






To describe the objectives and methods of the Spanish Society of Rheumatology primary Sjögren syndrome (pSS) registry (SJOGREN-SER).
MethodsThis is a multicenter descriptive transversal study of a cohort of pSS patients fulfilling European/American consensus criteria collected from Rheumatology clinics all over Spain. Patients were included by randomisation from an anonymised list provided by every department. Data were collected by reviewing clinical records and an interviewing the patients. Two hundred and ninety eight variables were investigated: epidemiological, clinical, serological characteristics, treatments and complications. Informed consent was obtained and local ethics committees approved the study. Variables were analyzed by descriptive statistical methods, using means, medians, and rates, with their deviations and interquartile ranges (p25–p75).
ResultsA total of 3 rheumatology departments participated in the registry. A total of 437 patients were included. And 95% of them were women, with a median age of 58. Median age at pSS's diagnosis was 50 years. Dryness symptoms (95%) were the most frequent complaint and anti-Ro/SS-A were present in 94% of the cases. Only 27% of the patients fulfilled the new 2012 SICCA-ACR classification criteria.
ConclusionsSJOGREN-SER has been designed in order to characterize a representative pSS Spanish cohort, in clinical daily practice, to analyze the magnitude and distribution of its manifestations, activity, accumulated damage and therapeutic management of the disease. This will allow broadening the knowledge of this disease and plan strategies of action in pSS.
Describir los objetivos y metodología del registro de síndrome de Sjögren primario (SSp) de la Sociedad Española de Reumatología (SJOGREN-SER).
MétodosEstudio transversal descriptivo multicéntrico de pacientes con SSp que cumplen los criterios de clasificación del consenso europeo-americano del 2002 atendidos en servicios de reumatología españoles. Cohorte elaborada a partir de la selección al azar de pacientes con SSp. Los datos se obtuvieron de la historia clínica y por entrevista médica al paciente el día de la inclusión en el estudio. Se recogieron 298 variables agrupadas en características epidemiológicas, clínicas, serológicas y terapéuticas, así como diferentes desenlaces reportados por el paciente. El estudio fue aprobado por los CEIC locales y los pacientes firmaron un consentimiento informado. Para el análisis de los datos se utilizó estadística descriptiva, se analizaron medias, medianas y frecuencias, con sus respectivas desviaciones y rangos intercuartílicos de las variables recogidas (p25-p75).
ResultadosHan participado 33 centros españoles. El número de pacientes incluidos es de 437, la mayoría mujeres (95%), con una mediana de edad al diagnóstico de SSp de 50 años. La mediana de edad de esta cohorte es de 58 años. La mayoría de los pacientes (95%) presenta síndrome seco y hasta el 94% anti-Ro positivo. Un total de 119 pacientes (27%) cumplen los nuevos criterios de clasificación SICCA-ACR de 2012.
ConclusionesSJOGREN-SER ha sido diseñado con el fin de caracterizar una cohorte representativa de pacientes con SSp en nuestro país, en situación de práctica clínica habitual, para analizar la magnitud y distribución de sus manifestaciones, la actividad, el daño acumulado y el manejo terapéutico de la enfermedad. Esto nos permitirá ampliar y actualizar el conocimiento sobre esta enfermedad y planificar estrategias de actuación en el SSp.
Primary Sjögren's syndrome (pSS) is a chronic, systemic, autoimmune disease that mainly affects the exocrine glands. From the clinical point of view, the most characteristic signs are dry mouth (xerostomia) and dry eyes (xerophthalmia). However, the clinical and serological spectra are wide and heterogeneous and—at onset or as it progresses—cytopenias, hypergammaglobulinemia or hypocomplementemia can develop, as can a number of extraglandular manifestations involving joints, lungs, kidneys, the nervous system, and the lymphatic system in the form of lymphoma. These extraglandular manifestations will mark the prognosis of the disease.1 The histological study of the glands reveals a lymphoplasmacytic infiltrate that leads to the destruction of acini and the ductal epithelial cells. Primary Sjögren's syndrome is considered a true autoimmune epithelitis,2 and is characterized by the production of certain autoantibodies, such as anti-Ro and anti-La, among others.
