




To: (1) describe the distribution of the public sector rheumatologists; (2) identify variables on which the workload in Rheumatology depends; and (3) build a predictive model on the need of rheumatologists for the next 10 years, in the Community of Madrid (CM).
MethodologyThe information was obtained through structured questionnaires sent to all services/units of Rheumatology of public hospitals in the CM. The population figures, current and forecasted, were obtained from the National Statistics Institute. A predictive model was built based on information about the current and foreseeable supply, current and foreseeable demand, and the assumptions and criteria used to match supply with demand. The underlying uncertainty in the model was assessed by sensitivity analysis.
ResultsIn the CM in 2011 there were 150 staff rheumatologists and 49 residents in 27 centers, which is equivalent to one rheumatologist for every 33280 inhabitants in the general population, and one for every 4996 inhabitants over 65 years. To keep the level of assistance of 2011 in 2021 in the general population, it would be necessary to train more residents or hire more rheumatologists in scenarios of demand higher than 15%. However, to keep the level of assistance in the population over 65 years of age it would be necessary to train more residents or hire more specialists even without increased demand.
ConclusionsThe model developed may be very useful for planning, with the CM policy makers, the needs of human resources in Rheumatology in the coming years.
En la Comunidad de Madrid (CM): a) describir la distribución de reumatólogos del sector público; b) identificar las variables de las que depende la carga de trabajo en Reumatología, y c) construir un modelo predictivo sobre la necesidad de reumatólogos para los próximos 10 años.
MetodologíaLa información se obtuvo mediante cuestionarios estructurados enviados a todos los servicios/unidades de Reumatología de los hospitales públicos de la CM. Las cifras y estimaciones de la población se obtuvieron del Instituto Nacional de Estadística. Se construyó un modelo predictivo que se basa en información sobre la oferta actual y previsible, la demanda actual y previsible, y las asunciones y criterios utilizados para adaptar la oferta a la demanda. La incertidumbre subyacente en el modelo se evaluó mediante análisis de sensibilidad.
ResultadosEn la CM en 2011 había 150 reumatólogos de plantilla y 49 residentes distribuidos en 27 centros, que equivale a un reumatólogo activo por cada 33.280 habitantes en la población general, y por cada 4.996 habitantes mayores de 65 años. Para mantener el nivel de asistencia de 2011 en 2021 en la población general, solo sería necesario formar más residentes o contratar más reumatólogos en escenarios de aumento de la demanda superior al 15%. Sin embargo, para mantenerlo en la población mayor de 65 años, sería necesario formar más residentes o contratar más especialistas, aún sin aumento de la demanda.
ConclusionesEl modelo desarrollado es muy útil para planificar con los responsables de la CM las necesidades de recursos humanos en Reumatología en los próximos años.
Rheumatology has established itself as a specialty due to the relevance and prevalence of the diseases dealt with,1,2 as well as for the development of specific diagnostic and therapeutic techniques.3–5 The specialty has undergone significant changes over the past years and is expected to continue this process in the future. Thus, new diagnostic techniques and the availability of new drugs allow addressing conditions that were difficult to treat for years, radically altering the management of these diseases. At the same time, the increased prevalence of rheumatic diseases and the higher levels of information in the population could lead to an increase in demand for services provided by rheumatologists. Moreover, demographic changes will also affect the prevalence of some diseases seen by the specialty. Since many of the rheumatic diseases are related to age, the progressive aging of the population points to a continuous increase in the number of patients with rheumatic diseases. Consequently, demand for attention of these conditions could overwhelm the ability of rheumatologists to develop the necessary services quickly, fairly and efficiently.
In view of this situation, many questions have arisen on the future of Rheumatology in the Community of Madrid (CM), especially on the needs in the number of rheumatologists to provide high quality and equitable healthcare to the population of Madrid. For these reasons, the Society of Rheumatology of the Community of Madrid (SORCOM) has taken the initiative to carry out a study to answer the questions that generate most uncertainty. This study seeks to address these questions by building a predictive model based on information about the current and foreseeable resources and the foreseeable demand, and the assumptions and criteria used to match supply to demand. Consequently, the objectives of our study are: (a) to describe the distribution of public sector rheumatologists in the CM based on their professional and socio-demographic characteristics, (b) to identify demographic aspects, prevalence, and technological data on which workload in Rheumatology depends in the CM, and (c) to build a predictive model of the need for rheumatologists in the CM for the next 10 years, based on the findings of the above objectives.
