

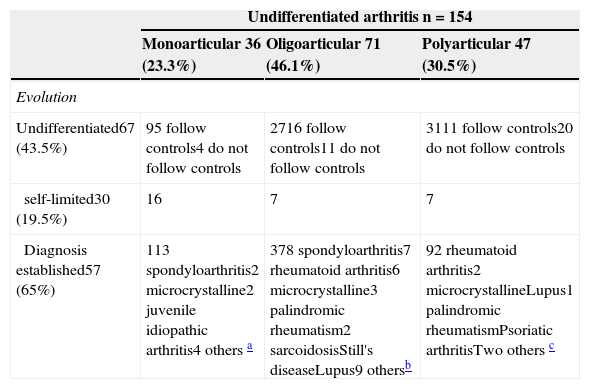
The use of a coding system in rheumatology improves the performance and quality of patient care 1. In the rheumatology department of our hospital, which has a reference area of 850 000 inhabitants, coding is carried out since 1984. Several rheumatologists prospectively collect, at 6 months of the first visit, filiation and diagnosis of patients seen in the clinic, patients admitted to hospital beds and admitted to other services that request an interconsultation. The nomenclature of the American College of Rheumatology (ACR) of 19832 was used and suitably modified to include a section of undiagnosed arthritis where mono, oligo and polyarthritis without an identified cause1 are included. Between 2006 and 2011 13,767 first consultations were carried out and 154 patients with undiagnosed arthritis (1.12%) were classified. They retrospectively reviewed the medical records of these patients and the location of arthritis, follow up and final diagnosis reached up until December 2013 were collected, with an elapsed minimum 2½ years since the first visit (range 2.5–5 years). The distribution of arthritis was: 36 (23.3%) monoarticular, 71 (46.1%) oligoarticular and 47 (30.5%) polyarticular. Monoarticular forms affected the following joints: in 21 cases (58.3%) knee; 4 (11.1%) metatarsophalangeal; 3 (8.3%) proximal interphalangeal; 2 (5.5%) tibioperoneoastragalus; 2 (5.5%) carpus; 2 (5.5%) metacarpophalangeal; 1 (2.7%) tarsus, and 1 (2.7%) elbow. The evolution of arthritis is summarized in Table 1.
| Undifferentiated arthritis n=154 | |||
|---|---|---|---|
| Monoarticular 36 (23.3%) | Oligoarticular 71 (46.1%) | Polyarticular 47 (30.5%) | |
| Evolution | |||
| Undifferentiated67 (43.5%) | 95 follow controls4 do not follow controls | 2716 follow controls11 do not follow controls | 3111 follow controls20 do not follow controls |
| self-limited30 (19.5%) | 16 | 7 | 7 |
| Diagnosis established57 (65%) | 113 spondyloarthritis2 microcrystalline2 juvenile idiopathic arthritis4 others a | 378 spondyloarthritis7 rheumatoid arthritis6 microcrystalline3 palindromic rheumatism2 sarcoidosisStill's diseaseLupus9 othersb | 92 rheumatoid arthritis2 microcrystallineLupus1 palindromic rheumatismPsoriatic arthritisTwo others c |
It is noteworthy that of the 36 patients with monoarthritis, 4 evolved to seronegative oligo or polyarthritis and 3 oligoarthritis patients progressed to undifferentiated polyarthritis, also undifferentiated.
We conclude that undifferentiated arthritis may progress to a classifiable inflammatory disease, self-limit or persist undifferentiated, representing a challenge for the rheumatologist.3–5 The percentage of spontaneous resolution in our series of cases is 44.4%, 9.8% and 14.9% for mono, oligo and polyarthritis, respectively. The former are more inclined to resolve spontaneously, whereas oligoarticular and polyarticular onset forms are more likely to become chronic. In the present series an established diagnosis was reached in 57 patients (65%) after an average of 8 months; mostly had an oligoarticular origin (65%). 11 patients (19%) were diagnosed with spondyloarthritis, whose onset was characterized as mono or oligoarticular; conversely, the 9 patients (16%) with a subsequent diagnosis of rheumatoid arthritis (RA) had an oligo or polyarticular onset. In addition, 10 patients (17.5%) were diagnosed with microcrystaline arthritis with a mono, oligo or polyarticular onset.
Most undiagnosed polyarthritis in the first 6 months, continued without cause after follow up. Interestingly, the percentage of patients who remain in follow-up is higher in classifiable than in undifferentiated arthritis (66.6 versus 32.9%).
Based on this, we can conclude that due to changes in the evolution of inflammatory joint diseases, rheumatology coding systems should be dynamic.1 In general, the ACR classification criteria for different rheumatic diseases have little discriminatory value in the initial stages of the disease, so must be modified so that they allow us to distinguish these forms of early arthritis.3,6 These criteria should be able to classify cases that will remain as undifferentiated arthritis, in which it has been shown that early treatment is paramount, even when not meeting established disease criteria.7,8 In practice, the new criteria for RA and spondyloarthritis already been developed in this light.9,10
Please cite this article as: Rodríguez-Muguruza S, Martínez-Morillo M, Riveros-Frutos A, Tena X. ¿Cuál es la evolución de las artritis indiferenciadas? Reumatol Clin. 2015;11:57–58.


