






The scapholunate ligament complex is a set of ligaments that provide attachment between the scaphoid and lunate bones of the carpus. It is divided into 3 components: dorsal, volar and secondary stabilisers. Of these, the dorsal is the thickest and strongest, and its rupture is the most important clinically and biomechanically1. Its rupture is secondary to trauma, although it can also rupture atraumatically in chronic gout. Diagnosis is often delayed, as it is a clinically and radiologically underdiagnosed finding due to its lack of specificity: plain radiography may be normal in the acute setting2 and is the test of choice. Over time, there is a diastasis between the lunate and the scaphoid greater than 3 mm on the posteroanterior wrist plain radiograph3. This condition predisposes to the development of early wrist osteoarthritis secondary to carpal instability, following a pattern known as SLAC wrist (ScaphoLunate Advanced Collapse)4. Full characterisation of the degree and severity of ligamentous injury is assessed with wrist MRI4,5. Based on the patient’s age and activity, a conservative or surgical approach may be considered3,6.
The case presented is that of a 30-year-old left-handed male who consulted for episodes of intermittent chronic pain in the dorsal aspect of the left wrist, which partially subsided after taking anti-inflammatory drugs. The condition began following an accidental fall from his height 2 years earlier, for which he did not consult. A posteroanterior wrist X-ray showed a scapholunate diastasis of 3.5 mm and a rotatory subluxation of the scaphoid (Fig. 1). The study was completed with ultrasound and magnetic resonance imaging (Figs. 2 and 3), which demonstrated a complete rupture of the dorsal component of the scapholunate ligament. The patient was referred to the Hand Unit for consultation, where surgical treatment with arthroscopic ligamentoplasty was decided.
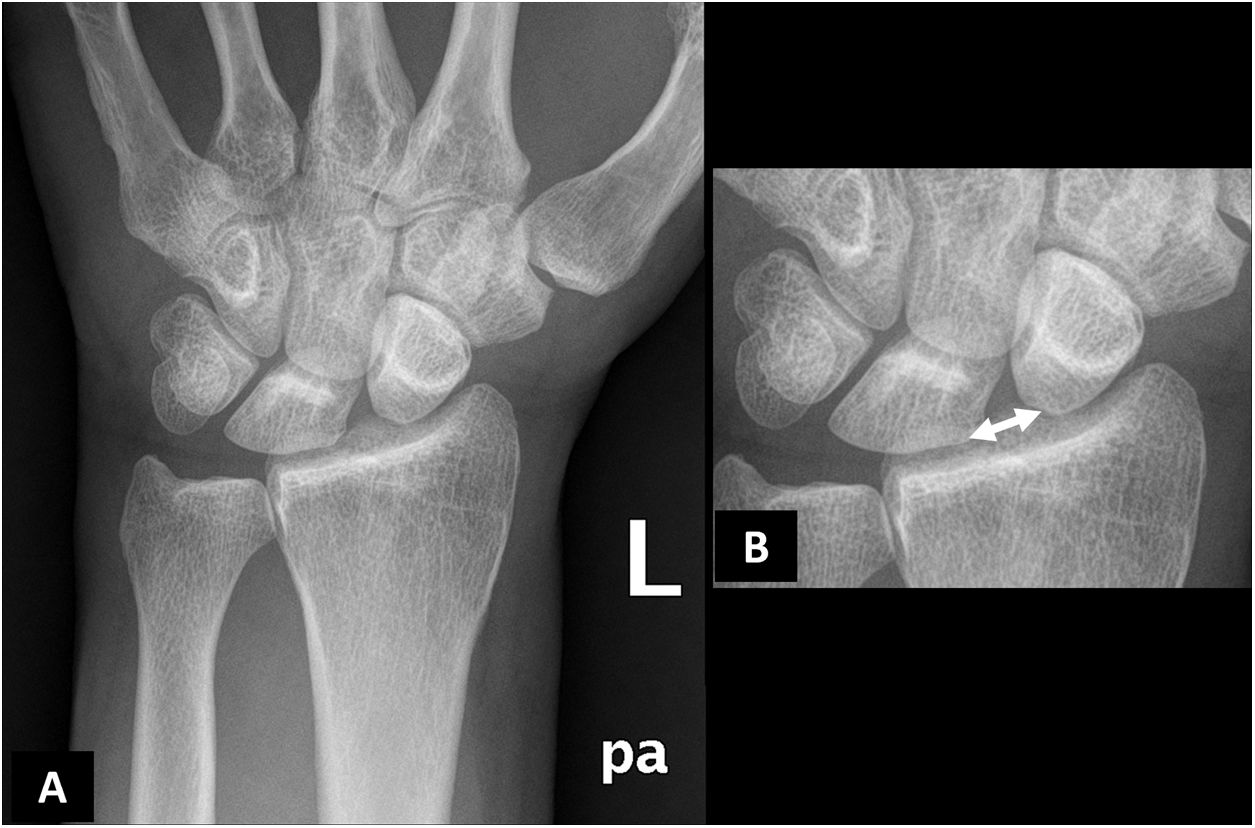
Posteroanterior plain radiograph of the left wrist (A) with magnified detail (B). There is a significant diastasis between the lunate and scaphoid bones of the carpus (double-headed arrow), which in the manual measurement was 3.5 mm. In addition, a rotatory subluxation of the scaphoid bone (B) is seen, which is an indirect indicator of scapholunate ligament injury, although it is visible in other injuries of different wrist stabilisers.
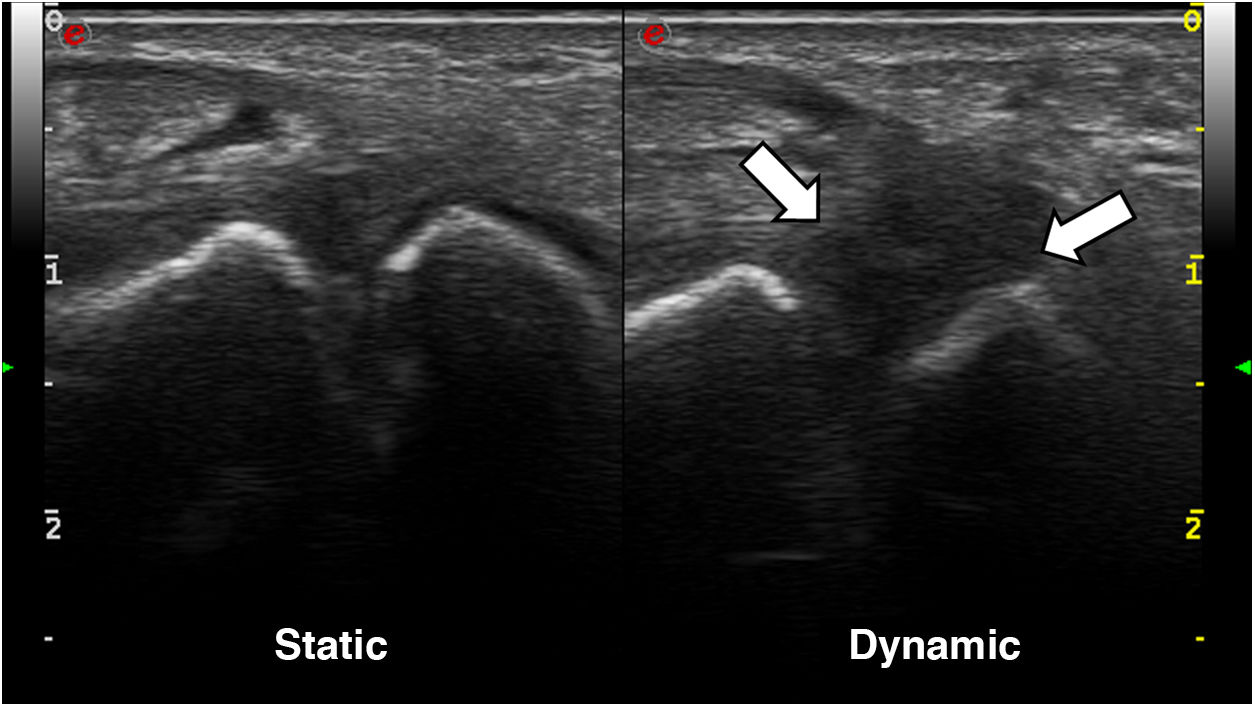
Ultrasound images of the wrist with a high-frequency linear probe; dorsal approach. In the static scan (left image), the scapholunate space appears to be preserved, although a certain hypoechogenicity of the scapholunate ligament can be sensed. However, in the dynamic scan (right image), there is a marked hypoechogenicity with significant scapholunate diastasis, without identifying the ligament with definition, in the context of its rupture.