Primary Sjögren's syndrome can be found anywhere in the world. Over the years, the application of a variety of classification criteria has largely impeded the interpretation of the results of different studies. Its incidence in the general population differs according to sex, age and race. A recent meta-analysis, published in 2015,3 reported an estimated incidence of pSS of 6.92 per 100,000 population/year (95% confidence interval [CI], 4.98–8.86).
The same meta-analysis found a prevalence of pSS in the general population of 60.82 per 100,000 population (95% CI, 43.69–77.94); a subanalysis of that study estimated the prevalence of pSS, when classified exclusively on the basis of European/United States consensus criteria, at 73.57 cases per 100,000 population (95% CI, 37.51–109.63).
Primary Sjögren's syndrome is of growing interest in the scientific community and is estimated to be the second most widespread rheumatic disease. The lack of clear symptoms, especially in the early stages, and the clinical heterogeneity result in a considerable delay in the diagnosis. The disease occurs more frequently in women, with an estimated prevalence of 116.72 cases per 100,000 women (95% CI, 70.39–163.05) and 5.53 per 100,000 men (95% CI, 2.49–15.62), with a ratio of women to men of 10.72 (95% CI, 7.35–15.62).3 It occurs most frequently between the fourth and fifth decades of life, although it can develop at any age. In European cohorts, we find that 6% of the patients with pSS in the Italian population are diagnosed after the age of 65 years4 and that 15% of the pSS patients in the Spanish population are over 70 years of age when diagnosed.5 Primary Sjögren's syndrome is rare in children, with only 81 cases reported between 2000 and 2010; the age at diagnosis ranges between 4 and 16 years, with a mean age of 9.84 years and a ratio of girls to boys of 5:1.6
The GEMESS group reported their findings in a Spanish multicenter cohort in 2008.5 It involved 1010 patients who met the 1993 European criteria.7 This registry was established in 2005 and included incident and prevalent cases recorded between 1994 and 2007. Of the 1010 patients recruited, 707 also met the 2002 classification criteria of the American-European Consensus Group.8
The availability of a new homogeneous cohort of pSS patients in Spain will enable us to further our understanding of this complex and heterogeneous disease, update the epidemiological and clinical characteristics of pSS in our setting and improve the evaluation of certain outcome measures such as damage, comorbidity and the level of activity. It will also make it possible to compare subgroups of patients according to age, sex or serological profile, among other variables. There is lack of data on the diagnostic and therapeutic management of pSS in Spain, the percentage of patients with disease that is refractory to treatment, or the extent to which certain therapies are being employed. Thus, knowledge of these aspects would facilitate the standardized utilization of different tools for the diagnosis and evaluation of this disease, which would result in a greater uniformity of the clinical management of pSS in our population.
For this purpose, the Spanish Society of Rheumatology (SER [Sociedad Española de Reumatología]) has promoted its first registry of pSS patients (SJÖGREN'S-SER), an initiative of its working group on systemic autoimmune diseases (SAD-SER), with the methodological support and supervision of the SER research unit (RU-SER). SJÖGREN'S-SER is a descriptive, multicenter study of pSS patients who meet the consensus classification criteria of 2002.8 The 1-year cross-sectional phase, during which the patients were enrolled, has been completed. In this special article, we describe the objectives, design and methodology of SJÖGREN'S-SER, and some of the basic descriptive results as well as the strengths and weaknesses of the registry.
Patients and methodsSJÖGREN'S-SER is a Spanish retrospective multicenter registry of pSS patients who meet the American-European classification criteria of 20028 being treated in Spanish rheumatology outpatient clinics. The data were obtained from the review of medical records and from interviews between physicians and patients, and were collected using an electronic format.
ObjectivesThe primary objectives of SJÖGREN'S-SER are to describe the pSS patients included in the registry, providing data on:
- -
their clinical characteristics, with special reference to disease activity and severity,
- -
the biological characteristics,
- -
specific comorbidities and their incidence,
- -
disease management.
The secondary objectives of SJÖGREN'S-SER are:
- -
to establish a database including patients in the participating hospitals that could serve as a basis for future studies,
- -
establish a consortium of centers interested in pSS that could take part in collaborative projects on the disease.
