

Social media (SoMe) has reshaped access to health information, which may benefit patients with rheumatoid arthritis (RA), although an evaluation of the characteristics of contents for Spanish-speaking patients is lacking. We aimed to assess patient engagement, reliability, comprehensiveness, and quality of data uploaded to YouTube® for Spanish-speaking patients.
MethodsWe evaluated the videos uploaded to YouTube® in Spanish about RA. Information about video length, engagement (i.e., views, likes, popularity index), time online, and the source was retrieved; we appraised reliability (DISCERN), comprehensiveness (content score), and quality (Global Quality Score) using standardized scores.
ResultsWe included 200 videos in the study and classified 67% of the videos as useful. These videos had a higher number of views (19,491 [10,132–61,162] vs. 11,208 [8183–20,538]), a longer time online (1156 [719–2254] vs. 832 [487–1708] days), and a shorter duration (6.3 [3.4–15.8] vs. 11.8 [7.4–20.3] min). Engagement parameters were similar between useful and misleading videos. Useful videos had higher reliability, comprehensiveness, and quality scores. Useful videos were mainly uploaded by independent users and government/news agencies; academic organizations offered only 15% of useful videos.
ConclusionsMost of the information in YouTube® for Spanish-speaking patients with RA is useful; however, patient engagement is similar between useful and misleading content. More substantial involvement of academia in developing high-quality educational multimedia is warranted.
Las redes sociales (ReSo) han redefinido el acceso a la información en salud, beneficiando a los pacientes con artritis reumatoide (AR). No se cuenta con una evaluación de las características de su contenido para pacientes hispanohablantes. Nuestro objetivo fue evaluar los parámetros de interacción, la confiabilidad, la exhaustividad y la calidad de la información disponible en YouTube® para pacientes hispanohablantes con AR.
MétodosEvaluamos los videos en español sobre AR disponibles en YouTube®. Se extrajo información sobre la duración del video, los parámetros de interacción (por ejemplo, vistas, likes, índice de popularidad), el tiempo en línea y la fuente generadora. Estimamos la confiabilidad (DISCERN), la exhaustividad (puntaje de contenido) y la calidad (Global Quality Score) utilizando puntajes estandarizados.
ResultadosIncluimos 200 videos en el estudio y clasificamos a 67% como videos útiles. Estos videos tuvieron un mayor número de vistas (19.491 [10.132-61.162] vs. 11.208 [8.183-20.538]), un mayor tiempo en línea (1.156 [719-2.254] vs. 832 [487-1.708] días) y una menor duración (6,3 [3,4-15,8] vs. 11,8 [7,4-20,3] min). Los parámetros de interacción fueron similares entre los videos útiles y los no útiles. Los videos útiles presentaron puntajes mayores de confiabilidad, exhaustividad y calidad; en su mayoría fueron generados por usuarios independientes y por organizaciones gubernamentales/agencias de noticias. Las organizaciones académicas generaron únicamente 15% de los videos útiles.
ConclusionesLa mayoría de la información en YouTube® para pacientes hispanohablantes con AR es útil. Sin embargo, los parámetros de interacción son similares entre los videos útiles y los no útiles. Se requiere una mayor participación de las organizaciones académicas en el desarrollo de multimedia educativo de alta calidad.
Rheumatoid arthritis (RA) is a chronic autoimmune disease, and a significant cause of disability and decreased quality of life.1 Multiple studies identified that patients with more information about their disease have better symptoms control, present improved health outcomes, and are more comfortable with decision-making on their disease.2,3 The 2021 EULAR recommendations for the self-management of patients with inflammatory arthritis highlighted the importance of education to this end.4 For this reason, patients must have access to simple, accurate, and reliable information.3,5
In Latin America, a study identified that 70% of the population has access to the internet (i.e., internet penetration), with 85% of people having access to social media (SoMe).6 Even in the rural population that does not have personal access to the Internet, a significant proportion has relatives who do have internet access.5 SoMe's benefits include the ability to disseminate health information in a scalable way; to encourage the participation of patients in the development of health policies; to provide access to patient opinions and to offer a platform for medical education.5–7 However, SoMe is also a potential source of medical misinformation. There is evidence of a faster distribution of fake news in SoMe when compared with reliable information.7
In a previous study, Singh et al. identified that 55% of videos on YouTube® for English-speaking patients with RA were useful.2 In the case of Spanish-speaking patients, we previously reported that up to 95% of videos on YouTube® on systemic lupus erythematosus (SLE) are useful.8 Nevertheless, an attempt to assess the quality of information for Spanish-speaking patients with RA is lacking.
This study aims to describe the general characteristics and quality of the information shown by YouTube® videos in Spanish about RA, using previously applied and standardized evaluation tools.2,8–13 We evaluate their quality, reliability, and comprehensiveness and describe the differences between reliable and misleading videos, and the differences according with the generating sources.
MethodsWe performed an analytical observational study evaluating the videos about RA on YouTube® in Spanish. We included videos that presented information on epidemiology, risk factors, symptoms, diagnosis, treatment, or other relevant information on RA. We excluded duplicated videos. The study was considered no-risk research, in agreement with the Helsinki declaration, and was approved by the Institutional Research and Ethics Committee (FM-CIE-004-20).