MethodsTo describe the distribution of public sector rheumatologists in the CM based on their professional and demographic characteristics, an electronic questionnaire was developed (in Excel) with the variables of interest. The variables of interest were decided at a formal meeting to which all Heads of Service and/or persons responsible for Rheumatology Units of the CM were invited. Representatives from 13 rheumatology services of the CM attended, of which 11 were heads of Service or Unit. The meeting began with a list of variables proposed by two of the investigators (PLM and AJBB) and participating rheumatologists set final variables of interest in consensus with all participants. Finally, the variables considered of interest to rheumatologists were age, gender, professional category, the sector in which they worked and the type of contract they had. For residents, the variables were age, gender and category. To identify and describe the population of rheumatologists, the questionnaire was sent by email to those responsible for Rheumatology Units of the 27 public Units in the CM with a rheumatology service or at least one rheumatologist per unit or service, who completed the data from all rheumatologists from his or her center. A database with data received from all centers was then developed. Means and standard deviations were used to describe continuous variables and proportions for describing categorical variables.
The identification of the variables on which the Rheumatology workload depends in the CM was conducted at the meeting mentioned above, in which the activities that pose a substantial part of the work of rheumatologists were considered. Finally, we considered 2 groups of activities whose workload should be known and predicted: assistance care (conditions and clinical procedures) and non-assistance care (e.g. Research, teaching). With the variables set we developed an electronic questionnaire, also completed by those responsible for the departments. To estimate the workload of each variable in the set of the CM, we calculated the weighted average number of rheumatologists in each center.
For the demographic variables we used the population projections by age group of the National Institute of Statistics (NIE) to the last available year (2021).6 In addition, we estimated the population projection data from the 2011 census,7 assuming that the annual population increase is the same as in the population projections of NIE.
To predict the needs of rheumatologists in the CM for the next 10 years, we designed and built a predictive model in Excel whose calculation engine is based on information on the supply of rheumatologists, the demand for care and the assumptions and criteria used to adapt supply to demand. The model assigns rheumatologists whose age is unknown (one attending and 24 residents) an age obtained at random from rheumatologists in the same category of known age. The assumptions consist in values applied when the variable is not known or may change. For example, the number of residents that graduates each year, the effect of new technologies, the retirement age of rheumatologists or increases or decreases in the incidence of some diseases. The criteria consist of the explicit definition of the indicator you want to meet. For example, the desired number of rheumatologists per 100000 inhabitants of the general population or over 65 years. Mathematically combining the supply, demand, assumptions and criteria, the model identifies the number of necessary rheumatologists for the chosen year and that must be formed per year until the chosen year. Fig. 1 shows the interface of the model.

The model allows to estimate the number of rheumatologists available and needed every year until 2021. This article presents the estimates for the year 2021. To account for uncertainty in the assumptions underlying the model, we performed a sensitivity analysis that includes three scenarios: baseline case (more reasonable estimate), the most favorable case (lower estimated demand variables) and the worst case (high estimated demand variables). With these estimates, there are 3 scenarios that map the range of probability within which real needs are found.
Since this study does not include data from patients, it was not necessary to subject it to evaluation by an ethics committee.
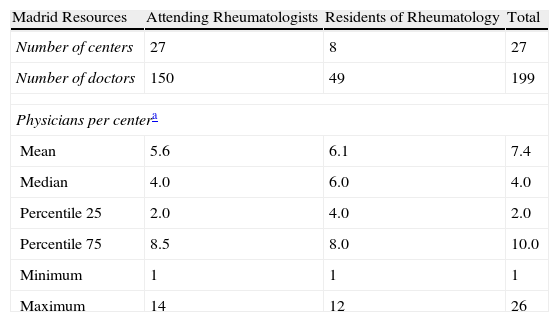
ResultsCurrent Population of Rheumatologists in the Public Sector in the Community of MadridIn the CM there are 150 attending rheumatologists in 27 centers. Additionally, 8 schools have residents, 49 being the total number of residents in the CM (Table 1). Given the CM population, according to the census of 2011, in the CM there is one active rheumatologist for every 33280 inhabitants in the general population (3 rheumatologists per 100000), and for every 4996 persons over 65 years of age (20 rheumatologists per 100000 persons over 65 years).