The study included pSS patients who met the 2002 American-European classification criteria, were at least 18 years old and in full command of their faculties in terms of their ability to formulate responses and participate in the collection of the requested data, and were being treated in rheumatology departments, mainly of hospitals, but also of tertiary care centers that take part in the SAD-SER group. It did not include patients who, in the opinion of the investigator, could find it difficult to keep appointments or complete forms, or those who met any of the exclusion criteria specified in the 2002 consensus classification criteria (head and neck radiation therapy, hepatitis C virus or human immunodeficiency virus infection, pre-existing lymphoma, sarcoidosis, graft-versus-host disease or the use of anticholinergic drugs).8
The collaborating researchers were rheumatologists with extensive experience in the care and management of pSS patients. All the hospitals participating in the study created a database according to the model provided by the coordinators of the project, guaranteeing anonymity, in which they included all the pSS patients who were being seen in the department who met the inclusion criteria. For this, they used administrative databases or their own files. The list of patients from each center was sent to the RU-SER. To obtain a representative sample, without selection biases, the list of anonymous patients from each center was subjected to randomized sampling and the resulting randomized list was sent to each rheumatology department for successive recruitment. Each researcher contacted the randomly selected patients in consecutive order according to the randomization list provided, and proposed their participation in the study. Those patients who refused to participate were replaced by the next patient in the randomization list and underwent a brief structured interview during which a series of minimum basic data was collected.
Data collectionTo facilitate data collection, we developed an investigator's handbook and a quick guide to the questions to ask each patient on the day of his or her visit. The patients were asked to complete self-administered questionnaires on the day they were enrolled in the study. A software application was designed expressly for the registry and data storage. A user manual was prepared with instructions for the researchers. The software application has filters, ranges, menus and help dialogs to enhance data reliability. A member of the RU-SER was appointed as database administrator and monitor.
Different strategies were employed to ensure adequate data quality control. First, a pilot study was conducted to evaluate difficulties and problems involving the electronic data collection notebook (DCN) and the web-based platform. The results of this study made it possible to introduce the modifications required to ensure the comprehensibility of the DCN and greater simplicity in its use. Second, an investigator's handbook was prepared to describe and standardize the processes involved in the study and to solve possible doubts that could arise when introducing data in the DCN. This handbook also included information on controlling lost data during follow-up and the processes of verification and quality control of the data. Third, in situ monitoring was carried out by monitors accredited in the RU-SER from a percentage of randomly selected centers. The filters of the DCN prevented the inclusion of values that fell out of the range and of lost values.
VariablesThe primary objective of the registry is to obtain a characterization as accurate and complete as possible of the clinical signs, features of the disease course and patterns in the development of comorbidities in our pSS patients, as well as their management. Thus, we did not define a specific main outcome variable in this study, with the limitations that this implies. We included 298 variables, which are provided below.
For the description of the patients and to be able to analyze subgroups or modifiers and confounding factors, we included the following sociodemographic data: sex, race, level of education, date of birth, date of pSS symptom onset, date of diagnosis of pSS and date of inclusion in the registry. Using these dates, we calculated different age-related variables (age at the time of diagnosis, at enrollment in the cohort and at disease onset) and the duration of the disease.
Data were gathered on different aspects that make it possible to characterize the disease, including the presence of each of the 2002 classification criteria (oral and ocular symptoms and signs, histopathology and compatible antibodies), the presence of clinical manifestations of pSS (gland and genital involvement; ear, nose and throat involvement; fatigue; cachexia; splenomegaly; lymphadenopathy; joint, muscle and skin involvement; Raynaud's phenomenon; airway, pulmonary, renal, central and peripheral nervous system, hematological, gastrointestinal, cardiac and thyroid involvement); abnormal serological findings (erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, antinuclear antibodies, anti-Ro and anti-La antibodies, complement 3 and complement 4, immunoglobulins, cryoglobulins, β2-microglobulin, and anti-DNA, anti-Sm, anti-ribonucleoprotein and antiphospholipid antibodies); and hospital admissions and comorbidities (tobacco use, hypertension, diabetes mellitus, dyslipidemia, heart failure, ischemic heart disease, peripheral arterial disease, stroke, multiple sclerosis, celiac disease, fibromyalgia, osteoporosis, osteoporotic fracture, osteonecrosis and neoplasm).