Data collection methodsWe created an exclusive YouTube® account for this research and performed the search strategy using the incognito mode (Chrome web browser) to minimize the risk of bias based on previous searches. We performed the search on March 2nd, 2022, using the words “artritisreumatoide” and organized the results according with the number of visits. No filters were applied. We aimed to select the first 200 videos in Spanish based on previous reports that described that 90% of users consume only the information displayed within the first three pages of results.14 Videos were assessed by board-certified physicians, specialists in internal medicine, and who hold a certification in the diagnosis of patients with articular pain by the Pan-American League of Associations for Rheumatology (PANLAR). We retrieved general information using a standardized electronic format, including web address, publication date, duration, and the number of interactions (i.e., views, likes). We extracted this information on the same date that we performed the search. All videos were independently watched and analyzed by two reviewers (JBC and CRO), who performed data extraction and allocation to ‘source’ and ‘useful/misleading’ categories (see below). Whenever video labeling was considered ambiguous, the research team defined by consensus which group it was assigned to.
Time on the internet was defined as the time from video publication to the data extraction in days.2 To establish video engagement, we calculated different previously used indexes,2,8,15,16 as it is still a matter of debate how to objectively measure a publication's relative impact to provide an adjusted engagement parameter aside from the time available on the internet. The popularity index (also known as view ratio) was defined as the ‘number of views’ divided by ‘time on the internet’.2,15,16Like ratio was defined as (number of likes/[number of dislikes+number of likes])*100.15,16Video power index was defined as (Like ratio*popularity index)/100.15,16
We classified videos according to their generating source as (1) independent users, (2) government/news agencies, (3) professional organizations/academic channels (e.g., universities), (4) health information websites, or (5) medical advertisements/for-profit companies.2
Additionally, we categorized videos into four groups: useful, misleading, useful patient's opinion, and misleading patient's opinion.13
- (1)
A ‘useful’ video contained scientifically correct and accurate information about any aspect of the disease;
- (2)
A ‘misleading’ video contained scientifically unproven or inaccurate information based on currently available scientific evidence (e.g., unsubstantiated claims about pathogenesis, treatment with unproven dietary, herbal, or alternative therapy, or negative recommendations about evidence-based treatment);
- (3)
A ‘useful patient's opinion’ video described a patient's personal experience of feelings while having/being treated for the disease, which offered emotional support whenever it provided scientifically correct and accurate information about any aspect of the disease or; and
- (4)
A ‘misleading patient's opinion’ video described a patient's personal experience or feelings while having/being treated for the disease whenever it claimed scientifically unproven or inaccurate information based on currently available scientific evidence.
All videos were independently watched and analyzed by two reviewers (JBC and CRO), who evaluated all videos for reliability, comprehensiveness, and quality using standardized and previously reported scores for each characteristic.2,8–13 Whenever the information was considered ambiguous, the research team (including specialists in internal medicine and rheumatology) reviewed data and reached a consensus. We established concordance between assessors (see below).
Reliability was defined as the presentation of correct and accurate information from a scientific point of view on any aspect of the disease. As previously reported,2 we applied the modified 5-point DISCERN tool (Supplementary Table 1), which comprises five questions and is scored from 0 to 5, based on the reviewers’ criteria; this tool was modified from the original DISCERN tool, which was developed by Charnock et al. to evaluate written health information.17
Comprehensiveness was defined as how exhaustive and complete the information presented on the disease.18 We applied a previously proposed content score (Supplementary Table 2), which comprises five domains and is scored from 0 to 5.2
Quality was defined as how useful the reviewer considers would be the presented information to a patient. We applied the Global Quality Score (GQS) tool (Supplementary Table 3), a 5-point scale to rate the overall quality of a video.2,9–12
Statistical analysisWe expressed categorical variables as absolute and relative frequencies, whereas continuous variables as medians and interquartile ranges. We evaluated data normality using the Shapiro–Wilk test. We considered the reliability (DISCERN), comprehensiveness (content score), and quality (GQS) score as quantitative variables. Before video assessment, we established inter-rater reliability by performing a pilot evaluation. This evaluation aimed to standardize how to rate each of the scores’ items, as we acknowledged the subjectivity of the available and previously used instruments to assess SoMe resources.2,8–13 The research team discussed each item to establish a standardized approach. Then, we randomly selected 20 videos to be appraised by the evaluators, who independently rated each. We calculated Cohen's Kappa coefficient for each tool to determine concordance between evaluators. We dichotomized the three tools as ‘good or higher’ or ‘bad’: ‘good or higher’ included 3, 4, and 5 scores, whereas ‘bad’ included 1 and 2 scores.
