


Rheumatoid arthritis (RA) is a chronic inflammatory disease, characterized by polyarthritis and systemic manifestations. RA-fatigue is a significant problem and adds on disease burden. Sleep disturbance, depression, and disease activity are suggested contributing factors to RA-fatigue; however, their combined role did not examine before among Egyptian RA patients. The objective of the study was to investigate the presence of fatigue, sleep and mood disturbances in RA patients. Also, to evaluate the possible association of poor sleep, depression, and disease activity with RA-fatigue.
MethodsThis cross-sectional study included 115 RA patients diagnosed according to the 2010 ACR-EULAR criteria and 46 age and sex matched controls. Fatigue using the Multidimensional Assessment of Fatigue-Global Fatigue Index, sleep using the Pittsburgh Sleep Quality Index and mood status using Beck Depression Inventory were assessed for all participants. RA disease activity was evaluated using disease activity score-28 joints.
ResultsRA patients had higher mean fatigue, sleep disturbance, and depression scores (27.2±8.9, 6.4±3.6, and 12.8±7.3; respectively) than controls (22.7±7, 4.8±3, 7.8±5.9; respectively) (P<.05). Poor sleep, depression and higher disease activity were significantly correlated with fatigue (r=0.4, r=0.65, r=0.55; respectively) (P<.001). The three variables may explain up to 49.1% of the variation in fatigue on multiple regression analysis.
ConclusionFatigue, poor sleep, and depression are more common in Egyptian patients with RA. A remarkably higher fatigue was associated with poor sleep, depression, and high disease activity, thus monitoring these silent comorbidities in clinical practice is required.
La artritis reumatoide (AR) es una enfermedad inflamatoria crónica, caracterizada por poliartritis y manifestaciones sistémicas. La fatiga asociada a AR es un problema importante y aumenta la carga de la enfermedad. La alteración del sueño, la depresión y la actividad de la enfermedad son factores sugeridos que contribuyen a la fatiga asociada a AR; sin embargo, su papel no se ha examinado previamente en pacientes egipcios con AR. El objetivo del estudio fue investigar la presencia de fatiga y alteraciones del sueño y humor en pacientes con AR. Además, evaluar la posible asociación del sueño deficiente, depresión y la actividad de la enfermedad con la fatiga asociada a AR.
MétodosEste estudio transversal incluyó 115 pacientes con AR, diagnosticados según los criterios de la ACR-EULAR 2010 y 46 pacientes de control emparejados por edad y sexo. Se evaluó en todos los participantes la fatiga mediante el índice de evaluación multidimensional de la fatiga y la fatiga global, el sueño utilizando el índice de calidad del sueño de Pittsburgh y el estado de ánimo mediante el Inventario de Depresión de Beck. La actividad de la enfermedad de la AR se evaluó utilizando la medida de la actividad de enfermedad-28 articulaciones.
ResultadosLos pacientes con AR presentaron en promedio una mayor fatiga, alteración del sueño y puntuaciones de depresión (27,2±8,9; 6,4±3,6 y 12,8±7,3, respectivamente) que los pacientes de control (22,7±7; 4,8±3 y 7,8±5,9, respectivamente) (p<0,05). El sueño deficiente, la depresión y una mayor actividad de la enfermedad se correlacionaron significativamente con la fatiga (r=0,4; r=0,65; r=0,55, respectivamente) (p<0,001). Las 3 variables pueden explicar hasta el 49,1% de la variación en fatiga en el análisis de regresión múltiple.
ConclusiónLa fatiga, el sueño deficiente y la depresión son más comunes en pacientes egipcios con AR. Una notablemente alta fatiga se asoció con un sueño deficiente, depresión y alta actividad de la enfermedad, por lo que se requiere el control de estas comorbilidades silenciosas en la práctica clínica.