Rheumatologists in the Community of Madrid in 2011.
| Madrid Resources | Attending Rheumatologists | Residents of Rheumatology | Total |
| Number of centers | 27 | 8 | 27 |
| Number of doctors | 150 | 49 | 199 |
| Physicians per centera | |||
| Mean | 5.6 | 6.1 | 7.4 |
| Median | 4.0 | 6.0 | 4.0 |
| Percentile 25 | 2.0 | 4.0 | 2.0 |
| Percentile 75 | 8.5 | 8.0 | 10.0 |
| Minimum | 1 | 1 | 1 |
| Maximum | 14 | 12 | 26 |
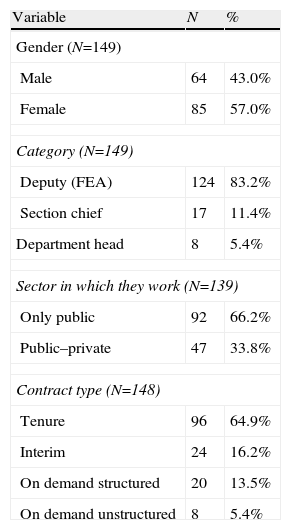
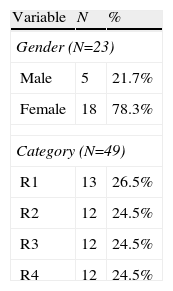
Attending rheumatologists are between 30 and 68 years of age, mean age 48.2 years (SD=8.6 years). 57% are women, the majority (83.2%) are attending medical specialists, only 64.9% have tenure, and 33.8% also work in the private sector (Table 2). 39.1% of rheumatologists who are not tenured are working in the private sector, while this proportion is 31.2% in those with tenure. Residents have between 25 and 35 years old, mean age 28.6 years (SD=2.3 years), and 78.3% were women (Table 3).
Attending Rheumatologists in the Community of Madrid in 2011 (N=150).
| Variable | N | % |
| Gender (N=149) | ||
| Male | 64 | 43.0% |
| Female | 85 | 57.0% |
| Category (N=149) | ||
| Deputy (FEA) | 124 | 83.2% |
| Section chief | 17 | 11.4% |
| Department head | 8 | 5.4% |
| Sector in which they work (N=139) | ||
| Only public | 92 | 66.2% |
| Public–private | 47 | 33.8% |
| Contract type (N=148) | ||
| Tenure | 96 | 64.9% |
| Interim | 24 | 16.2% |
| On demand structured | 20 | 13.5% |
| On demand unstructured | 8 | 5.4% |
| Age (N=149) | Years Old |
| Mean | 48.2 |
| Standard deviation | 8.6 |
| Median | 49.0 |
| Percentile 25 | 41.0 |
| Percentile 75 | 53.8 |
| Minimum | 30.0 |
| Maximum | 68.0 |
Residents of Rheumatology in the Community of Madrid in 2011 (N=49).
