





IgG4-related disease is characterized by a lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells, storiform fibrosis and obliterative phlebitis. It can present as parotid gland enlargement, tubulointerstitial nephritis, retroperitoneal fibrosis or pancreatitis, although nearly any organ can be affected. We report the case of a 37-year-old woman who presented with severe dysphonia and recurrent painful aphthous ulcers, with histopathological findings at the level of the larynx that revealed a lymphoplasmacytic infiltrate and IgG4 positivity. In addition, extensive studies were performed to rule out other diseases. Thus the diagnosis was IgG4-related laryngitis, an exceptional finding in the literature.
La enfermedad relacionada con IgG4 (ER-IgG4) se caracteriza por un infiltrado linfoplasmocítico rico en células plasmáticas IgG4 positivas, fibrosis estoriforme y flebitis obliterativa. Se puede presentar como seudotumor orbitario, parotidomegalia, nefritis túbulo intersticial, fibrosis retroperitoneal o pancreatitis, aunque prácticamente cualquier órgano puede verse afectado. Presentamos el caso de una mujer de 37 años, que presenta un cuadro de disfonía severa y aftosis oral dolorosa recurrente, con unos hallazgos histopatológicos a nivel laríngeo que muestran infiltrado linfoplasmocítico y positividad para IgG4, así como amplios estudios descartando otras etiologías, por lo que se confirma una laringitis por ER-IgG4, cuya descripción en la literatura es excepcional.
IgG4 (ER-IgG4)-related disease is characterized by a lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells, storiform fibrosis and obliterative phlebitis.1,2 It can present as orbitary pseudo tumour, paratoid gland enlargement, tubulointerstitial nephritis, retroperitoneal fibrosis or pancreatitis, although nearly any organ can be affected.3,4
We report the case of a woman with refractory laryngitis and recurrent oral aphthosis, where an IgG4-related disease was revealed, a syndrome which has only been reported exceptionally in the literature.5