Rheumatoid arthritis (RA) is the most common chronic inflammatory disease that affects about 1% of the population. RA is characterized by symmetric polyarthritis and widespread systemic manifestations lead to joint damage and functional disability.1 Among those manifestations, fatigue is very frequent and present in more than 40% of patients with RA using different diagnostic tools.2,3 Fatigue in RA can be defined as a sustained feeling of generalized exhaustion that interferes with activities, which is different from normal tiredness.4 Fatigue has a meaningful contribution to the impaired quality of life and thus adding to disease burden,5 that can make management of RA more challenging. Even though, patients with RA indicated they are not properly supported in the management of RA-fatigue in the healthcare services.6 In routine daily practice, RA patients are evaluated for their disease activity and treatment response; however, silent comorbidities of the disease such as fatigue, anxiety, depression and poor sleep are usually not addressed and thus not controlled.
Although it is the most prevalent complaint in patients with RA, the cause of fatigue is still unknown. Fatigue appears to be multifactorial and associated with multiple determinants (inflammatory and non-inflammatory factors).2,7 Possible inflammatory causes could be RA disease-related components, including pain and disease activity.8–10 In addition, there are non-specific factors associated with fatigue such as sleep disturbances, depressed mood, and physical inactivity.2,7,9 The majority of studies handled the effect of these variables (disease activity, poor sleep, and mood disturbance) on fatigue separately. There are relatively few data on the impact of these factors together on fatigue in RA.9,11
Cultural and religious aspects are important components that play role in expression of fatigue.12 The country of residence has an important influence on the level of fatigue and fatigue levels known to be variable across countries. Thus the data about fatigue cannot be transferred between different countries.13 Fatigue levels and its effects can be modified by cultural differences.14 Therefore, fatigue in RA remains an “unmet need” and more illustration of the contributing factors especially in different RA populations is required. There are limited studies evaluating the contributors of fatigue among Egyptian RA patients.15 To our knowledge, the contributions of poor sleep quality, mood disturbance, and disease activity altogether on fatigue has not been systematically studied among Egyptian patients with RA. The objective of this study was to investigate the presence of fatigue, poor sleep quality and depression in patients compared to healthy controls. Also, to analyze the possible relationship between sleep, mood status, and disease-specific variables with fatigue in RA patients.
Materials and MethodsStudy Design and ParticipantsThis cross-sectional study was carried out at the Rheumatology Department, Assiut University Hospital, Assiut, Egypt. From March 2014 to September 2015, patients who met the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for RA16 and were able to understand and respond to the questionnaires were recruited to this study. Patients who had a history of malignancies, major cognitive deficits, overlapping connective tissue diseases or currently receiving antipsychotic treatment were excluded from the study. As a reference group, age- and sex-matched apparently healthy volunteer subjects were randomly selected and enrolled in the study as the control group. All subjects provided informed consent to participate in this study and the study was approved by the local ethics committee.
Sociodemographic, Clinical and Laboratory AssessmentsAll subjects included in the study underwent sociodemographic data collection. For RA patients, disease-specific variables such as disease duration, morning stiffness (MS), current medications were evaluated. RA disease activity was measured by rheumatologists using the 28-joint disease activity score (DAS28) including swollen joint count (SJC), tender joint count (TJC), the patients’ global assessment (PGA) score and erythrocyte sedimentation rate (ESR) (mm/h). Remission was defined by DAS28-ESR<2.6, patients with DAS28-ESR ≥2.6 and <3.2 was considered to have mild or low disease activity, patients with ≥3.2 to less than or equal to 5.1 were considered moderate, and high activity was defined by DAS28-ESR more than 5.1.
Questionnaires AssessmentAll participants were interviewed personally to answer the study questionnaires delivered to them by the trained investigator (AR) who was blind to the patients’ clinical status.
Fatigue AssessmentFatigue was measured by the Multidimensional Assessment of Fatigue-Global Fatigue Index (MAF-GFI) questionnaire, which has been validated previously in RA,5 and in Arabic RA population after its translation.10 MAF-GFI is a self-reported questionnaire evaluates four dimensions of fatigue; degree and severity (MAF1), distress (MAF2), interference on activities of daily living (MAF3) and timing of fatigue (MAF4). MAF-GFI total score is calculated, with higher scores represented more severe fatigue.