We included drug and nondrug therapies used for the management of pSS and its complications, categorized on the basis of oral, cutaneous, nasal or vaginal involvement, Raynaud's phenomenon, systemic involvement and eye surgery.
The degree of involvement, activity and damage were measured using different validated indices. Some of these questionnaires are self-administered and were completed by the patients on the day they visited their rheumatologists, whereas others were calculated on the basis of the information gathered from the medical records and registered in the database developed specifically for this study. These indices were the Sjögren's Syndrome Disease Activity Index (SSDAI),9 the EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI) and the Sjögren's Syndrome Disease Damage Index (SSDDI).10
Statistical analysisGiven that there is no single main outcome variable, we assume that we want an accuracy of 1.5% to detect signs of pSS for an expected prevalence of around 2.5%. Accepting a type I error of 0.05 for an accuracy of 0.015 percent units, in a two-sided test for an estimated proportion of 0.025, we would need a population size of 417 individuals, which, moreover, is a realistic prediction of the total number of patients that could be included.
Descriptive statistics were used to describe the clinical and analytical characteristics of the patients. The normal distribution of the continuous variables was analyzed using the Kolmogorov–Smirnov test. The association between the variables was evaluated using parametric or nonparametric tests, depending on their distribution. Prevalence rates for 100 of the different signs, complications and comorbidities were estimated, together with their 95% CI. An analysis by center was performed to determine whether there were important differences, in which case, any estimate will be adjusted to the samples according to center.
Ethical aspectsThe present study complies with the Declaration of Helsinki and its subsequent revisions. All the participating patients have been duly informed and have completed and signed in duplicate the informed consent form. The participating centers assigned an identification number to each patient to maintain the confidentiality of the data in accordance with the current legislation (Royal Decree 1720/2007, a further development of Organic Law 15/1999, dated December 13, regarding the protection of personal data). The project was approved by the ethics committee of the hospital of the principal investigators and by the ethics committees of the participating hospitals.
ResultsThirty-three Spanish centers participated (Table 1). A total of 437 patients were included. The sociodemographic characteristics of the patients are shown in Table 2.
Participating centers.
| Hospital de Albacete |
| Hospital Carlos Haya |
| Hospital Clínico San Cecilio |
| Hospital de Basurto |
| Hospital de Bellvitge |
| Hospital de Donostia |
| Hospital de León |
| Hospital Marina Baixa |
| Hospital de Sierrallana |
| Hospital de Valme |
| Hospital Doce de Octubre |
| Hospital Dr. Negrín |
| Hospital General de Alicante |
| Hospital de L’Hospitalet |
| Hospital General Universitario Jerez de la Frontera 52 |
| Hospital Germán Trías y Pujol |
| Hospital Gregorio Marañón |
| Hospital Infanta Sofía |
| Hospital de la Princesa |
| Hospital Madrid Norte Sanchinarro |
| Hospital Marqués de Valdecilla |
| Hospital de Meixoeiro |
| Hospital Miguel Servet |
| Hospital Parc-Taulí |
| Hospital Puerta de Hierro |
| Hospital Ramón y Cajal |
| Hospital San Pau y Santa Creu 97 |
| Hospital Sant Joan Despí Moisès Broggi |
| Hospital Universitario de Canarias |
| Hospital Virgen de la Concha |
| Hospital Virgen de la Salud |
| Hospital Virgen de las Nieves |
| Hospital Príncipe de Asturias 127 |
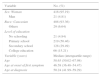
Sociodemographic characteristics.
| Variable | No. (%) |
|---|---|
| Sex: Woman | 416 (95.19) |
| Man | 21 (4.81) |
| Race: Caucasian | 408 (93.36) |
| Others | 29 (6.64) |
| Level of education | |
| No schooling | 21 (4.84) |
| Primary school | 219 (50.46) |
| Secondary school | 128 (29.49) |
| College education | 66 (15.21) |
| Variable (years) | Median (interquartile range) |
| Age | 58.63 (50.02–67.98) |
| Age at onset of first symptom | 46.58 (36.48–54.47) |
| Age at diagnosis | 50.24 (41.99–59.29) |
The 115 patients who declined the invitation to participate in the study had a mean age of 62.25±16.63 years. The majority were women and 3.48% were men. The minimum questionnaire completed by these 115 patients revealed no significant differences with respect to the group of participants.