A 27-year-old woman who presented with severe dysphonia of 3 year onset, and painful oral aphthous ulcers which spontaneously receded after around 2 weeks, with several outbreaks per year. She did not report dry syndrome, uveitis, arthritis, acne, thrombosis, diarrhoeas, abdominal pain or episodes of chondritis. She had received treatment with omeprazol, as well as aciclovir and low doses of oral corticoids due to the aphthosis, with no improvement.
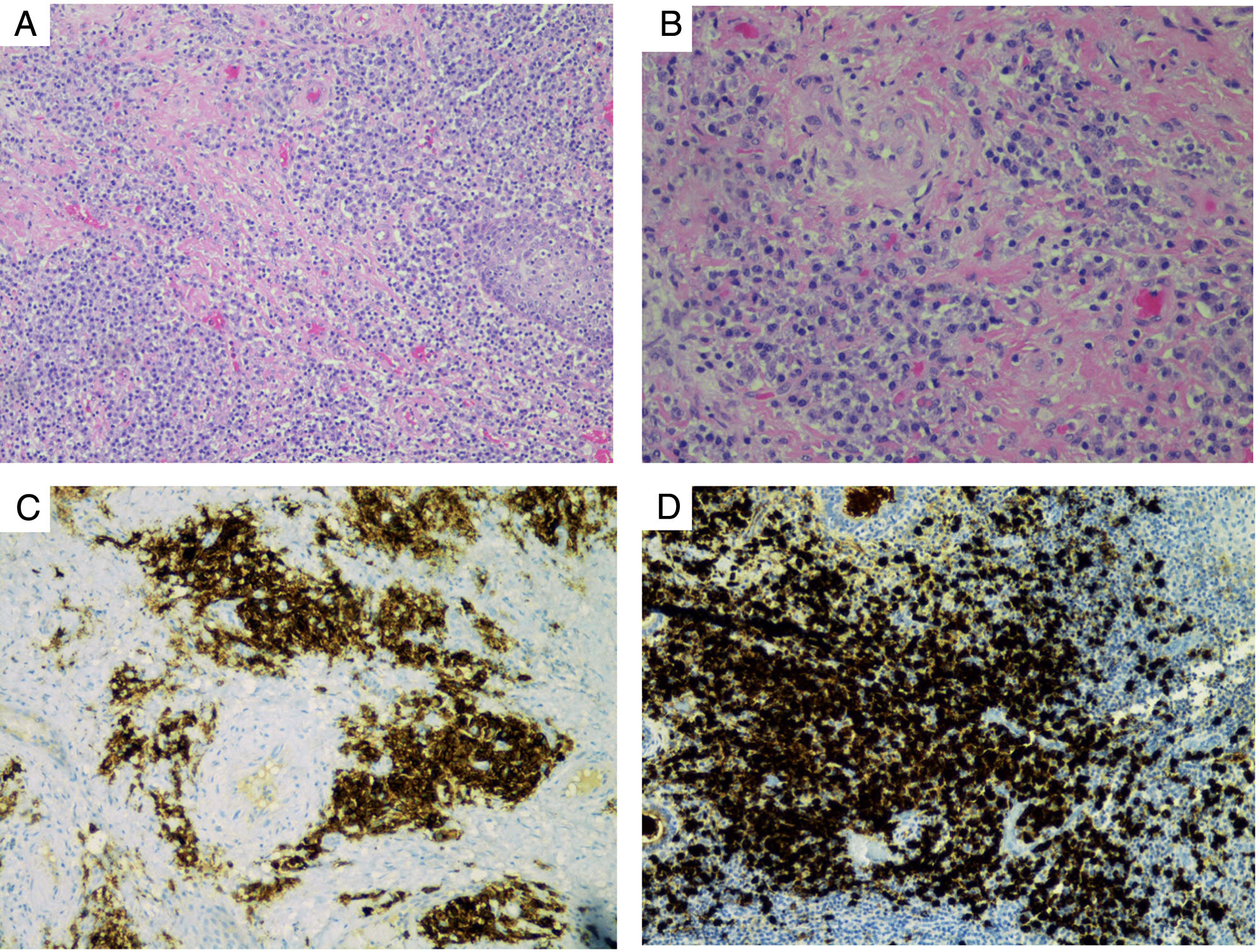
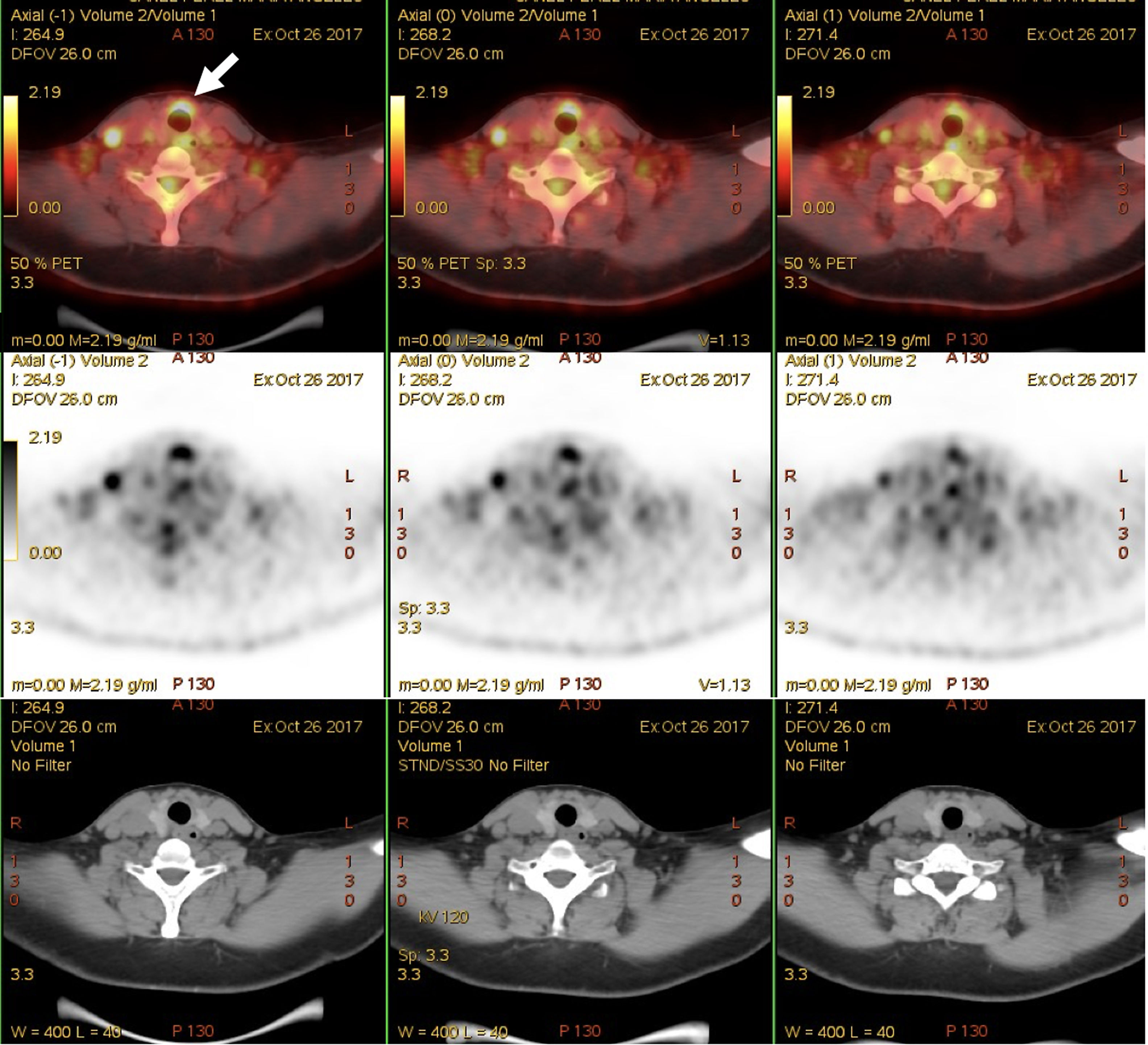
General and ophthalmological examination was normal, except for the dysphonia and a fibroscopy confirmed intense laryngitis. Complete blood count, general biochemistry, ESR and C-reactive protein tested normal. Determination of HLA-B5, ANA, ANCA, anti-transgluaminase IgA antibodies and HIV serology tested negative. Computerized tomography of the neck and chest only showed contrast enhanced uptake at laryngeal level and small non-specific laterocervical adenopathies. A laryngeal biopsy showed an inflammatory infiltrate with positive immunohistochemistry for IgG4, and IgG4/IgG-related disease of nearly 40% (Fig. 1). No plasmablasts were observed (lymphocytes with CD19+CD24−CD38hi phenotype) in peripheral blood. Serum IgG4: 1.40U (N: .05–1.25). A 18F-FDG PET/CT scan showed laryngeal level uptake, but not at blood vessel or other cartilaginous structure level (Fig. 2).
On diagnosis of IgG4-related disease with laryngeal involvement, treatment was initiated with 3 boluses of 125mg of methylprednisolone, followed by oral prednisone (.4mg/kg/day) with gradual tapering, adding azathioprine as a steroid replacement, with improvement of dysphonia and with no further outbreaks of aphthosis.