Based on usefulness (e.g., useful, misleading, useful patient's opinion, and misleading patient's opinion) and the source categories, we compared the time on the internet, the number of interactions, the popularity index, the like ratio, the video power index, and the scores on each of the tools, using a Chi-squared test for qualitative variables or non-parametric tests (Mann–Whitney U test for pairwise comparisons or Kruskal–Wallis test for multiple comparisons) for quantitative variables. Further, we performed correlation analysis between quantitative variables using Spearman's rank correlation coefficient. The p values <0.05 were considered significant. We performed statistical analyses using STATA (Stata Statistical Software: Release 14. College Station, TX: StataCorp LLC).
ResultsGeneral characteristics and concordance between ratersWe retrieved 200 videos. After review, we did not exclude any of them. We found a median of 15,504 (interquartile range [IQR] 9439–52,743) views, with a median length of 8.8min (IQR 3.6–17.6) and a median of 1076 days online (656–1989). Only 15.5% were from professional organizations or academic channels. Concerning assessment scores, reliability (DISCERN) median value was 3 (1–3), comprehensiveness (content score) median value was 2 (1–3), and quality (GQS) median value was 3 (2–3.5). The agreement between independent raters was substantial, with a Cohen's Kappa coefficient of 0.775 (95% confidence interval [CI] 0.684; 0.867) for quality (GQS), and almost perfect (0.864; 95% CI 0.793; 0.936) for comprehensiveness (content score), and for reliability (DISCERN) (0.888; 95% CI 0.824; 0.952). One hundred thirty-five videos (67.5%) were considered useful. We present the characteristics by usefulness category in Tables 1 and 2.
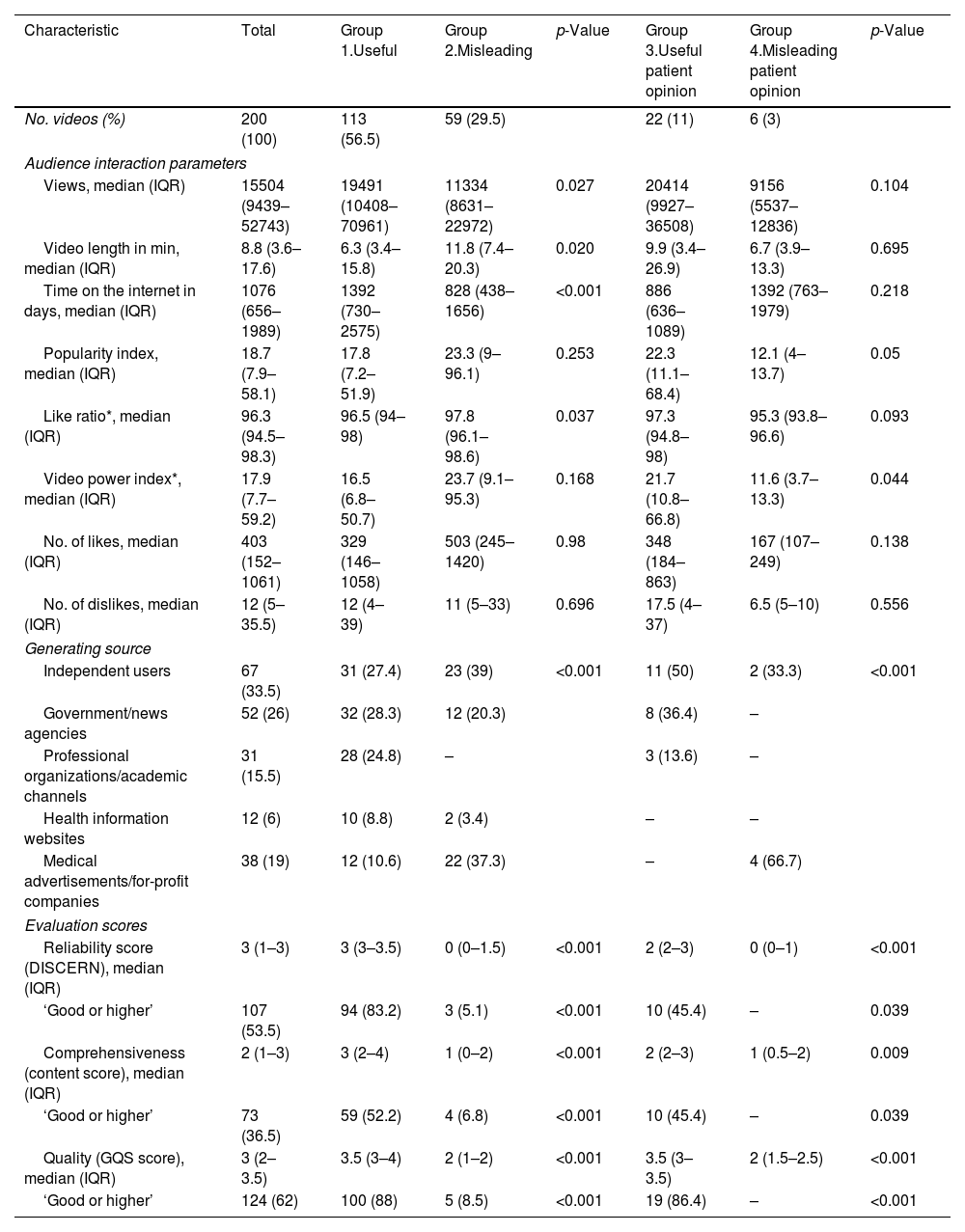
Characteristics of videos in Spanish on YouTube® on rheumatoid arthritis by usefulness category.