| Variable | N | % |
| Gender (N=23) | ||
| Male | 5 | 21.7% |
| Female | 18 | 78.3% |
| Category (N=49) | ||
| R1 | 13 | 26.5% |
| R2 | 12 | 24.5% |
| R3 | 12 | 24.5% |
| R4 | 12 | 24.5% |
| Age (N=25) | Years Old |
| Mean | 28.6 |
| Standard deviation | 2.3 |
| Median | 28.0 |
| Percentile 25 | 27.0 |
| Percentile 75 | 29.0 |
| Minimum | 25.0 |
| Maximum | 35.0 |
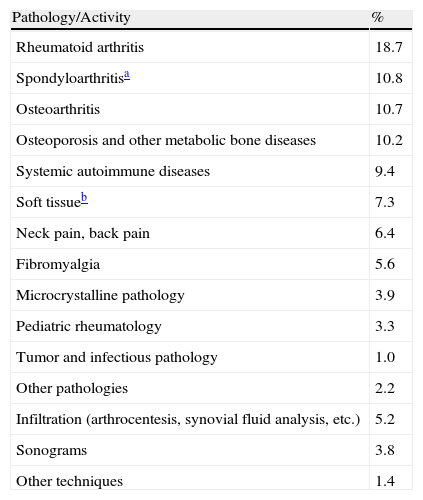
78.4% of the workload performed by rheumatologists is assistance care. Table 4 shows the care burden posed by different conditions and the techniques performed. Diseases involving a higher workload are rheumatoid arthritis (18.7%), spondyloarthritis (10.8%) and osteoarthritis (10.7%). Techniques account for 10.4% of the burden of care.
Workload of Assistance Care.
| Pathology/Activity | % |
| Rheumatoid arthritis | 18.7 |
| Spondyloarthritisa | 10.8 |
| Osteoarthritis | 10.7 |
| Osteoporosis and other metabolic bone diseases | 10.2 |
| Systemic autoimmune diseases | 9.4 |
| Soft tissueb | 7.3 |
| Neck pain, back pain | 6.4 |
| Fibromyalgia | 5.6 |
| Microcrystalline pathology | 3.9 |
| Pediatric rheumatology | 3.3 |
| Tumor and infectious pathology | 1.0 |
| Other pathologies | 2.2 |
| Infiltration (arthrocentesis, synovial fluid analysis, etc.) | 5.2 |
| Sonograms | 3.8 |
| Other techniques | 1.4 |
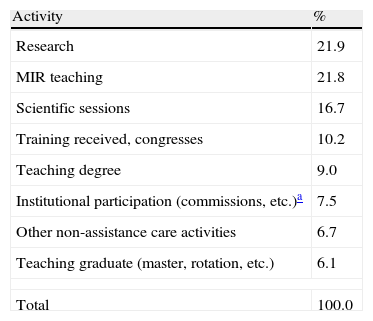
Non-assistance care performed by rheumatologists is 21.6% of their workload. Table 5 shows the activities of non-assistance workload. The activities that lead to increased workload are research (21.9%) and teaching medical interns and residents (MIR) (21.8%).
Non-assistance Care.
| Activity | % |
| Research | 21.9 |
| MIR teaching | 21.8 |
| Scientific sessions | 16.7 |
| Training received, congresses | 10.2 |
| Teaching degree | 9.0 |
| Institutional participation (commissions, etc.)a | 7.5 |
| Other non-assistance care activities | 6.7 |
| Teaching graduate (master, rotation, etc.) | 6.1 |
| Total | 100.0 |
Assuming that 12 residents will graduate per year, half of the residents remain in the CM and the retirement age is 65, in 2021 there will be 225 active rheumatologists in the CM. Considering the population growth estimated from census data, there will be one active rheumatologist for every 28954 persons in the general population (3.5 rheumatologists per 100.00 inhabitants), and for every 5447 persons aged 65 years (18.4 rheumatologists per 100.00 inhabitants over 65 years).
In the baseline scenario it is considered that the increased demand will be due to a population growth and increased demand for care of 15%. To maintain the level of assistance of 2011 in the general population, in 2021 it would be necessary to have 225 rheumatologists, which coincides with the number of rheumatologists that the model predicts that there will be by that year with the assumptions made. To maintain the level of assistance to the population over 65 years 282 rheumatologists would be needed, falling 57 short and, therefore, training would have to increase to 23 rheumatologists per year.
The most favorable scenario considered that the increased demand will be due solely to an increase of the population, with no change in the demand for care. In this scenario, it would take 196 rheumatologists in 2021 to keep the general population with the same level of support as in 2011, so current levels are more than enough and only 29 new graduates would be needed (6 new rheumatologists per year). To maintain the level of assistance to the population over 65 years 245 rheumatologists would be needed, so currently 20 are needed (16 new rheumatologists annually).
