

To survey the efficacy of a practical workshop on clinical musculoskeletal anatomy held in five American countries.
MethodsA self-assessment competence questionnaire sent to participants 1–3 months after the workshop. Results were compared to the results of a practical, instructor-assessed, pre-workshop test.
ResultsThe response rate of participants was 76.4%. The overall, self-assessed competence score for anatomical items that had been included in the pre-test was 76.9 (scale 0–100) as compared to an overall score of 48.1 in the practical, pre-workshop test (p<0.001). For items that were addressed in the workshop, but not included in the pre-test, self-assessed competence was rated at 62.9. Differences in anatomical knowledge between individuals from different countries and professional groups noted in the practical pre-test were no longer present in the post-test self-assessment.
ConclusionsFrom this preliminary data and supporting evidence from the literature we believe that our anatomy workshop provides an effective didactic tool for increasing competence in musculoskeletal anatomy.
Estudiar la eficacia de un taller práctico de anatomía musculoesquelética realizado en 5 países de América.
MétodosUn cuestionario de autoevaluación de competencias se envió por correo electrónico a los participantes en un taller práctico de anatomía clínica musculoesquelética 1–3 meses después de concluido el taller. Los resultados de este cuestionario se compararon con los resultados de un examen práctico tomado por un instructor, previo al taller práctico.
ResultadosLa tasa de respuesta de los participantes fue del 76,4%. La puntuación de la competencia autoevaluada global de los temas anatómicos incluidos en el examen práctico previo fue 76,9 (escala de 0 a 100) en comparación con una puntuación total de 48,1 obtenida en la evaluación práctica previa al taller (p<0,001). Para los temas que se abordaron en el taller, pero no incluidos en la competencia previa a la autoevaluación, la calificación fue de 62,9. Las diferencias en el conocimiento anatómico entre personas de diferentes países y grupos de profesionales que se observaron en el examen práctico previo ya no se vieron en el cuestionario de autoevaluación.
ConclusionesA partir de estos datos preliminares y apoyados en la literatura creemos que nuestro taller de anatomía clínica práctica proporciona una herramienta didáctica eficaz para aumentar la competencia en anatomía musculo-esquelética.
Knowledge of musculoskeletal anatomy is suboptimal at many levels of rheumatology training and practice.1,2 In a recent practical anatomy test administered to rheumatology fellows, practicing rheumatologists and non-rheumatologist health care practitioners prior to a clinical anatomy workshop held in seven American countries, the overall mean percent of correct answers was 46.6% (SD 19.9). The test consisted in the identification or demonstration of 20 anatomical items thought to be relevant to rheumatologic practice.3 We now report the results of a self-assessed competence questionnaire completed 1–3 months after our workshop took place in five of the seven participating American countries, and compare these results to those of the pre-workshop assessment. The objective of the current study was to determine, using a self-assessment instrument, the efficacy of our clinical anatomy workshop in the five of the studied American countries. By previous agreement with the academic centers and rheumatology societies or associations, all data would be submitted or presented blinded.
MethodsThe methodology of our workshop which is based on the use of clinical vignettes and participant cross-examination to supplement classic anatomic teaching through drawings has been described in detail.4–10 Briefly, the seminar is based on the presentation of clinical vignettes with common clinical problems for each of the reviewed anatomic regions. Each one of the vignettes is followed by a didactic description of the pertinent anatomical structures involved. After a group of related vignettes, the practical part of the seminar follows, which is the identification of each of the discussed anatomical structures, by cross examination, in the participants and instructors bodies. For the current study, 25 questions were selected for use in the post-workshop competence assessment from an initial pool of 40 questions. This was achieved via a three-round Delphi exercise in which five of the authors participated (MAS, JEN-Z, JJC, PV-O, CH-D). To include a question, at each round an 80% agreement between participants was required. Of the selected questions, 17 had been asked in the pre-workshop practical anatomy test and eight referred to items that were not asked in the practical pre-test but were specifically reviewed in the workshop. In the current self-assessment survey, a five-point Likert scale ranging from not competent (score=0) to highly competent (score=4) at identifying the structure or function of each anatomical item queried was used. Two countries were not included in this survey due to anticipated communication barriers. Thus, a total of 140 participants from five countries were asked to participate. The initial request was sent via email one month after the workshop and monthly thereafter to a maximum of three requests.