| Characteristic | Total | Group 1.Useful | Group 2.Misleading | p-Value | Group 3.Useful patient opinion | Group 4.Misleading patient opinion | p-Value |
|---|---|---|---|---|---|---|---|
| No. videos (%) | 200 (100) | 113 (56.5) | 59 (29.5) | 22 (11) | 6 (3) | ||
| Audience interaction parameters | |||||||
| Views, median (IQR) | 15504 (9439–52743) | 19491 (10408–70961) | 11334 (8631–22972) | 0.027 | 20414 (9927–36508) | 9156 (5537–12836) | 0.104 |
| Video length in min, median (IQR) | 8.8 (3.6–17.6) | 6.3 (3.4–15.8) | 11.8 (7.4–20.3) | 0.020 | 9.9 (3.4–26.9) | 6.7 (3.9–13.3) | 0.695 |
| Time on the internet in days, median (IQR) | 1076 (656–1989) | 1392 (730–2575) | 828 (438–1656) | <0.001 | 886 (636–1089) | 1392 (763–1979) | 0.218 |
| Popularity index, median (IQR) | 18.7 (7.9–58.1) | 17.8 (7.2–51.9) | 23.3 (9–96.1) | 0.253 | 22.3 (11.1–68.4) | 12.1 (4–13.7) | 0.05 |
| Like ratio*, median (IQR) | 96.3 (94.5–98.3) | 96.5 (94–98) | 97.8 (96.1–98.6) | 0.037 | 97.3 (94.8–98) | 95.3 (93.8–96.6) | 0.093 |
| Video power index*, median (IQR) | 17.9 (7.7–59.2) | 16.5 (6.8–50.7) | 23.7 (9.1–95.3) | 0.168 | 21.7 (10.8–66.8) | 11.6 (3.7–13.3) | 0.044 |
| No. of likes, median (IQR) | 403 (152–1061) | 329 (146–1058) | 503 (245–1420) | 0.98 | 348 (184–863) | 167 (107–249) | 0.138 |
| No. of dislikes, median (IQR) | 12 (5–35.5) | 12 (4–39) | 11 (5–33) | 0.696 | 17.5 (4–37) | 6.5 (5–10) | 0.556 |
| Generating source | |||||||
| Independent users | 67 (33.5) | 31 (27.4) | 23 (39) | <0.001 | 11 (50) | 2 (33.3) | <0.001 |
| Government/news agencies | 52 (26) | 32 (28.3) | 12 (20.3) | 8 (36.4) | – | ||
| Professional organizations/academic channels | 31 (15.5) | 28 (24.8) | – | 3 (13.6) | – | ||
| Health information websites | 12 (6) | 10 (8.8) | 2 (3.4) | – | – | ||
| Medical advertisements/for-profit companies | 38 (19) | 12 (10.6) | 22 (37.3) | – | 4 (66.7) | ||
| Evaluation scores | |||||||
| Reliability score (DISCERN), median (IQR) | 3 (1–3) | 3 (3–3.5) | 0 (0–1.5) | <0.001 | 2 (2–3) | 0 (0–1) | <0.001 |
| ‘Good or higher’ | 107 (53.5) | 94 (83.2) | 3 (5.1) | <0.001 | 10 (45.4) | – | 0.039 |
| Comprehensiveness (content score), median (IQR) | 2 (1–3) | 3 (2–4) | 1 (0–2) | <0.001 | 2 (2–3) | 1 (0.5–2) | 0.009 |
| ‘Good or higher’ | 73 (36.5) | 59 (52.2) | 4 (6.8) | <0.001 | 10 (45.4) | – | 0.039 |
| Quality (GQS score), median (IQR) | 3 (2–3.5) | 3.5 (3–4) | 2 (1–2) | <0.001 | 3.5 (3–3.5) | 2 (1.5–2.5) | <0.001 |
| ‘Good or higher’ | 124 (62) | 100 (88) | 5 (8.5) | <0.001 | 19 (86.4) | – | <0.001 |
p values calculated using the Mann–Whitney test for quantitative variables and χ2 or Z-test for qualitative variables.
‘Good or higher’ is considered if the score is equal to 3 or more.
Useful videos contained scientifically correct and accurate information about any aspect of the disease.
Misleading videos contained scientifically unproven or inaccurate information based on currently available scientific evidence (e.g., unsubstantiated claims about pathogenesis and treatment with unproven dietary, herbal, or alternative therapy, or negative portrayal of evidence-based treatment).
Useful patient opinion videos described a patient's personal experience of feelings while having/being treated for the disease, which offered emotional support whenever it provided scientifically correct and accurate information about any aspect of the disease.
Misleading patient opinion videos described a patient's personal experience or feelings while having/being treated for the disease whenever it claimed scientifically unproven or inaccurate information based on currently available scientific evidence.
