDs in Geriatrics and the use of recommendations for the safe prescription of NSAIDs according to Gastrointestinal and Cardiovascular Risks, was found that the Cardiovascular risk in the patients of the third age was the most insignificant item taken to assess the prescription of NSAIDs.
ConclusionThere is a low level of agreement between prescribed and recommended NSAID in elderly population.
The use of the recommendations for the safe prescription of NSAIDs according to Gastrointestinal and Cardiovascular Risks, must be used in the patients of the third age for the prescription of NSAIDs.
Ethical approvalAll procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consentInformed consent was obtained from all individual participants included in the study.
FundingThis study was not funded.
Conflict of interestAll the authors state that they have not conflict of interest.