Sleep Quality AssessmentAll subjects completed the Pittsburgh Sleep Quality Index (PSQI) questionnaire that evaluates sleep quality during the last month. PSQI has been used as an assessment tool to evaluate sleep quality in RA and it was previously translated and validated in Arabic RA patients.17 PSQI measures 7 components including subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication and daytime dysfunction. The PSQI total score is calculated by summing the 7 component scores, with poor sleep quality was defined when the PSQI total score was more than 5.
Depression AssessmentThe Beck Depression Inventory (BDI) was used for assessment of the depression in RA patients. Arabic version of BDI was validated and used to predict depression in RA.18 The BDI consists of 21 questions, and the total score of 0–13 is considered minimal (normal up and down), 14–19 is mild, 20–28 is moderate and 29–63 is severe depression.
Statistical AnalysisData were tested for normality by Shapiro–Wilk test and were normally distributed. Data are presented by means and standard deviation (SD) for continuous variables and by frequencies and percentages for categorical variables. Differences between groups were examined by independent samples t-test or chi square when appropriate. Correlations were performed with Pearson correlation coefficient. Multiple linear regression analyses that included significant variables associated with fatigue (dependent variable) in bivariate analyses were computed and expressed with beta coefficient (β) and 95% confidence interval (CI). A P value of ≤.05 was considered as statistically significant in all analyses. Data were analyzed using the Statistical Package for Social Science version 16 (SPSS Inc.; Chicago, IL, USA).
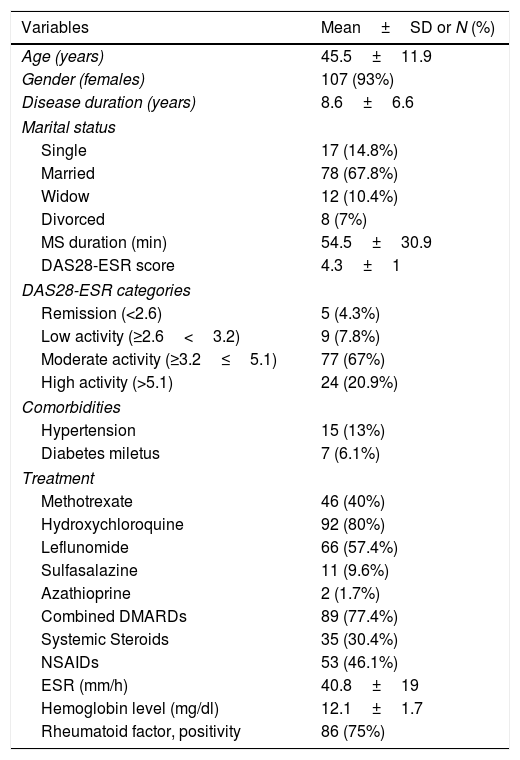
ResultsRA Patients’ CharacteristicsA total of 115 patients with RA, 93% females, with mean age was 45.5±11.9 years and mean disease duration was 8.6±6.6 years participated in the study. Participants’ characteristics are illustrated in Table 1.
Demographic and Clinical Characteristics of RA Patients.