The worst case scenario considered that the increased demand will be due to a population growth and increased demand for care of 30%. In this scenario, it would take 254 rheumatologists to maintain the current level of support in the general population in 2021, so 29 more rheumatologists are needed (18 rheumatologists graduating annually). To maintain the level of assistance to the population over 65 years of age, 319 rheumatologists would be needed, currently lacking 94 and, therefore, 31 new rheumatologists per year would need to graduate.
Figs. 2 and 3 show the number of rheumatologists per 100000 inhabitants over the period considered (supply) and those required to maintain the same level of assistance in the 3 demand scenarios (baseline, most favorable and least favorable) in the general population and in the population over 65 years of age, respectively. The assumptions are maintaining the current rate of 12 new residents per year, 50% of residents remaining in the CM and a retirement age of 65. Throughout the period the number of active rheumatologists (supply) exceeds the number of rheumatologists needed to maintain the same level of care in the general population in the baseline scenario (15% increase in demand) and the most favorable scenarios (no increase in demand), but not in the least favorable scenario (30% increase in demand) (Fig. 2). However, the number of active rheumatologists at any time during the period (2012–2021) will be insufficient to maintain the same level of assistance care in the population over 65 years in the 3 demand scenarios (Fig. 3).

Prediction of demand and supply of rheumatologists until 2021. Criteria: same level of care to the general population in 2011. Rheumatologists per 100000 inhabitants Demmand Supply Demand Demand: unchanged Year.
Assumptions: 12 new residents per year, 50% of residents remain in the CM and the retirement age is 65 years. “Demand: +15%” baseline scenario, assuming an increase in health care demand of 15%. “Demand unchanged” best scenario: assuming no change in the demand for care. “Demand: +30%” worst-case scenario, assuming an increase in health care demand of 30%.

Prediction of demand and supply of rheumatologists until 2021. Criteria: same level of assistance to the population over 65 than in 2011. Rheumatologists per 100000 inhabitants over 65 years of age Demmand Demand Demand: unchanged Supply Year.
Assumptions: 12 new residents per year, 50% of residents remain in the CM and the retirement age is 65 years. “Demand: +15%” baseline scenario, assuming an increase in health care demand of 15%. “Demand unchanged” best scenario: assuming no change in the demand for care. “Demand: +30%” worst-case scenario, assuming an increase in health care demand of 30%.
The lack of accurate knowledge on the situation and forecast of human resources in Rheumatology led the SORCOM to formulate questions about the future of Rheumatology in the CM, especially about the needs in the number of rheumatologists that allow for health care quality and equal access for the population of Madrid. The first obstacle to answering these questions is that the exact number of rheumatologists in the CM and age distribution is unknown. The methodology used to determine the number of rheumatologists in the CM, and their distribution according to their professional and socio-demographic characteristics, provides accurate information that allows to overcome such an obstacle. One of the strengths of this study is that all the centers in the CM in which there is at least one rheumatologist have responded.
According to the findings of this study, in 2011 the CM had 3.0 active rheumatologists per 100000 persons in the general population. This figure is higher than that obtained in a previous study by the Ministry of Health, which estimated the number of rheumatologists in the CM in 2009 at 2.1 rheumatologists per 100000.8 This difference is because this study includes residents and the Ministry only included attending rheumatologists. If we only had considered attending rheumatologists, the figure would be 2.3 rheumatologists per 100000 inhabitants. This small difference could be due to the fact that this SORCOM study uses data from 2011 an the Ministry study used data from 2009.
The number of rheumatologists per unit of population in the CM is higher than the UK (0.9/100000 inhabitants),9 the U.S. (1.7/100000 inhabitants)10 or the province of Ontario in Canada (1.2/100000 inhabitants),11 although this should be interpreted with caution due to likely under-or overestimation bias that may occur due to the methodology used in the different studies. Moreover, the number of rheumatologists in the CM is much higher than that recommended by the Spanish Society of Rheumatology (SER) in their standards of quality of care,12 which provides that the maximum number of people per rheumatologist should be 40000–50000. Among the factors that could explain a higher density of rheumatologists in the CM per unit of population, perhaps the most relevant is that many CM centers are national referral centers where patients are derived from other regions. Another reason could be the high number of centers with MIR teaching ability, which makes the CM have one resident for every 3 attending rheumatologists. Another possible explanation could be related to the greater burden of research and teaching activities of rheumatologists in the CM, compared to other communities.
