


The aim of this study was to determine the reliability of The Osteoarthritis Knee and Hip Quality of Life questionnaire in a Columbian older adult population with knee and hip osteoarthritis.
MethodsThe methodological approach of this study was quantitative, with a cross-sectional design. Respondents completed the questionnaire with a period of 5–8 days between measurements. The psychometric properties of reproducibility, internal consistency and level of agreement of the questionnaire were determined using the intraclass correlation coefficient, Cronbach's alpha coefficient and Bland–Altman graphical analysis, respectively.
ResultsSixty-two older adults with osteoarthritis of the knee and hip aged between 57 and 82 responded to the questionnaire. Almost perfect reproducibility (ICC=.89) was found for the domain of physical activity, and substantial reproducibility (ICC=.62–.77) for the domains of pain, mental health and activities. A very satisfactory internal consistency was also obtained for the domains of mental health and physical activity (alpha=.90–.94), while that for pain was adequate (alpha=.89). As soon as the level of agreement was established, the mean of the differences in the domains of physical activity, main and mental health was −7.0, −8.0 and −6.9 points, respectively.
Discussion and conclusionsThe Osteoarthritis Knee and Hip Quality of Life questionnaire showed good psychometric properties principally in the domains of physical activity, pain and mental health. This questionnaire can be used in the clinical setting, but requires adjustment to be used in research.
El objetivo de este estudio fue determinar la confiabilidad del cuestionario The Osteoarthritis Knee and Hip Quality of Life en población adulta mayor colombiana con osteoartritis de rodilla y cadera.
MétodosEl enfoque metodológico de este estudio es cuantitativo, con un diseño de corte transversal. Los participantes diligenciaron el cuestionario con un lapso entre mediciones entre 5 a 8 días. Las propiedades psicométricas de reproducibilidad, consistencia interna y nivel de acuerdo del cuestionario se determinaron a través del coeficiente de correlación intraclase, el coeficiente alfa de Cronbach y el análisis gráfico de Bland y Altman, respectivamente.
ResultadosSesenta y dos adultos mayores con osteoartritis de rodilla y cadera, con edad entre los 57 y 82 años respondieron el cuestionario. Se encontró una reproducibilidad casi perfecta (CCI=0,89) para el dominio de actividad física; y sustancial (CCI=0,62-0,77) para los dominios de dolor, salud mental y actividades. También se obtuvo una consistencia interna muy satisfactoria en los dominios de salud mental y actividad física (alfa=0,9-0,94), mientras que la de dolor fue adecuada (alfa=0,89). En cuanto a lo encontrado con el nivel de acuerdo, el promedio de las diferencias de los dominios de actividad física, dolor y salud mental fue de –7, –8 y –6,9 puntos, respectivamente.
Discusión y conclusionesEl cuestionario The Osteoarthritis Knee and Hip Quality of Life mostró buenas propiedades psicométricas en los dominios de actividad física, dolor y salud mental, principalmente. Este cuestionario puede ser utilizado en el ámbito clínico, pero requiere ajustes para ser utilizado en investigación.
Osteoarthritis (OA) is considered to be the most common joint condition mainly affecting the older adult population.1 It is an anatomical and clinical syndrome characterised by mechanical pain, which is frequently associated with stiffness and which progressively leads to a loss of joint function.2 OA mainly affects weight-bearing joints, such as those of the lower limbs. The rate of incidence in knee joints is 240 cases per 100,000 people per year, followed by the hip with 88 cases per 100,000 people per year.3
Approximately 40% of adults over 70 have OA, and 80% of the people with this disease suffer from some type of limitation when carrying out their daily activities.4
In Colombia, one epidemiological marker of disease burden expressed in years of healthy life lost reports that 150 years healthy life are lost for every 1000 people with the disease.5 Years of health life lost to OA is among the first 20 causes of disability in women over 45 years of age.6
OA is one of the main causes of pain and disability in the world. It causes progressive impairment in functional capacity and consequently a diminishing quality of life.7 According to Neogi8 patients suffering from OA often present with chronic pain which increases with activity. As a result, people with OA lessen their participation in different activities to avoid triggering the pain. Pain therefore has a high impact on their quality of life, because it generates negative effects on their mood, their participation in social activities, recreation and even affects their sleep.