| Variables | Mean±SD or N (%) |
|---|---|
| Age (years) | 45.5±11.9 |
| Gender (females) | 107 (93%) |
| Disease duration (years) | 8.6±6.6 |
| Marital status | |
| Single | 17 (14.8%) |
| Married | 78 (67.8%) |
| Widow | 12 (10.4%) |
| Divorced | 8 (7%) |
| MS duration (min) | 54.5±30.9 |
| DAS28-ESR score | 4.3±1 |
| DAS28-ESR categories | |
| Remission (<2.6) | 5 (4.3%) |
| Low activity (≥2.6<3.2) | 9 (7.8%) |
| Moderate activity (≥3.2≤5.1) | 77 (67%) |
| High activity (>5.1) | 24 (20.9%) |
| Comorbidities | |
| Hypertension | 15 (13%) |
| Diabetes miletus | 7 (6.1%) |
| Treatment | |
| Methotrexate | 46 (40%) |
| Hydroxychloroquine | 92 (80%) |
| Leflunomide | 66 (57.4%) |
| Sulfasalazine | 11 (9.6%) |
| Azathioprine | 2 (1.7%) |
| Combined DMARDs | 89 (77.4%) |
| Systemic Steroids | 35 (30.4%) |
| NSAIDs | 53 (46.1%) |
| ESR (mm/h) | 40.8±19 |
| Hemoglobin level (mg/dl) | 12.1±1.7 |
| Rheumatoid factor, positivity | 86 (75%) |
Abbreviations: morning stiffness (MS), DAS28-ESR: disease activity score, ESR: erythrocyte sedimentation rate, DMARDs: disease modifying anti-rheumatic drugs, NSAIDs: nonsteroidal anti-inflammatory drugs.
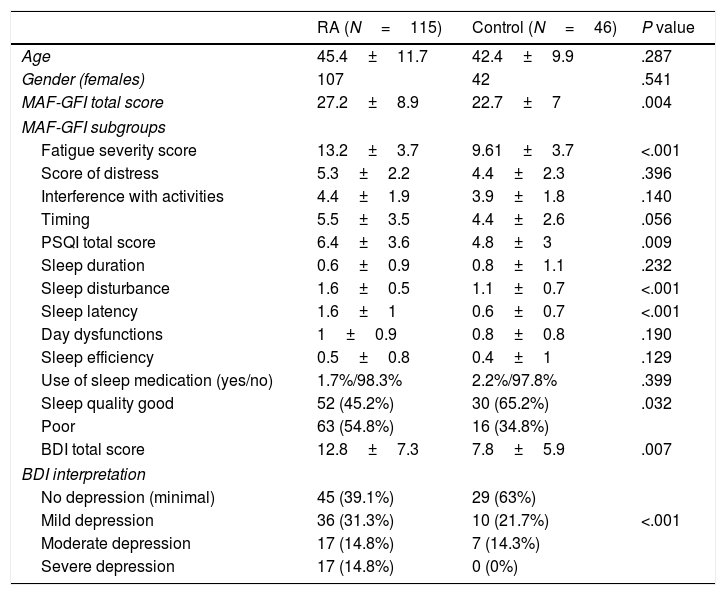
All RA and 46 matched subjects were able to complete the study questionnaires. There was no significant age or sex difference between them, Table 2. Overall, RA patients have significantly higher mean scores of fatigue severity, total MAF-GFI score, PSQI score, and BDI score compared to control subjects, (P<.001). 54.8% of RA are poor sleeper compared to 34.8% in the controls (P<.032), and average of 29.6% of RA patients have moderate to severe depression versus 14.3% within the controls (P<.001).
Characteristics of Studied Variables in Rheumatoid Arthritis Patients and Controls.