Moreover, the findings on the description of rheumatologists suggest, as observed in other specialties,13 a feminization of Rheumatology, as the proportion of women in the population of residents (78.3%) is higher than what is currently seen in rheumatologists (57.0%).
The predictive model developed allows us to estimate the number of available rheumatologists and those that will be needed from 2011 to 2021. The model works through the interaction of the information contained or assumed in 4 modules: supply, demand, assumptions (on supply and demand) and criteria. The variable information of each of the modules can be changed by the user, so as to constitute a useful tool for allowing the user to build numerous scenarios that can occur now or in the future. The methodological robustness of the model is that the database contains the 199 rheumatologists who are in the CM, the population figures until 2021 in the CM, the proportional workload of the most relevant rheumatological conditions, and some mathematics formulations to apply with different assumptions and criteria.
With reasonable assumptions, the forecast for 2021 indicates that only forming more residents or hiring more rheumatologists would be needed to maintain the level of assistance in the large increase in general population and demand scenarios (over 15%). However, to maintain the same level of assistance in the population over 65, it would be necessary to train more residents or hire more specialists, even without increased demand.
A limitation of the study is the lack of data on the age of 25 rheumatologists, which in principle could be a limitation for the proportion of rheumatologists who will be retired in a given year in the predictive model. However, given that 24 of the rheumatologists of unknown age are residents and the model is until 2021, none would be retired by this year, so it constitutes a minor limitation that did not affect the predictions model. In any case, the model assigns rheumatologists whose age is unknown an age collected at random from rheumatologists of known age in the same level or category. This way to solve the lack of information on age is based on the assumption that the age distribution of rheumatologists’ known age is similar to the age distribution of rheumatologists whose age is unknown.
In summary, this study can be useful for planning with officials of the Ministry of Health of the CM the need for graduate medical training, and assess the need for human resources in the area of Rheumatology. Furthermore, the model may make changes in the variables, assumptions, and criteria, which is adaptable to the clinical, technological, sociological or demographic environment, users assumptions and modifications in the criteria.
Ethical ResponsibilitiesProtection of People and AnimalsThe authors declare that experiments have not been done on humans or animals.
Data ConfidentialityThe authors state that no patient data appears in this article.
Right to Privacy and Informed ConsentThe authors state that no patient data appears in this article.
FinancingThe study was funded by Pfizer Spain.
Conflict of InterestThe authors declare no conflict of interest.
We express our appreciation to the following centers who provided data on available human resources and workload: Canto Blanco Hospital, Hospital Carlos III, Central Hospital of Defense “Gómez Ulla”, Hospital Clinico San Carlos, Hospital of the Henares, El Tajo Hospital, Southeast Hospital, Hospital El Escorial, Fundación Jiménez Díaz Hospital, Hospital General Universitario Gregorio Marañón, Hospital Infanta Cristina, Infanta Leonor Hospital, Hospital Infanta Sofia, Hospital Infantil Universitario Niño Jesús, Hospital Universitario 12 de Octubre, Hospital Universitario de Fuenlabrada, Getafe University Hospital, University Hospital of Móstoles, Hospital Universitario Fundación Alcorcón, Hospital Universitario La Paz, Hospital Universitario La Princesa, Prince of Asturias University Hospital, Hospital Universitario Puerta de Hierro, Hospital Universitario Ramón y Cajal, University Hospital St. Cristina, Hospital Universitario Severo Ochoa and Provincial Rehabilitation Institute. Finally, we thank Pfizer Spain for their assistance in financing the project.
Please cite this article as: Lázaro y De Mercado P, Blasco Bravo AJ, Lázaro y De Mercado I, Castañeda S, López Robledillo JC. La Reumatología en la Comunidad de Madrid: disponibilidad actual de reumatólogos y necesidades futuras aplicando un modelo predictivo. Reumatol Clin. 2013;9:353–358.