Patients with OA have to face changes in how they go about their daily life activities, bearing in mind that approximately 25% of people with this condition present with reduced functional capacity and therefore a diminished quality of life.9
Quality of life is considered to be a major trigger for measuring the effectiveness of interventions in these patients and it is therefore necessary to have tools which assess the impact of the different interventions in the patient's perception of their disease. Self-completion questionnaires are one of the tools used to assess the quality of life in patients with OA. They are a simple method, capable of evaluating the impact of the disease on the patient's life.4,10
The use of generic questionnaires such as the English Short Form Survey SF36 is common in patients with OA. This is a generic survey and one of its limitations is its low sensitivity to change.11 The Western Ontario and Master Universities Osteoarthritis Index (WOMAC) has been used worldwide to measure the quality of life of patients with OA; but it is a questionnaire which mainly measures functional capacity since it measures variables such as pain, stiffness and function and does not bear in mind aspects such as mental health and social functioning that may be affected by OA.12,13
The Osteoarthritis Knee and Hip Quality of Life (OAKHQOL) questionnaire is specifically for OA of the knee and hip but it has not been assessed in the Colombian context through interviews. This tool consists of 43 items distributed into 5 domains which include physical activity, mental health, pain, social support and social functioning. Each item is scored on an ordinal scale of 11 points, where 0 is the worst quality of life and 10 is the best quality of life. For each dimension the average score of the items contained in it are calculated.12
The aim of this study is to become aware of the reliability of the results from the tool in the Colombian context when it is applied through the use of interviews. Health professionals use interviews to attend to the users in research and clinical settings, since OA of the knee and hip is a major social and health problem in all societies, making it relevant and of general interest to adapt the existing assessment indexes to different cultures.
Material and methodsResearch designThe methodological focus of this study was quantitative, with a short cross-sectional design.
Population and sampleThe subjects had to present with at least 2 clinical criteria for OA of the hip and knee diagnosis, in accordance with the American College of Rheumatology.14 These criteria included: pain in the knees for days or months, early morning stiffness and aged over 40 years.
Participants who presented with limitations in answering the questionnaire, such as cognitive disability were excluded, as were people with an orthopaedic history in lower limbs, such as fractures.
ProceduresTwo applications of the questionnaire per participant were used with a time lapse between evaluations of 5–8 days and each application lasted 15–20min. If doubts arose from the participant during the application process they were noted and taken into account for analysis of the findings.
Data analysisTo determine reproducibility of the dimensions the intraclass correlation coefficient (ICC) was used, which was interpreted as: 1.00 perfect, .81–.99 almost perfect, .61–.80 substantial, .41–.60 moderate, .21–.40 light and .01–.20 almost insignificant.15 The level of agreement was assessed using the Bland–Altman graphical analysis method, with report of the average differences and 95% agreement limits and lastly internal consistency was determined using Cronbach's alpha, the interpretation of which corresponded to: .90–1.00 highly satisfactory, .80–.89 adequate, .70–.79 moderate, .60–.69 low, .50–.59 very low and <.50 unreliable.16 The STATA 12 software programme was used for statistical analysis.
Ethical considerationsThe Declaration of Helsinki ethical principles were adhered to during this project. Respect for the essential ethical principles of autonomy, confidentiality, beneficence, equity and justice were followed. Private participant data were only known to the researchers and were concealed during the data base construction process and their analysis. According to Resolution 008430 el there was a lower than minimum risk level in this study, because it did not include any participant intervention. All participants in the study gave their permission through signing their informed consent.
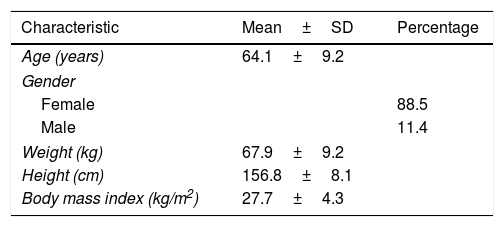
ResultsSampleThe final simple comprised 62 participants who completed the OAKHQOL questionnaire. Population characteristics are presented in Table 1.
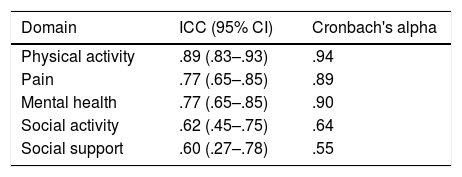
ReliabilityReproducibilityThe ICC was almost perfect for the physical activity domain, whilst the domains of pain, mental health and social activities were substantial, and the reproducibility of the social support domain was moderate (Table 2).
Reproducibility and internal consistence by questionnaire dimensions.
| Domain | ICC (95% CI) | Cronbach's alpha |
|---|---|---|
| Physical activity | .89 (.83–.93) | .94 |
| Pain | .77 (.65–.85) | .89 |
| Mental health | .77 (.65–.85) | .90 |
| Social activity | .62 (.45–.75) | .64 |
| Social support | .60 (.27–.78) | .55 |
ICC: intraclass correlation coefficient, CI: 95% confidence interval.
The domains of physical and mental health had a highly satisfactory internal consistency, whilst that of pain was adequate. Social activity and social support domains had a low and very low consistency, respectively (Table 2).
Level of agreementIn the graphic representation of the level of agreement it was observed that the average of differences of the domains of physical activity, pain and mental health were close to 0, with scores of −7.0, −8.0 and −6.9 points, respectively; for their part the social activity and social support domains had an average of differences of 6.4 and 9.3 points. Limits of agreement were broad, ranging from −50 to 50 points (Fig. 1).