| RA (N=115) | Control (N=46) | P value | |
|---|---|---|---|
| Age | 45.4±11.7 | 42.4±9.9 | .287 |
| Gender (females) | 107 | 42 | .541 |
| MAF-GFI total score | 27.2±8.9 | 22.7±7 | .004 |
| MAF-GFI subgroups | |||
| Fatigue severity score | 13.2±3.7 | 9.61±3.7 | <.001 |
| Score of distress | 5.3±2.2 | 4.4±2.3 | .396 |
| Interference with activities | 4.4±1.9 | 3.9±1.8 | .140 |
| Timing | 5.5±3.5 | 4.4±2.6 | .056 |
| PSQI total score | 6.4±3.6 | 4.8±3 | .009 |
| Sleep duration | 0.6±0.9 | 0.8±1.1 | .232 |
| Sleep disturbance | 1.6±0.5 | 1.1±0.7 | <.001 |
| Sleep latency | 1.6±1 | 0.6±0.7 | <.001 |
| Day dysfunctions | 1±0.9 | 0.8±0.8 | .190 |
| Sleep efficiency | 0.5±0.8 | 0.4±1 | .129 |
| Use of sleep medication (yes/no) | 1.7%/98.3% | 2.2%/97.8% | .399 |
| Sleep quality good | 52 (45.2%) | 30 (65.2%) | .032 |
| Poor | 63 (54.8%) | 16 (34.8%) | |
| BDI total score | 12.8±7.3 | 7.8±5.9 | .007 |
| BDI interpretation | |||
| No depression (minimal) | 45 (39.1%) | 29 (63%) | |
| Mild depression | 36 (31.3%) | 10 (21.7%) | <.001 |
| Moderate depression | 17 (14.8%) | 7 (14.3%) | |
| Severe depression | 17 (14.8%) | 0 (0%) | |
Abbreviations: MAF-GFI: multidimensional assessment of fatigue-global fatigue index, PSQI: Pittsburgh Sleep Quality Index and BDI: Becks depression inventory.
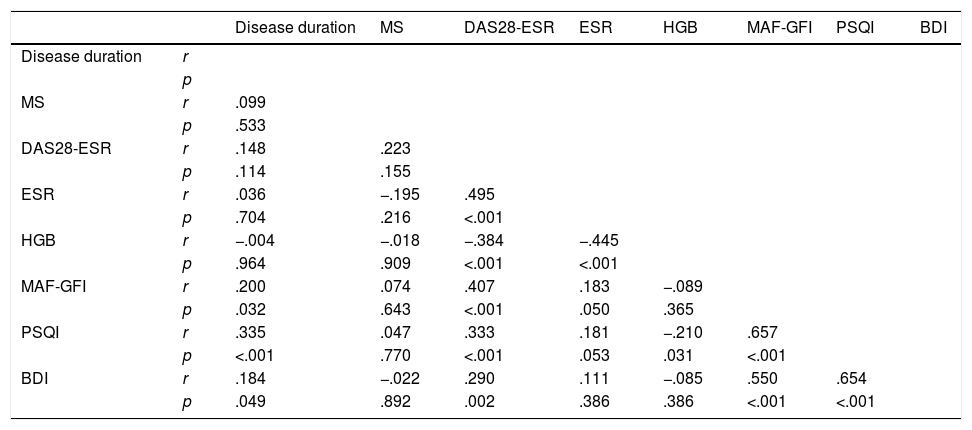
The mean fatigue score has moderate positive correlation with disease activity (r=0.407; P<.001), while mild correlations with disease duration (r=0.200; P=.032) and ESR (r=0.183; P=.050). Also, total MAF-GFI score is strongly correlated with poor sleep quality (r=0.657; p <.001) and with higher depression (r=0.550; P <.001), Table 3. No significant differences in fatigue score are found between those using different drug treatments and those not, Fig. 1.
Correlation Between Clinical and Laboratory RA Variables With Fatigue, Sleep Quality and Mood Scores.
| Disease duration | MS | DAS28-ESR | ESR | HGB | MAF-GFI | PSQI | BDI | ||
|---|---|---|---|---|---|---|---|---|---|
| Disease duration | r | ||||||||
| p | |||||||||
| MS | r | .099 | |||||||
| p | .533 | ||||||||
| DAS28-ESR | r | .148 | .223 | ||||||
| p | .114 | .155 | |||||||
| ESR | r | .036 | −.195 | .495 | |||||
| p | .704 | .216 | <.001 | ||||||
| HGB | r | −.004 | −.018 | −.384 | −.445 | ||||
| p | .964 | .909 | <.001 | <.001 | |||||
| MAF-GFI | r | .200 | .074 | .407 | .183 | −.089 | |||
| p | .032 | .643 | <.001 | .050 | .365 | ||||
| PSQI | r | .335 | .047 | .333 | .181 | −.210 | .657 | ||
| p | <.001 | .770 | <.001 | .053 | .031 | <.001 | |||
| BDI | r | .184 | −.022 | .290 | .111 | −.085 | .550 | .654 | |
| p | .049 | .892 | .002 | .386 | .386 | <.001 | <.001 |
Abbreviations: MAF-GFI: multidimensional assessment of fatigue-global fatigue index, PSQI: Pittsburgh Sleep Quality Index and BDI: Becks depression inventory.
 between RA patients who use specific drug therapy and who do not show no significant difference in fatigue score were found.")