Time on the internet was defined as the time from video publication to data extraction in days.
Popularity index was defined as the ‘number of views’ divided by ‘time on the internet’.
Reliability was defined as the presentation of correct and accurate information from a scientific point of view on any aspect of the disease.
Comprehensiveness was defined as how exhaustive and complete the information presented on the disease.
Quality was defined as how useful the reviewer considered would be the presented information to a patient.
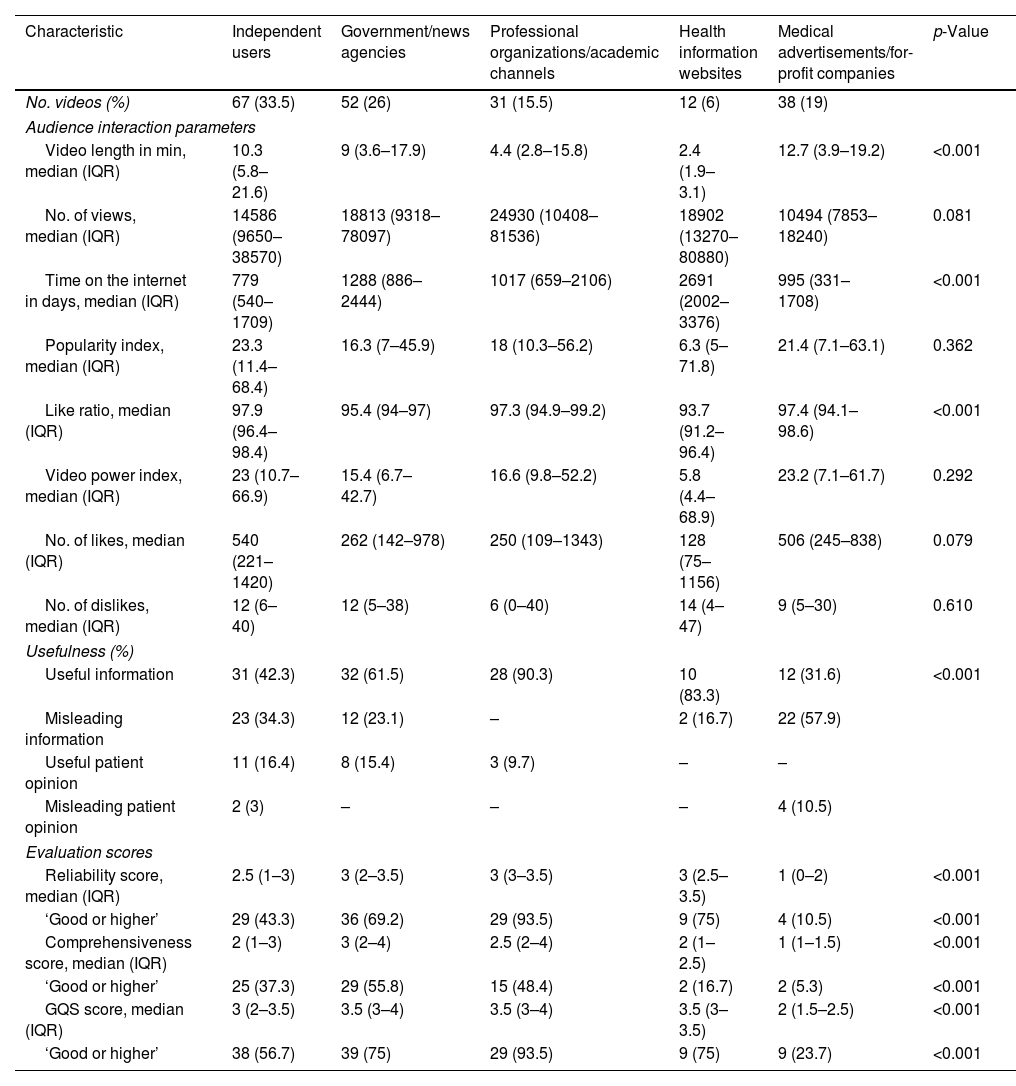
Characteristics of videos in Spanish on YouTube® on rheumatoid arthritis by source.