, pain (B), mental health (C), social activities (D), and social support (E). Each point of data indicates the difference between the 2 measurements for one subject, the purple line represents the average agreement observed from the 2 measurements for scores of each OAKHQOL domain. The red line shows the limits of agreement above and below 95%.")
Graphical representation of Bland–Altman analysis of level of agreement of each OAKHQOL questionnaire domain. The domains are physical activity (A), pain (B), mental health (C), social activities (D), and social support (E). Each point of data indicates the difference between the 2 measurements for one subject, the purple line represents the average agreement observed from the 2 measurements for scores of each OAKHQOL domain. The red line shows the limits of agreement above and below 95%.
The results in reproducibility are similar to those found in the original research, which was determined by the French population,17 so the domains of activity and pain presented a ICC which was higher in comparison with the other domains. Regarding the domain of physical activity, reproducibility in both studies was almost perfect. The pain and social activities domains, for their part, were classified as substantial.
It may be observed that the similarity in ICC results, range between substantial and almost perfect, with the exception of the social support domain, which was classed with a moderate ICC in this study, whilst in the French version it was substantial. Another of the differences to the French study is that the mental health domain was classified as almost perfect, whilst the ICC result in this study was substantial. These differences may be due to the fact that in the French version the sample was larger compared to that of this study.
In the Spanish version12 of the questionnaire reproducibility was substantial in physical activity, pain and mental health domains, and light in social activities and social support domains. When the findings from this study were compared with those of the Spanish version some major differences were found in the social support and social activities domains which in our study were shown to have a higher reproducibility. This may be due to the form of application since in the Spanish study the questionnaire was sent via electronic mail and the participant was unable to air their doubts, whilst in this study they were able to be resolved.
Regarding internal consistency of the findings from this study, they were consistent with the French version, in that the dimensions of the social activities and the social support also present lower coefficients. However, in this study the consistency was moderate for this dimension, which may be explained by the way in which it was applied in this study, since the person in charge of explaining the questionnaire was present during its application and responded to doubts, which were able to improve the correlation between the items.17 The application using electronic mail may facilitate data collection and cover a large part of the sample more easily and quickly, but this form of application is inconsistent with the form of application of tools in the clinic or in research.
The level of agreement mainly describes the differences existing between measurements and offers an idea of the variability of the questionnaire between the different measurements. These variations between the different applications can relate to variations in the people at whom the questionnaire is conducted or the professional who explains the questionnaire, and may be due, among other factors, to the prevailing mood, fatigue, or time of day applied. The questionnaire also presents variability of measurements, and both those of the questionnaire and the people are the result of random situations.
The level of agreement enables an approach to be made to this variability determined by chance, which is important as a first step in establishing a cut-off point. From this cut-off point the variation of one questionnaire between 2 measurements will be the result of reasons other than chance, such as the research setting, an experimental design where changes would be expected to depend on intervention or on the clinical setting where changes would be expected to derive from the effectiveness of a therapeutic intervention.18
According to the graphic Bland–Altman analysis it may be proven that the 5 domains present an average of differences close to 0, which indicates that the difference in the score obtained in the first and second measurement was approximately 10 points; this is acceptable for a questionnaire with scores between 0 and 100.19 It should be considered that the maximum difference allowed between scores of both applications of the questionnaire is a clinical, not a statistical decision.20
The difficulty with the OAKHQOL questionnaire is that its agreement is determined in this case by the agreement limits, which show the maximum and minimum range of variation of the questionnaire and these were very extensive, with 5 domains between −50 and 50 points which means that the questionnaire in total may vary by around 100 points due to chance. In the terms previously mentioned this meant that changes under but close to 100 points in the research area could be due only to chance.20
Since the average of the differences is close to 0, this indicates that the error is approximately 10 points, which is acceptable to our interpretation, this questionnaire may be used in clinical practice, but in research more reliable measures are required, with fewer differences between the measurements to measure the impact of therapeutic interventions with quality of life as a dependent variable in older adults suffering from OA of the hip and knee. As a result this questionnaire could be the most appropriate one.
One limitation of this study is its small sample size and as a result all the participants included in this research may not be sufficiently representative of the adult population with OA of the hip and knee in Colombia.
ConclusionsThe OAKHQOL questionnaire proved to have good psychometric properties in the domains of physical activity, pain and mental health, but in the domains of social activities and social support results were less reliable when it was applied through interview format. The variability of the questionnaire between measurements shows that it may be used in the clinical filed, but its use in research would have major implications.
Conflict of interestsNone.
Please cite this article as: Salas-Vargas S-C, Rodríguez-Grande E-I. Confiabilidad de un cuestionario específico para evaluar calidad de vida en personas con osteoartritis. Reumatol Clin. 2021;17:279–283.