IgG4-related disease is a fibro-inflammatory disease, which was first described in 2003 and the clinical spectrum of which has extended.6 An IgG4-related disease is considered possible when it affects a typical organ and there is elevated serum IgG4, probable IgG4-related disease due to the presence of typical histopathological findings and IgG4/IgG>40%. It is considered a definitive IgG4 –related disease when there is a combination of involvement of a typical organ, elevated serum IgG4 levels and compatible histopathology.7 in our patient, diagnosis of IgG4-related disease could be considered probable. Involvement of IgG4-related disease to ENT level is exceptional, and as far as we know has only be described in one case of pseudo tumour at tracheal level.8
Furthermore, the patient reported recurrent oral aphthosis for which the differential diagnosis with a Behçet disease (BD) was suggested, ruling out the most common diseases involving oral ulcers.9 A case has recently been reported of a laryngeal and oral aphthosis IgG4-related disease, similar to that of our patient, which was focused as a overlapping BD syndrome.5 Overlapping between systemic diseases is well known, including that of BD and polychondritis (MAGIC syndrome)10 or that of positive ANCA vasculitis and IgG4-related diease.3 In these cases treatment was based on the severity of the disease and the affected organs. In these cases, treatment is based on the severity and the affected organs. In IgG4-related diseases glucocorticoids are the treatment of choice, whilst steroid replacements used are azathioprine or micophenolate and rituximab for refractory or severe cases.1,2
Finally, we believe that laryngitis should be included in the clinical spectrum of IgG4-related diseases. As with other presentations of the disease which may mimic other diseases, in this case it was a BD, which could be a new overlapping syndrome.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Suárez-Díaz S, Núñez-Batalla F, Fernández-García MS, Fernández-Llana MB, Yllera-Gutiérrez C, Caminal-Montero L. Aftosis oral y laringitis, ¿otra forma de presentación de la enfermedad relacionada con IgG4? Reumatol Clin. 2020;16:416–418.