The data concerning the prevalence in the registry cohort of the 6 criteria that comprise the American-European classification appear in Table 3. The table includes information on the numbers and percentages of patients who responded affirmatively to each of the 14 items encompassed in the 6 criteria, as well as the median of items recorded for these individuals, which was 5 (interquartile range: 4–5). Clinical criteria were those most often reported. The Schirmer I test was performed in 402 patients; it was indicative of disease in 85% (371 of 402). Unstimulated salivary flow rate was measured in 133 patients, representing 30% of the individuals in the cohort; the results were abnormal in 89%. Rose Bengal staining was used in 144 patients, 81% of whom had evidence of disease. Salivary gland scintigraphy was carried out in more than half the participants (253 of 437), with results indicative of disease in 87%. Minor salivary gland biopsy was carried out in 193 patients, 44% of the patients in the cohort; the histological criteria for disease were met in 69% of the cases in which this study was performed. In all, 93% of the patients tested positive for anti-Ro and 67% for anti-La at some point in the course of the disease (Table 3).
Percentage of patients who met the American-European classification criteria for Sjögren's syndrome.
| Classification criteria | No. of patients (%) |
|---|---|
| 1. Ocular symptoms: a positive response to at least one question | |
| Have you had daily, persistent, troublesome dry eyes for more than 3 months? | 413 (94.51) |
| Do you have a recurrent sensation of sand or gravel in the eyes? | 402 (91.99) |
| Do you use artificial tears more than 3 times a day? | 354 (81.01) |
| 2. Oral symptoms: a positive response to at least one question | |
| Have you had a daily feeling of dry mouth for more than 3 months? | 411 (94.05) |
| Do you have persistent or recurrent swollen salivary glands? | 154 (35.24) |
| Do you frequently drink liquids to aid in swallowing dry food? | 364 (83.30) |
| 3. Ocular signs: a positive result for at least one of the following tests: | |
| Schirmer I test, performed without anesthesia (≤5mm in 5 minutes) | 371 (84.90) |
| Rose Bengal score or other validated dry eye score (≥4 according to the van Bijsterveld score) | 117 (26.77) |
| 4. Salivary gland involvement: a positive result for at least one of the following tests: | |
| Unstimulated whole salivary flow (≤1.5mL in 15 minutes) | 119 (27.23) |
| Parotid sialography (diffuse sialectasia, without obstruction in a major duct) | 27 (6.18) |
| Salivary scintigraphy (delayed uptake, reduced concentration and/or delayed excretion of tracer | 221 (50.57) |
| 5. Histopathology: in minor salivary gland (focal lymphocytic sialoadenitis, evaluated by an expert histopathologist, with a focus score ≥1) | 133 (30.44) |
| 6. Antibodies: | |
| Positive test for anti-Ro/SSA and/or | 409 (93.59) |
| Positive test for anti-La/SSB | 293 (67.05) |
| No. of criteria met, median (interquartile range) | 5 (4–5) |
Classification criteria for primary Sjögren's syndrome: positive results for at least 4 of the 6 items, provided that either the histopathological or serological criterion (5 or 6) is met, or positive results for 3 of the 4 objective criteria (3, 4, 5 and 6).
Exclusion criteria: hepatitis C virus, human immunodeficiency virus, sarcoidosis, previous head and neck radiation therapy, pre-existing lymphoma, graft-versus-host disease, use of anticholinergic drugs.
A total of 119 patients (27%) met the new classification criteria issued in 2012 by the Sjögren's International Collaborative Clinical Alliance Cohort-American College of Rheumatology (SICCA-ACR).11Table 4 shows the prevalence of each item in this cohort. The criteria that were most frequently met (86.47% of the patients) were serological findings (anti-Ro or anti-La antibodies or RF+ and ANA ≥1/320). Staining with lissamine green and with fluorescein was carried out in 38 and 56 patients, respectively; thus, the total ocular staining score (OSS)12 was not determined in 416 patients, more than 94% of the cohort.