| Characteristic | Independent users | Government/news agencies | Professional organizations/academic channels | Health information websites | Medical advertisements/for-profit companies | p-Value |
|---|---|---|---|---|---|---|
| No. videos (%) | 67 (33.5) | 52 (26) | 31 (15.5) | 12 (6) | 38 (19) | |
| Audience interaction parameters | ||||||
| Video length in min, median (IQR) | 10.3 (5.8–21.6) | 9 (3.6–17.9) | 4.4 (2.8–15.8) | 2.4 (1.9–3.1) | 12.7 (3.9–19.2) | <0.001 |
| No. of views, median (IQR) | 14586 (9650–38570) | 18813 (9318–78097) | 24930 (10408–81536) | 18902 (13270–80880) | 10494 (7853–18240) | 0.081 |
| Time on the internet in days, median (IQR) | 779 (540–1709) | 1288 (886–2444) | 1017 (659–2106) | 2691 (2002–3376) | 995 (331–1708) | <0.001 |
| Popularity index, median (IQR) | 23.3 (11.4–68.4) | 16.3 (7–45.9) | 18 (10.3–56.2) | 6.3 (5–71.8) | 21.4 (7.1–63.1) | 0.362 |
| Like ratio, median (IQR) | 97.9 (96.4–98.4) | 95.4 (94–97) | 97.3 (94.9–99.2) | 93.7 (91.2–96.4) | 97.4 (94.1–98.6) | <0.001 |
| Video power index, median (IQR) | 23 (10.7–66.9) | 15.4 (6.7–42.7) | 16.6 (9.8–52.2) | 5.8 (4.4–68.9) | 23.2 (7.1–61.7) | 0.292 |
| No. of likes, median (IQR) | 540 (221–1420) | 262 (142–978) | 250 (109–1343) | 128 (75–1156) | 506 (245–838) | 0.079 |
| No. of dislikes, median (IQR) | 12 (6–40) | 12 (5–38) | 6 (0–40) | 14 (4–47) | 9 (5–30) | 0.610 |
| Usefulness (%) | ||||||
| Useful information | 31 (42.3) | 32 (61.5) | 28 (90.3) | 10 (83.3) | 12 (31.6) | <0.001 |
| Misleading information | 23 (34.3) | 12 (23.1) | – | 2 (16.7) | 22 (57.9) | |
| Useful patient opinion | 11 (16.4) | 8 (15.4) | 3 (9.7) | – | – | |
| Misleading patient opinion | 2 (3) | – | – | – | 4 (10.5) | |
| Evaluation scores | ||||||
| Reliability score, median (IQR) | 2.5 (1–3) | 3 (2–3.5) | 3 (3–3.5) | 3 (2.5–3.5) | 1 (0–2) | <0.001 |
| ‘Good or higher’ | 29 (43.3) | 36 (69.2) | 29 (93.5) | 9 (75) | 4 (10.5) | <0.001 |
| Comprehensiveness score, median (IQR) | 2 (1–3) | 3 (2–4) | 2.5 (2–4) | 2 (1–2.5) | 1 (1–1.5) | <0.001 |
| ‘Good or higher’ | 25 (37.3) | 29 (55.8) | 15 (48.4) | 2 (16.7) | 2 (5.3) | <0.001 |
| GQS score, median (IQR) | 3 (2–3.5) | 3.5 (3–4) | 3.5 (3–4) | 3.5 (3–3.5) | 2 (1.5–2.5) | <0.001 |
| ‘Good or higher’ | 38 (56.7) | 39 (75) | 29 (93.5) | 9 (75) | 9 (23.7) | <0.001 |
p values calculated using Kruskal–Wallis test for quantitative variables and χ2 for qualitative variables.
‘Good or higher’ is considered if the score is equal to 3 or more.
Useful videos contained scientifically correct and accurate information about any aspect of the disease.
Misleading videos contained scientifically unproven or inaccurate information based on currently available scientific evidence (e.g., unsubstantiated claims about pathogenesis and treatment with unproven dietary, herbal, or alternative therapy, or negative portrayal of evidence-based treatment).
Useful patient opinion videos described a patient's personal experience of feelings while having/being treated for the disease, which offered emotional support whenever it provided scientifically correct and accurate information about any aspect of the disease.
Misleading patient opinion videos described a patient's personal experience or feelings while having/being treated for the disease whenever it claimed scientifically unproven or inaccurate information based on currently available scientific evidence.
Time on the internet was defined as the time from video publication to data extraction in days.
Popularity index was defined as the ‘number of views’ divided by ‘time on internet’.
Reliability was defined as the presentation of correct and accurate information from a scientific point of view on any aspect of the disease.
Comprehensiveness was defined as how exhaustive and complete the information presented on the disease.
Quality was defined as how useful the reviewer considered would be the presented information to a patient.
*We included 198 videos, as there were 2 videos had 0 likes and 0 dislikes (one from Professional organizations/academic channels and one from medical advertisements/for-profit companies).
Further, we performed exploratory correlation analysis for quantitative variables (Supplementary Table 6). We found significant strong correlations (<−0.7 or >0.7, p<0.05) for the following variables: number of views with number of likes (r=0.73) or dislikes (r=0.83), and a fair correlation with popularity index and video power index (r=0.67, both); popularity index with video power index (r=0.99), likes (r=0.87), or dislikes (r=0.69); video power index with likes (r=0.87), or dislikes (r=0.68); likes with dislikes (r=0.8); reliability score (DISCERN) with content score (r=0.63), or quality score (GQS, r=0.72); content score with quality score (GQS, r=0.72).
Useful (group 1) vs. misleading (group 2) videosGroup 1 had a higher number of views (19,491 [10,408–70,961] vs. 11,334 [8631–22,972], p=0.027), a longer time on the internet (1392 [730–2575] vs. 828 [438–1656] days, p<0.001) and had shorter duration (6.3 [3.4–15.8] vs. 11.8 [7.4–20.3] min, p=0.020). Group 2 had a significantly higher like ratio (96.5 [94–98] vs. 97.8 [96.1–98.6], p=0.037), with no significant differences in the other audience interaction parameters (i.e., popularity index, number of likes or dislikes, video power index). Regarding evaluation scores, group 1 had higher assessment scores, and a larger proportion was classified as ‘good or higher’ in all evaluation scores. The most frequent source of useful videos were government/news agencies’ channels, whereas for-profit users uploaded more often misleading videos (Table 1 and Supplementary Table 4).