The self-assessment competence scores were obtained as follows: (added Likert self-rated scores/maximum possible punctuation)×100. Competence scores of fellows, rheumatologists and non-rheumatologist health care practitioners, as well as between countries, were compared by ANOVA. Efficacy of the workshop was determined by comparing the pre-workshop scores (as assessed by instructors) and the post-workshop scores (self-assessed) by the t test for paired samples.
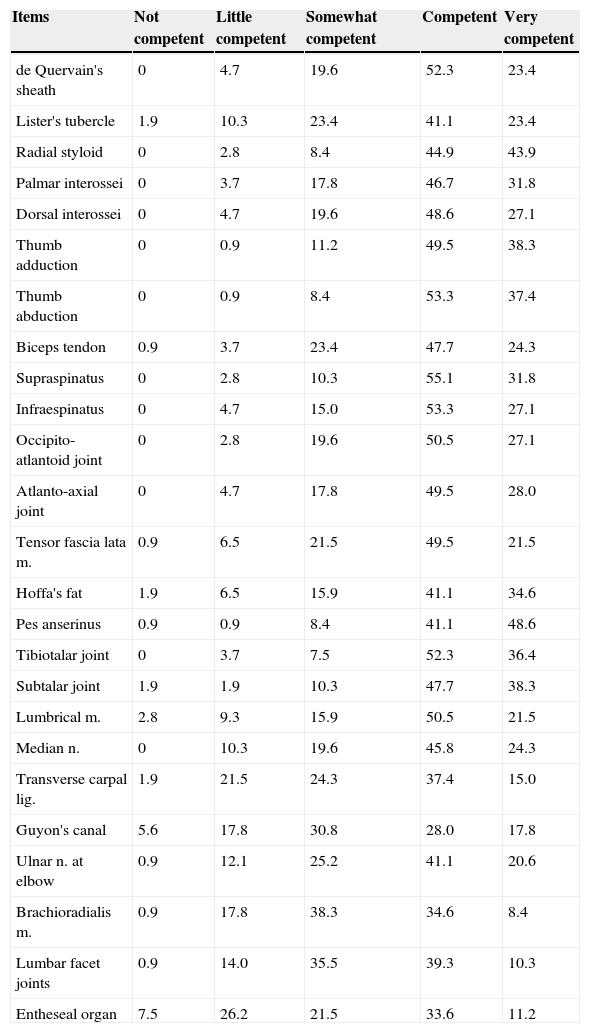
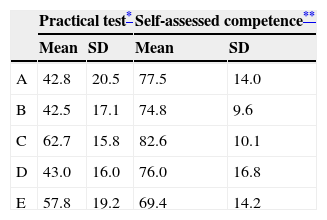
ResultsThe overall response rate was 76.4% (107/140 respondents, inter-country range 56–100%). Of the total participants, 54.2% were female, and 45.8% male; 55.1% were residents, 33.4% were practicing rheumatologists, and 8.4% non-rheumatologists. The average professional experience was 6.2±8.6 years (range 1–46). A significantly higher overall self-assessment competence score (Table 1, items 1–17) was noted as compared to the pre-workshop practical examination score (76.9±16.3 vs 48.1±19.6; p<0.0001). The self-assessment competence score for the items not included in the pre-workshop practical test but discussed in the seminar (Table 1, items 18–25) was 62.9±16.5, which differed statistically from the score for the 17 items that had been included in the pre-workshop assessment of 76.9±16.3; p<0.001 (Table 1). Interestingly, the marked differences noted between countries in the pre-workshop tests (inter-country range 42.5±17.1 to 67.2±15.8) were no longer present in the post-workshop self-assessments (inter-country range 69.4±14.2 to 82.6±10.1, Table 2). Likewise, whereas in the preworkshop assessment rheumatology fellows scored significantly higher than non-rheumatologist health care practitioners, with the rheumatologists in practice placing in between, these differences were no longer present in the post workshop self-assessment. All three groups showed significant improvement in the post workshop self-assessment (results not shown).
Self-assessed anatomical competency: 25 anatomical items inquired.a
| Items | Not competent | Little competent | Somewhat competent | Competent | Very competent |
|---|---|---|---|---|---|
| de Quervain's sheath | 0 | 4.7 | 19.6 | 52.3 | 23.4 |
| Lister's tubercle | 1.9 | 10.3 | 23.4 | 41.1 | 23.4 |
| Radial styloid | 0 | 2.8 | 8.4 | 44.9 | 43.9 |
| Palmar interossei | 0 | 3.7 | 17.8 | 46.7 | 31.8 |
| Dorsal interossei | 0 | 4.7 | 19.6 | 48.6 | 27.1 |
| Thumb adduction | 0 | 0.9 | 11.2 | 49.5 | 38.3 |
| Thumb abduction | 0 | 0.9 | 8.4 | 53.3 | 37.4 |
| Biceps tendon | 0.9 | 3.7 | 23.4 | 47.7 | 24.3 |
| Supraspinatus | 0 | 2.8 | 10.3 | 55.1 | 31.8 |
| Infraespinatus | 0 | 4.7 | 15.0 | 53.3 | 27.1 |
| Occipito-atlantoid joint | 0 | 2.8 | 19.6 | 50.5 | 27.1 |
| Atlanto-axial joint | 0 | 4.7 | 17.8 | 49.5 | 28.0 |
| Tensor fascia lata m. | 0.9 | 6.5 | 21.5 | 49.5 | 21.5 |
| Hoffa's fat | 1.9 | 6.5 | 15.9 | 41.1 | 34.6 |
| Pes anserinus | 0.9 | 0.9 | 8.4 | 41.1 | 48.6 |
| Tibiotalar joint | 0 | 3.7 | 7.5 | 52.3 | 36.4 |
| Subtalar joint | 1.9 | 1.9 | 10.3 | 47.7 | 38.3 |
| Lumbrical m. | 2.8 | 9.3 | 15.9 | 50.5 | 21.5 |
| Median n. | 0 | 10.3 | 19.6 | 45.8 | 24.3 |
| Transverse carpal lig. | 1.9 | 21.5 | 24.3 | 37.4 | 15.0 |
| Guyon's canal | 5.6 | 17.8 | 30.8 | 28.0 | 17.8 |
| Ulnar n. at elbow | 0.9 | 12.1 | 25.2 | 41.1 | 20.6 |
| Brachioradialis m. | 0.9 | 17.8 | 38.3 | 34.6 | 8.4 |
| Lumbar facet joints | 0.9 | 14.0 | 35.5 | 39.3 | 10.3 |
| Entheseal organ | 7.5 | 26.2 | 21.5 | 33.6 | 11.2 |
We found that our workshop on clinical anatomy using clinical vignettes and participant cross-examination to supplement classic anatomic teaching through drawings is effective across a wide array of pre-workshop levels of anatomic knowledge and experience. Post workshop self-assessment scores indicate a meaningful enhancement in knowledge and confidence in skills in clinical anatomy in participants of varying pre-workshop competence. This study did not include direct observation of participants’ clinical anatomy skills through a post workshop practical assessment. Nonetheless we feel the importance of self-perceived confidence in a practitioner's ability in clinical anatomy as well as the degree of interest and pleasure we have observed in participants (qualitative data not shown) is likely to stimulate further interest in learning and teaching in this important area. This will address both the key gap that exists in clinical anatomy skills and greatly benefit patients. Interestingly, the scores were significantly higher for questions referring to items that had been included in the practical pre-test, than those that referred to items not included in the pre-test but specifically addressed in the workshop. While it is possible that these questions were inherently more difficult, it is also possible that the pre-test primed the participants for a greater recollection. An important limitation to our study is that scores from two dissimilar assessment methods, a practical clinical musculoskeletal anatomy pre-test and a self-rated competency assessment, were compared. However, two pieces of information lend support to the validity of our findings. The first is that in Country B, appropriate conditions allowed us to take a practical post-workshop anatomy test. In this country, the pre-workshop score (modified for 17 items) was 40.1 and the post-workshop score was 78.2, which approximates to the findings of the current survey.3 The second is a European self-reported competence survey taken in rheumatology fellows and young rheumatologists in which competence in anatomy was rated at 52.3% which lies close to the 46.6±19.9% found in our pre-workshop practical anatomy test.11 These two pieces of information suggest that self-assessment may be a valid method to study competency in musculoskeletal clinical anatomy. Based on these limited data we are optimistic that our clinical anatomy workshop may positively impact knowledge and skills in this important area for practicing rheumatologists and that further assessment of its utility is warranted.
Conflict of interestThe authors declare no conflict of interest.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.