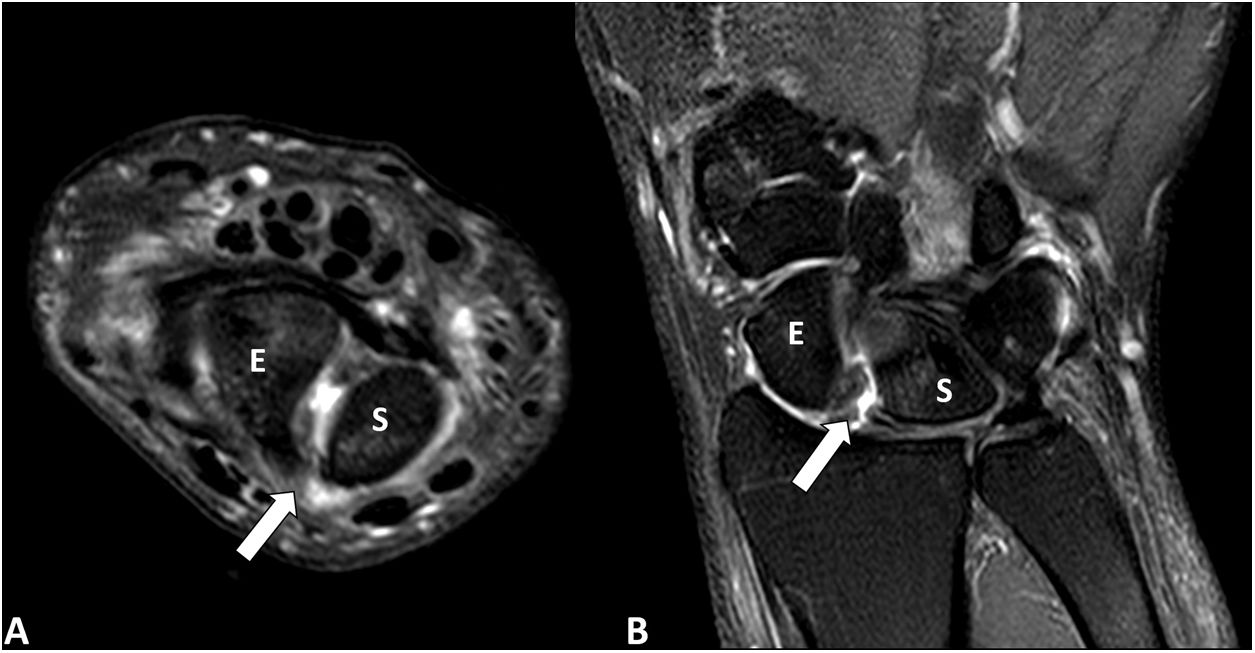
Magnetic resonance imaging. Axial (A) and coronal (B) images of the left wrist in T2-weighted sequences with fat suppression (SPAIR). There is a complete rupture of the dorsal portion of the scapholunate ligament (arrow) producing a significant diastasis between the scaphoid bone (E) and the lunate (S) with minimal effusion and signs of synovitis. There are no foci of MRI signal similar to bone oedema suggestive of inflammation/arthritis or significant osteoarthritic changes.
The scapholunate ligament is a fundamental element in the stability of the wrist. Its rupture is not particularly uncommon and is usually represented in all imaging tests. Therefore, all specialists involved in the management of these patients should be familiar with the radiological semiology of this entity.
Conflict of interestsNone of the authors have any conflict of interests to declare.
Please cite this article as: Herrán de la Gala D, Sáenz Aldea M. Ligamento escafosemilunar: una estructura fundamental en la estabilidad de la muñeca. Reumatol Clin. 2022;18:186–187.