Percentage of patients who met the Sjögren's International Collaborative Clinical Alliance Cohort-American College of Rheumatology (SICCA-ACR) classification criteria for Sjögren's syndrome.
| Classification criteria | No. of patients (%) |
|---|---|
| 1. Ocular staining score (OSS) ≥3 | |
| OSS right eye (median, interquartile range) | 2 (2–3) |
| OSS left eye (median, interquartile range) | 3 (2–3) |
| Lissamine green | 19 (3.75) |
| Fluorescein | 81 (18.54) |
| 2. Histopathology: in minor salivary gland (focal lymphocytic sialoadenitis. evaluated by an expert histopathologist, with a focus score ≥1) | 133 (30.44) |
| 3. Serology: | |
| Positive test for anti-Ro/SSA or | 409 (93.59) |
| Positive test for anti-La/SSB or | 293 (67.05) |
| Antinuclear antibodies (ANA) ≥1/320 and | 272 (62.23) |
| Positive test for rheumatoid factor (RF) | 283 (64.76) |
| Patients who meet the SICCA classification criteria | 119 (27.23) |
SICCA classification criteria: positive results for at least 2 of the criteria described above.
Exclusion criteria: hepatitis C virus, human immunodeficiency virus, sarcoidosis, amyloidosis, previous head and neck radiation therapy, graft-versus-host disease, IgG4-related disease.
The Spanish SJÖGREN'S-SER registry was designed for the purpose of characterizing a representative cohort of patients with pSS in Spain, in the routine clinical practice setting, in order to analyze the magnitude and distribution of the clinical signs, the biological features, the activity and cumulative damage of the disease, the associated comorbidity and the therapeutic management with and without drug treatment in the Spanish population. This will enable us to build on and update our understanding of this disease and plan strategies to be implemented in the early diagnosis, follow-up and management of the patients. This would not only benefit these individuals, but would facilitate strategic health planning, which is the responsibility of both primary care specialists and rheumatologists.
The participating patients are presently being followed up in the participating departments, a circumstance that reflects real-world routine clinical practice in pSS in Spain. The purpose of this cross-sectional study is to address certain well-defined objectives. We established the mandatory collection of certain variables for the database, most of which have standardized definitions, as they are used in validated damage and activity indices. The SJÖGREN'S-SER will make it possible to analyze subgroups according to age, clinical characteristics or biological features, will provide information on cardiovascular risk in pSS patients in the Spanish population and will outline the therapeutic management of pSS patients in Spain. Thus, this registry is an important knowledge instrument that will enable the multicenter study of pSS, either with the data stored in a database or the collection of data on additional variables in new lines of research.
The SJÖGREN'S-SER recruited a total of 437 patients who meet American-European classification criteria and are being treated in Spanish rheumatology departments. The demographic profile of a patient included in this cohort is similar to that of other series: a Caucasian woman over 50 years of age.5 The delay between the onset of the first symptoms and diagnosis is considerable, the median age at the time of the first symptom being 47 years and the median age at diagnosis being 50 years. The great majority of the patients presented with oral and ocular sicca syndrome. The Schirmer test was the technique of choice for the evaluation of ocular dryness in most of the patients. Despite its being a simple and readily available technique, unstimulated salivary flow rate was measured much less frequently than salivary gland scintigraphy in the evaluation of dry mouth (30% and 50%, respectively). In all, 69% of the minor salivary gland biopsies met the histological classification criteria for pSS. The majority of the patients enrolled in this cohort are serologically positive. Classical rose Bengal staining was performed in only 1 third of the patients. Staining with lissamine green and fluorescein was carried out in 9% and 13% of the patients, respectively. For this reason, the results of the OSS were not determined in over 94% of the participants. This circumstance is probably related to the recent introduction of these stains as classification criteria in the new 2012 criteria, and this may explain the low percentage of patients who met the SICCA-ACR criteria.
One of the strengths of our study lies in the fact that all the centers with specialized care in rheumatology of the SAD-SER group were invited to participate. These centers are not expected to have a selection bias, since none of them receive pSS patients referred from other institutions. They simply are centers in which there is a higher probability that the professionals perform a complete follow-up of the patients because of their interest in autoimmune diseases. Although no secondary care centers were included, it can be expected that a sufficiently representative proportion of the patients with pSS in Spain has been attended to at some point at the tertiary care level, either because of complications or in regard to some specific problem.