Differences in MAF-GFI between RA patients who use and those not use specific drug therapy. Abbreviations: MAF-GFI: multidimensional assessment of fatigue-global fatigue index; MTX: methotrexate; HCQ: hydroxychloroquine; LFN: leflunomide; SZS: sulfasalazine; AZA: azathioprine; NSAIDs: nonsteroidal anti-inflammatory drugs. Legend: The differences in multidimensional assessment of fatigue-global fatigue index (MAF-GFI) between RA patients who use specific drug therapy and who do not show no significant difference in fatigue score were found.
The mean fatigue, sleep quality and depression scores are higher among RA patients with hypertension compared to those without, however it did not reach statistical significant (P > .05) for all. RA patients with concomitant diabetes have significantly higher frequencies of fatigue and poor sleep (P=.025 and P=.013; respectively), while depression level did not reach significance (P=.074) between patient groups.
Determinants of Fatigue Among RA PatientsThe statistically significant correlated variables with MAF scores from Table 3 were included in the multiple regression analysis. Sleep quality was the strongest determining parameters of fatigue (β=0.478; 95%CI=0.733–1.591; P<.001) followed by DAS28-ESR (β=0.215; 95%CI=0.620–2.941; P=.003) and depression (β=0.173; 95%CI=0.002–0.418; P=.048). The three variables could explain 49.1% of the variation in fatigue scores.
DiscussionFatigue is reported to be the most disabling factor by RA patients, with a negative impact on disease outcome and quality of life, therefore examining the factors associated with the levels of fatigue is important in clinical practice. The present study showed that fatigue levels, sleep and mood disturbances are higher in Egyptian patients with RA than healthy subjects. Also, poor sleep, severe depression as long as higher disease activity were significant determinants of fatigue in the RA patients. The current reported mean fatigue score among RA patients was comparable to that observed previously using the same fatigue tool measurement.19,20 There was a wide range of prevalence of RA-fatigue has been reported in the literature, with the difference in assessment tools and the ethnicity of RA populations.3,21 Higher fatigue rate has been found in other rheumatic diseases,22 with depression and sleep disturbances have been reported to influence fatigue. Fibromyalgia, which is known with high fatigue level, poor sleep quality and depression among other factors were common.23
While RA fatigue has been viewed as the byproduct of inflammatory process, others have shown that psychosocial factors may play a role. The inflammatory perspective of depression and fatigue in RA has been investigated. Different inflammatory cytokines, such as tumor necrosis factor (TNF)-α, interleukin (IL)-1 and IL-6 are important proinflammatory cytokines implicated in chronic fatigue and all of these are contributors in the inflammatory state in RA. Furthermore, social, family, work and daily living activities are multiple aspects may have an impact on fatigue.
The relationship between fatigue and examined determinants in RA are variable,2 most likely because of the multifactorial etiology of fatigue (physiological, psychological, as well as the disease aspects). Disease duration was found to be correlated with fatigue. However, Stebbings et al. showed that longer disease duration was associated with severe fatigue,20 a recent systematic review found that RA patients experience greater fatigue in irrespective of disease duration.8 The advanced age was not associated with greater fatigue in RA patients which is corresponding to prior study.20 Association between fatigue and disease activity in RA is controversial. A significant correlation between fatigue and ESR was noted in the RA patients as in other.8 DAS28-ESR has several components and this makes it better than measuring inflammation only. In this study, there was correlation between fatigue and overall DAS28-ESR in accordance with previous studies.10,15,24 In contrary, fatigue was not correlated with the ESR value and disease activity.3,20 Fatigue was reported among RA patients in remission or a low disease activity.25 This difference may be related to differences in the characteristics of the patient cohorts. Moreover, in a large longitudinal study despite decreased inflammation with RA treatment, fatigue severity remained unchanged.24 Specifically tailored interventions to reduce fatigue should be offered to RA patients.