Useful (group 3) vs. misleading (group 4) patient opinion videosRegarding patients’ opinions, group 3 had higher video power index (21.7 [10.8–66.8] vs. 11.6 [3.7–13.3], p=0.044), with no significant differences in the other audience interaction parameters. Evaluation scores were also higher for videos from group 3. Noteworthy, the most frequent source for group 4 was for-profit users (Table 1).
Videos by sourceThe most common sources were independent users and government/news agencies. Useful information was uploaded more frequently by academic sources or government/news agencies, whereas for-profit companies more frequently uploaded misleading information. Professional organizations or academic channels uploaded 15% of videos; all were rated as useful. As for the audience interaction parameters, professional institutions and health information websites had the shortest videos (4.4min [2.8–15.8] and 2.4min [1.9–3.1], respectively) and a significant difference was observed for the like ratio among different sources, probably due to a lower value in videos from health information websites. No statistical differences in other engagement parameters were observed. Additionally, 93.5% of videos from professional organizations were considered ‘good or higher’ in their reliability and quality scores (Table 2).
DiscussionMost of the information in SoMe for Spanish-speaking patients with RA is useful. However, although useful videos are more frequently watched, other engagement parameters (e.g., popularity index, likes/dislikes) are similar between useful and misleading videos. Quality, reliability, and comprehensiveness scores were higher for useful videos. Most useful videos are uploaded by independent users or government/news agencies, while for-profit companies offer misleading videos; noteworthy, academic sources are less common. To the best of our knowledge, we offer the first evaluation of videos in SoMe for Spanish-speaking patients with RA.
Ten years ago, Singh et al. published the first study evaluating the usefulness of information on YouTube® for English-speaking patients with RA.2 The authors reported that 55% of videos were useful, with no differences in engagement parameters between groups. We found a higher proportion of useful videos with a similar engagement behavior. In contrast, previous studies on the usefulness of the information on YouTube® for Spanish-speaking patients for other immune-mediated inflammatory diseases (IMIDs), such as SLE and inflammatory bowel disease (IBD), reported a higher proportion of useful videos (67.5% for RA vs. 95.1% for SLE or 98% for IBD).8,19 Nevertheless, our study found a higher proportion of useful videos than when contrasting our findings with studies assessing videos in English on Sjögren's syndrome, psoriasis, SLE, and application method of injectable medications such as anti-TNF or methotrexate10,11,13,20–23 (Supplementary Figure 1). Regarding correlation analysis we highlight the positive significant correlation between number of views and engagement parameters such as likes, dislikes, popularity index, and video power index. We consider that the most plausible explanation is the fact that a higher number of views increases the chance of a larger number of likes or dislikes. Further, as both the popularity index and the video power index calculations rely on the number of views, this positive relation would be expected. Interestingly, the fact of a near perfect correlation between the latter and the former is encouraging as it may suggest that both reflect the same adjusted engagement parameter aside from the time available on the internet, by means of a different arithmetic approach; a standardized definition should be sought. In addition, a strong correlation between reliability, comprehensiveness, and quality scores may reflect that, although each evaluates multimedia from different points of view, all are improved when the video is generated using accurate information from a scientific point of view.
Differences observed for videos in Spanish, which have been evaluated since 2020, may be due to the recently adopted policy on the quality of information by YouTube®.24 Onder et al. reported a similar result, with a search performed in April 2021 to assess the quality of videos on psoriatic arthritis on YouTube®.20 Some other articles on relevant issues for IMIDs have been recently published22,25–31; however, their classification methods differ from our approach, thus, limiting comparisons. Regarding engagement parameters between useful and misleading videos, the subtle differences between both groups implies that Spanish-speaking patients with RA may not identify helpful information for their disease. As previously suggested,8 this issue may be overcome by offering high-quality and appealing content. Nonetheless, several studies have shown that YouTube® is not a good source of education for patients. A study on the quality of information of YouTube® videos on knee osteoarthritis and total knee arthroplasty found that 66% of the included videos (n=56) on knee osteoarthritis and 64% of the included videos (n=50) on arthroplasty presented a poor quality, based on an author's generated specific content score.32 A similar study on the diagnosis and treatment of hip arthritis found that 84% of the included videos (n=133) presented a poor quality.33 A study on total knee arthroplasty (90%, n=40) reported an even higher percentage.34 Using a different approach, Fischer et al. reported that 40% of videos (n=13) on knee arthrocentesis were unhelpful, based on a scarce agreement with evidence-based guidelines.35 Lastly, a study similar to ours on the reliability and educational value of YouTube® videos on injuries to the posterior cruciate ligament of the knee found a low-reliability value (mean 2.02, maximum score 4), using the Journal of the American Medical Association benchmark criteria; further, educational value scores were also low using both a nonspecific content score (GQS, mean 2.3) and an author's generated specific content score (mean 2.9, maximum score 18).36 Compared to our results, GQS mean value was lower (2.3 vs. 3), although one should ascertain that the authors reported mean values. In contrast, we reported median values, a fact that limits comparability. Although the authors of this study did not classify videos based on their utility, their results illustrate a low reliability and educational value.