The extensive representation of the different Spanish autonomous communities among the participating centers and the large number of centers collaborating in the project will enable us to better adjust our basic knowledge of pSS to the particular features of our patient population.
One limitation of our study is the retrospective collection of the clinical characteristics and analytical data of the patients at the time of their inclusion in the study. This could pose certain problems such as the absence of control of the quality of the information, measurement errors that can result in a bias in the magnitude of the associations, difficulties in establishing the moment at which a given event occurred or problems related to the collection of data for important confounding variables.
Another limitation of the study is that it will only be representative of pSS patients attended to in rheumatology departments. Thus, there could be an overrepresentation of bone and joint and systemic autoimmune manifestations, as well as an underrepresentation of severe ocular involvement, among other signs.
ConclusionsThe SJÖGREN'S-SER is a registry of pSS patients in Spain that is in the process of examining and analyzing a current, homogeneous, multicenter cohort. It has collected detailed and reliable information on the clinical signs, biological features, activity and damage of the disease, associated comorbidity and management with and without drug treatment.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThe Spanish Society of Rheumatology (SER).
Conflicts of interestThe authors declare they have no conflicts of interest.
We thank Milena Gobo and Loreto Carmona for their work, effort and methodological support, and all the staff of the SER that has participated in the project in some way or another.
Raúl Menor (Hospital General Jerez de la Frontera, Jerez de la Frontera). Beatriz Rodríguez (Hospital Universitario de Canarias, Santa Cruz de Tenerife). Ángel García Aparicio (Hospital Virgen de la Salud, Toledo). Francisco Javier López Longo (Hospital Gregorio Marañón, Madrid). Sara Manrique-Arija (Hospital Carlos Haya, Málaga). Jesús Alberto García Vadillo (Hospital de la Princesa, Madrid). Susana Gil Barato (Hospital General de Alicante, Alicante). Ruth López-González (Hospital Virgen de la Concha, Zamora). Francisco Javier Narváez (Hospital de Bellvitge, Barcelona). Carlos Galisteo (Hospital Parc-Taulí, Sabadell). Jorge González Martín (Hospital Madrid Norte Sanchinarro, Madrid). Esther Ruiz Lucea (Hospital de Basurto, Basurto). Antonio Naranjo, Celia Erausquin, Iñigo Rúa-Figueroa (Hospital Doctor Negrín, Las Palmas de Gran Canaria). Óscar Illera (Hospital Infanta Sofía, Madrid). Lurdes Romani (Hospital Virgen de las Nieves, Granada). Sheila Melchor (Hospital Doce de Octubre, Madrid). Begoña Moreira (Hospital de Sierrallana, Torrelavega). Enrique Raya (Hospital Clínico San Cecilio, Granada). Marina Rodríguez López, Coral Mouriño, José María Pego (Hospital de Meixoeiro, Vigo). Natalia Cid (Hospital de Valme, Sevilla). Enrique Júdez (Hospital de Albacete, Albacete). Clara Moriano (Hospital de León, León). Vicente Torrente (Hospital de L’Hospitalet, Hospitalet de Llobregat). Hèctor Corominas (Hospital Sant Joan Despí Moisès Broggi, Barcelona). Blanca García Magallón (Hospital Miguel Servet, Zaragoza). Carlos Guillén Astete (Hospital Ramón y Cajal, Madrid). Ivan Castellvi (Hospital San Pau y Santa Creu, Barcelona). Cristina Bohórquez (Hospital Príncipe de Asturias, Alcalá de Henares), Javier Loricera (Hospital Marqués de Valdecilla, Santander). Joaquín Belzunegui (Hospital de Donostia, Guipúzcoa).
A complete list of contributors is available on the Annex A.
Please cite this article as: Fernández Castro M, et al. SJÖGREN-SER: Registro nacional de pacientes con síndrome de Sjögren primario de la Sociedad Española de Reumatología: objetivos y metodología. Reumatol Clin. 2016;12:184–189.