According to our results, RA therapy that is based on the administration of disease-modifying anti-rheumatic drugs (DMARDs), immunosuppressant drugs, has no impact on fatigue level in consistent with Abdel-Magied et al.15 However previous work showed some evidence that TNF-inhibitors and to lesser extent DMARDs can reduce fatigue,3 there are relatively few data on whether conventional DMARDs only improve fatigue. Those authors present a different view when it comes to the importance of the type of therapy in the severity of fatigue. They claim that methods of treatment have an impact on decreased fatigue perception among RA patients. Furthermore, longitudinal studies focusing on the effectiveness of DMARDs and new therapies on fatigue seem to be necessary.
A high percentage RA patients have low quality of sleep, in accordance with the authors,21,26 with more than half of RA patients were poor sleepers. In our study, overall PSQI score (6.4±3.6) was similar to Elazeem et al. findings in Egyptian RA patients using PSQI (6.9±2.8).26 Sleep disturbance was strongly associated with fatigue in RA patients.11,27 While fatigue may disturb sleep quality, the disturbance in the sleep may also lead to greater fatigue and thus vicious cycle. The significant association between total PSQI score and DAS28-ESR score is observed in this study which emphasizes that painful joints and inflammation precipitate poor sleep and decreased alertness.7,20,28 In agreement with other authors,26 we found no significant association between PSQI and the use of DMARDs or NSAIDs (data not shown). From another prospect, depression represents a component of the vicious cycle of RA constitutional symptoms and can impede the remission of the disease.24 The medical literature suggests heterogeneous prevalence rates of depression in RA.21 Depression score recorded in RA study population is comparable to the literature.27 Presence of severe fatigue, high disease activity as well as poor sleep in RA patients could explain the higher number of RA cases with depression. Depression has been found to be associated with the fatigue within the RA cohort in previous studies.3,20
There are limited integrative data aiming at characterizing RA-related fatigue from a whole viewpoint. Fatigue, poor sleep, depression and disease activity can be the cause and the outcome in this viscous cycle. These findings support the results reported in different RA ethnic population.11,22,26 In a recent review by Katz,7 an empirical model of the causes of RA fatigue showed that these variables had direct and indirect effects on fatigue and explained the majority of variation in fatigue.
The major strengths of this study are the multiple multidimensional measurements used in the assessment of the variables, which all had been validated in RA. However, being cross-sectional design, the causality of the relationships cannot be determined. Some of the measure used may be affected by each other. Further research is needed to investigate whether improvements in sleep, depression and disease activity can reduce fatigue. Some other variables such as levels of pain did not included; which have been shown to have strong associations with fatigue.29 Stebbing et al. found that fatigue in RA patients had no significant association with pain but was associated with depression and anxiety.20 Despite these limitations, though, our findings were consistent with other research. Most of the studies about fatigue in patients with RA have been done in western countries and very few from developing countries. If we consider cultural differences, research from developing countries would be helpful to reveal ethnic differences. Future research in this field should aim at finding instruments covering all related dimensions of fatigue in patients with RA. Furthermore, the future investigations able to understand the underlying pathophysiological mechanisms of fatigue are needed.
ConclusionIn conclusion, severe fatigue, poor sleep and depression are more common in Egyptian patients with RA. The results of this study would suggest that fatigue may not solely result of RA disease activity, but may be the result of a constellation of multiple factors that include depression, and poor sleep. That is to say, evaluation of the fatigue and its determinants in RA assessment must be included in clinical practice. These results will be better to validate and replicate in RA patients from different ethnic origin.
FundingThe study was not funded by grant.
Conflict of InterestNone.
None.