Physician-patient shared-decision is the hallmark of patient-centered care,18 in which patient education plays a pivotal role in achieving informed decision-making to improve outcomes. The current management guidelines of RA support this approach.37,38 SoMe allow the massive distribution of self-paced educational sources. Aside of the relevance of fostering education among patients, the 2021 EULAR recommendations for the self-management of patients with inflammatory arthritis encourage the use of digital healthcare tools to improve self-management and self-efficacy, that, in turn, will improve patients’ outcomes.4 The development of high-quality educational resources should be promoted. Surprisingly, most useful information was uploaded by independent users or government/news agencies, with a relatively small share of videos offered by professional organizations. Studies assessing videos on RA in English reported a similar trend,2 in which academic sources uploaded only 20%. Studies in other IMIDs have replicated these results.12–14,17 Nonetheless, the case of SLE deserves further discussion, as mainly academic sources upload information for both English and Spanish speaking patients.8,13 Drenkard et al.6 offered a detailed description of their experience developing Let's Talk About Lupus, which should be considered a call to action to foster the involvement of academic organizations in the development of evidence-based educational tools. Of interest, Centers of Excellence in RA developed some of the assessed videos in our study, a follow-up approach that has influenced clinical outcomes39–41; thus, suggesting that the shortage of videos from academic sources is increasingly recognized.
Unfortunately, patients with RA are prone to present disabling deformities that limit their productivity potential. In fact, this is one of the variables rheumatologists assess to establish disease activity and treatment effectiveness.42 Consequently, up to 40% of patients with RA may present work disability (i.e., the cessation of paid employment, or receiving working disability benefits, or working less than full time) as early as five years from the diagnosis of the disease.43 Several videos from law firms approached this issue and offered support to obtain early retirement benefits. Rheumatologists and health workers who care for RA patients should be aware of these issues, as evidence-based interventions have been suggested to allow early detection and intervention of at-risk patients, thus, improving their chances of retaining productivity.43 Discussion with patients about work should be sought and supported, where appropriate.4 This topic should be considered a priority in developing educational videos for patients with RA.
Several videos in our research addressed dietary interventions, and the vast majority declared that nutrition could cure RA. Growing evidence supports the relevance of a healthy diet in managing RA, particularly in patients under stable, optimized drug therapy.44 Although evidence to support an improvement in outcomes remains to be elucidated, a healthy diet has been demonstrated to reduce the risk for cardiovascular events45; to date, no evidence of dietary-induced RA remission is available. A similar approach should be made concerning complementary and alternative medicine.46 Further, several videos addressed physiotherapy and physical exercise for patients with RA. High-quality evidence is still lacking; however, as mentioned by Hu et al. in their metanalysis on this topic, “any exercise is better than no exercise”.47 In summary, incorporating wellness practices into managing patients with RA should be a growing priority for rheumatologists,45 as supported by recent EULAR recommendations.4 These issues are of significant relevance to patients; thus, multimedia that contain reliable and peer-reviewed information should be encouraged.
We acknowledge some limitations of our study. First, we evaluated only Spanish-language videos on YouTube®, thus, overlooking information in other languages. Second, we included only multimedia on one SoMe platform. Recent evidence suggests that patients with IMIDs may be more prone to access health information on Facebook®6; thus, future studies should consider its inclusion. Third, we used previously reported scores2,8–13 to assess the quality of multimedia, which report subjective ratings by independent evaluators. Although our concordance test rendered an adequate concordance, in line with previous reports,2,8–13 it is essential to call for the development of validated tools to evaluate the growing wave of health-related multimedia objectively. Fourth, as YouTube® is a dynamic platform renewed daily, a cross-sectional study should capture only “one snapshot”; this limitation is expected for this methodology. Finally, the fact that physicians performed the assessment may not reflect the perception of quality and content that a patient may obtain from a video. Future studies should invite disease-specific educated patients to assess multimedia quality and usefulness.
ConclusionsMost of the information in YouTube® for Spanish-speaking patients with RA is useful; however, patient engagement is similar between useful and misleading content. More substantial involvement of academia in developing high-quality educational multimedia is warranted.
Authors’ contributionsAll authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by Julián E. Barahona-Correa, Camilo Rueda-Ortiz, Angel Alberto García, Oscar Muñoz, and Daniel G. Fernández-Ávila. The manuscript was drafted by Julián E. Barahona-Correa and Camilo Rueda-Ortiz; all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
FundingNone declared.
Conflict of interestThe authors declare no conflict of interest for the present study.
We thank our patients and their families, for whom we have inspired our research.
The following are the supplementary data to this article:


