

There are national and international clinical practice guidelines for systemic lupus erythematosus treatment. Nonetheless, most of them are not designed for the Mexican population or are devoted only to the treatment of certain disease manifestations, like lupus nephritis, or are designed for some physiological state like pregnancy. The Mexican College of Rheumatology aimed to create clinical practice guidelines that included the majority of the manifestations of systemic lupus erythematosus, and also incorporated guidelines in controversial situations like vaccination and the perioperative period. The present document introduces the “Clinical Practice Guidelines for the Treatment of Systemic Lupus Erythematosus” proposed by the Mexican College of Rheumatology, which could be useful mostly for non-rheumatologist physicians who need to treat patients with systemic lupus erythematosus without having the appropriate training in the field of rheumatology. In these guidelines, the reader will find recommendations on the management of general, articular, kidney, cardiovascular, pulmonary, neurological, hematologic and gastrointestinal manifestations, and recommendations on vaccination and treatment management during the perioperative period.
Existen varias guías de práctica clínica tanto nacionales como internacionales para el tratamiento del lupus eritematoso sistémico. No obstante, la mayoría de las guías disponibles no están diseñadas para población mexicana o solamente son para el manejo de manifestaciones específicas como nefritis lúpica o para algún estado fisiológico como el embarazo. El Colegio Mexicano de Reumatología se propuso elaborar unas guías de práctica clínica que conjuntaran la mayor parte de las manifestaciones de la enfermedad y que incluyeran adicionalmente pautas en situaciones controversiales como lo son la vacunación y el periodo perioperatorio. En el presente documento se presenta la «Guía de práctica clínica para el manejo del lupus eritematoso sistémico» propuesta por el Colegio Mexicano de Reumatología, que puede ser de utilidad principalmente a médicos no reumatólogos que se ven en la necesidad de tratar a pacientes con lupus eritematoso sistémico sin tener la formación de especialistas en reumatología. En esta guía se presentan recomendaciones sobre el manejo de manifestaciones generales, articulares, renales, cardiovasculares, pulmonares, neurológicas, hematológicas, gastrointestinales, respecto a la vacunación y al manejo perioperatorio.
Systemic lupus erythematosus (SLE) is an autoimmune disease that behaves very heterogeneously, and is characterised by remissions and exacerbations. Its incidence and prevalence adjusted by age is 5.5 per 100,000 persons (95% CI: 5.0–6.1) and 72.8 (95% CI: 70.8–74.8).1 There is no national registry of cases in Mexico but it is known that there are substantial differences in the load of the disease in different populations and countries.2 For example, the black American population have an incidence and prevalence more than twice that of the Caucasian population.1 Even among “Hispanic” populations – as Latin Americans are often grouped in clinical studies – there are significant differences in the presentation of the disease.3
There are several national and international clinical practice guidelines (CPG) for the treatment of SLE.4–7 However, the majority of those available are not designed for the Mexican population or only seek to manage specific manifestations, such as lupus nephritis, or physiological conditions, such as pregnancy. National guidelines facilitate the inclusion of certain disease in national health plans. There is no proposal as yet in this country for managing this disease that encompasses representatives of the principal health systems in a global and standardised way.
The disease has distinct features in the different ethnic groups, as reported in cohorts such as LUMINA and GLADEL.8,9 Mixed race people suffer severe forms, with a higher frequency of glomerulonephritis, higher mortality and accumulated damage. Similarly, some manifestations, such as demyelinating neuropathies and transverse myelitis, are more frequent in Latin American populations, although they usually respond better to treatment than Caucasian populations.10,11 Some studies have been published on Mexican patients, that assess biochemical variants that might be related to therapeutic response,12 and specific lupus nephritis induction treatments13 or specific response to biological drugs.14 However, these studies have the weakness that they were performed on captive populations, with a limited number of participants, and therefore general peculiarities of Mexican patients or generalised recommendations cannot be established based on this local evidence.
These facts justify the drawing up of national guidelines in a country where most of the population is of mixed race and requires access to public health systems for medical advice and treatment.
Based on the above, the Mexican College of Rheumatology (MCR) set out to draw up a CPG that would combine the majority of the disease's manifestations, and which would also include guidelines for controversial situations such as vaccination and the perioperative period. Although the recommendations provided in this CPG are based on scientific evidence, all guidelines have limitations in terms of individual decision-making, since each patient has unique features, and therefore this document, as its name states, is only intended as a guide and in no way attempts to substitute or limit the clinical judgement of the physician. Publishing this CPG marks the start of process of continuous updating which the MCR will undertake every 2 years or when appropriate in light of new evidence. The report on the evidence to support the recommendations is being drawn up to complement this guideline, and will be published later.
In preparing this guideline, we endeavoured to cover a wide range of patients. To make the recommendations we took into account publications on patients with SLE, and all organ and systemic involvement, with possible comorbidities. The only two cases that we did not consider were the paediatric population and lupus during pregnancy since the MCR already has a guideline to cover these groups.5 Because response to treatment and the presentation of the disease can differ in different ethnic groups, the recommendations were made with the Mexican population in mind. The country's socioeconomic context was taken into consideration, because the cost of some drugs can be very high for patients who are not insured or who are not right holders, and for the health institutions themselves. The recommendations included in this guideline, therefore, apply to adult, non-pregnant, Mexican patients with SLE.
This document was undertaken to provide the most complete guideline possible to serve as support particularly for non-rheumatologist doctors who have to treat patients with SLE and lack the training of rheumatology specialists. It is common for primary care doctors and those of other specialties to have to manage patients with SLE due to the lack of rheumatologists in the health institutions. It is important to stress that patients with SLE should always be treated by rheumatologists, but, where this option does not exist, this guideline can provide useful evidence-based information and serve as support in decision-making in the treatment of these patients. This guideline presents recommendations on the management of general, articular, renal, cardiovascular, pulmonary, neurological, haematological and gastrointestinal manifestations.
MethodologyThe rheumatologists who formed the panel of experts drawing up this CPG were chosen by the governing board of the MCR based on their expertise in the treatment of lupus. Senior rheumatologists from various states of the Mexican Republic were included, and young rheumatologists who had shown great interest in participating in the academic activities of the MCR were invited to form part of the teams.
The panel of experts met for the first time in Mexico City in December 2016 to draft this document. The working groups were formed during this meeting, and the methodology outlined for the preparation of this document. After this meeting, there were 2 face-to-face meetings to check that the proposed methodology was being followed, and the findings from the literature were presented by each of the teams. In addition, there was constant electronic communication. The teams, after presenting their results to the other panellists, prepared their recommendations and sent them to the methodologist coordinating the work, who in turn drafted a document with all the recommendations. This document was submitted electronically to all the panellists for their consideration, and the final recommendations were chosen by consensus: there was no disagreement between the team members.
The author responsible for publication submitted the subjects that the guideline needed to cover to the Research Committee, and together they made the final decision to produce recommendations per type of manifestation, and include recommendations on general management.
Literature SearchFor the literature search, a series of research questions were generated for the general management of the disease, and for each of its manifestations. Each research question resulted in one or more than one search, depending on its complexity. The PICO methodology was used, for searches clearly identifying the population (P), intervention (I), comparator (C), and outcome (O). In sum, the target population were patients with SLE, the interventions and comparators were all the treatments presented in this document, and there were multiple outcomes. Not only were the most clinically relevant outcomes considered, such as prevention of renal damage or reducing progression of the disease, remission after induction, prevention of relapse, the control or reduction of the manifestations of the disease, but also those relevant to the patients, such as fatigue and pain reduction. The searches were performed from 2000 to 2016, they were limited to adults and, given the limited scientific literature, the search was not restricted to publications on Mexican populations, although the articles that did cover this population bore more weight when making the recommendations. Given the absence of direct evidence, most of the recommendations were made based on the results from other populations.
Each team received from the methodologist the PICO search mechanisms for the subject that they had been allocated. Each team reviewed the articles and, based on the review of related articles and the references cited in the publications of interest, completed their search. The team members checked that the articles that were to be used to make the recommendations answered the research questions, and met the selection criteria that had been determined beforehand by the governing board of the MCR. Any disagreements among the teams were resolved through discussion between team members. Once all the scientific literature had been reviewed, the recommendations were drafted. Unlike most Mexican CPG that use the levels of evidence of Shekelle et al.,15 the GRADE16 system was used to draw up the recommendations of this CPG, and rate the level of evidence and strength of the recommendations. This is the system currently recommended by the same authors who developed the levels of evidence used in previous years in the new guideline for drawing up CPG.17 The GRADE method has proved superior to other systems for evaluating CPG18 recommendations, and has now been adopted by the Cochrane Collaboration.
Quality of the EvidenceThe quality of the body of the evidence used to make the recommendations was classified as very low, low, moderate and high, depending on its characteristics. Expert opinion was not considered evidence; therefore it was classified as very low quality of evidence. A classification of high quality means that further research is very unlikely to change confidence in the estimate of effect, moderate quality means that that further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate; low quality means that further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate and, finally, very low quality means that any estimate of effect is very uncertain.19
Strong or Weak Recommendation or Good Practice RecommendationOnce the quality of the evidence had been assessed, the recommendations were determined as either strong or weak. It is said that when a strong recommendation is made, the desirable consequences of the intervention clearly outweigh the undesirable consequences; by contrast, with weak recommendations it is uncertain whether the desirable consequences substantially outweigh the undesirable consequences or are similar.19 The recommendations that were considered important but that could not be rated in terms of quality of evidence or strength of recommendation were classified as “good practice”.20
Results and DiscussionTreatment of Systemic Lupus ErythematosusThere is no general treatment for SLE because of the heterogeneity of its behaviour, and its management must be individualised based on patient features and the activity of the disease, and even with the possibility of access to certain drugs, such as the biological therapies. Treatment is based on the use of glucocorticoids (GC), nonsteroidal anti-inflammatory drugs (NSAIDs), antimalarials and various immunosuppressants. The prognosis of these patients has notably improved with these treatments, although there can be frequent relapses as well as, in some cases, therapeutic failure. The toxicity of these drugs must be monitored. The aim of treatment is to achieve remission21 (absence of perceived clinical activity) or, at least, achieve minimum disease activity22,23 for the patient enabling immunosuppressants and GC to be stopped or at least maintained at the lowest possible doses to prevent their associated adverse effects. There are patients who are refractory to treatment, do not respond to standard treatment or require an unacceptable dose of GC to maintain remission.24 Before a patient refractory is considered refractory, their adherence to the therapy should be checked, as well as any accumulated damage that is not likely to improve with treatment.25,26
For the purposes of these recommendations, severe lupus is understood to be when treatment is needed for potentially fatal manifestations such as lupus nephritis, neuropsychiatric involvement, haemolytic anaemia (Hb<7g/dL), thrombocytopenia (<30,000 platelets),27 vasculitis, pulmonary haemorrhage, myocarditis, lupus pneumonitis, severe myositis, lupus enteritis, lupus pancreatitis, lupus hepatitis, protein-losing enteropathy, severe keratitis, retinal vasculitis, severe scleritis, optic neuritis. Non-severe lupus is understood as the involvement of a minor organ (mucocutaneous, articular, serous lupus), and when the manifestations of the disease do not warrant treatment.28
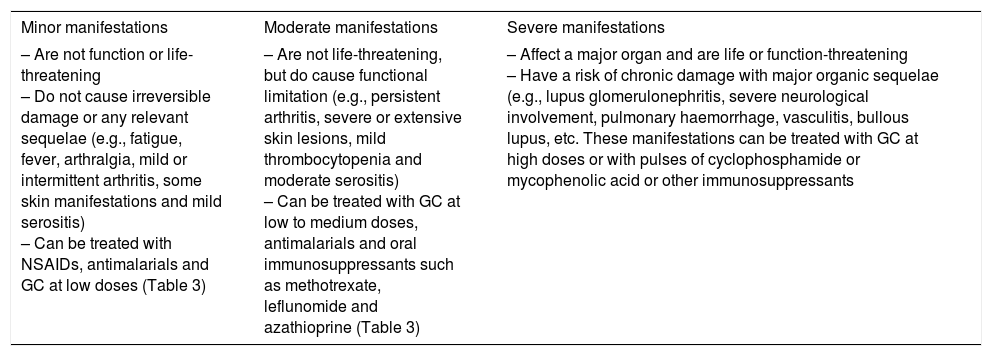
As we have already mentioned, treatment of SLE must be individual and will depend on the type of manifestation, the organ/s or system/s involved, and the severity of the disease.26 Classification of the manifestations according to severity are given in Table 1.
Classification of Clinical Manifestations in SLE Based on Their Impact on Patients.25,26
| Minor manifestations | Moderate manifestations | Severe manifestations |
|---|---|---|
| – Are not function or life-threatening – Do not cause irreversible damage or any relevant sequelae (e.g., fatigue, fever, arthralgia, mild or intermittent arthritis, some skin manifestations and mild serositis) – Can be treated with NSAIDs, antimalarials and GC at low doses (Table 3) | – Are not life-threatening, but do cause functional limitation (e.g., persistent arthritis, severe or extensive skin lesions, mild thrombocytopenia and moderate serositis) – Can be treated with GC at low to medium doses, antimalarials and oral immunosuppressants such as methotrexate, leflunomide and azathioprine (Table 3) | – Affect a major organ and are life or function-threatening – Have a risk of chronic damage with major organic sequelae (e.g., lupus glomerulonephritis, severe neurological involvement, pulmonary haemorrhage, vasculitis, bullous lupus, etc. These manifestations can be treated with GC at high doses or with pulses of cyclophosphamide or mycophenolic acid or other immunosuppressants |
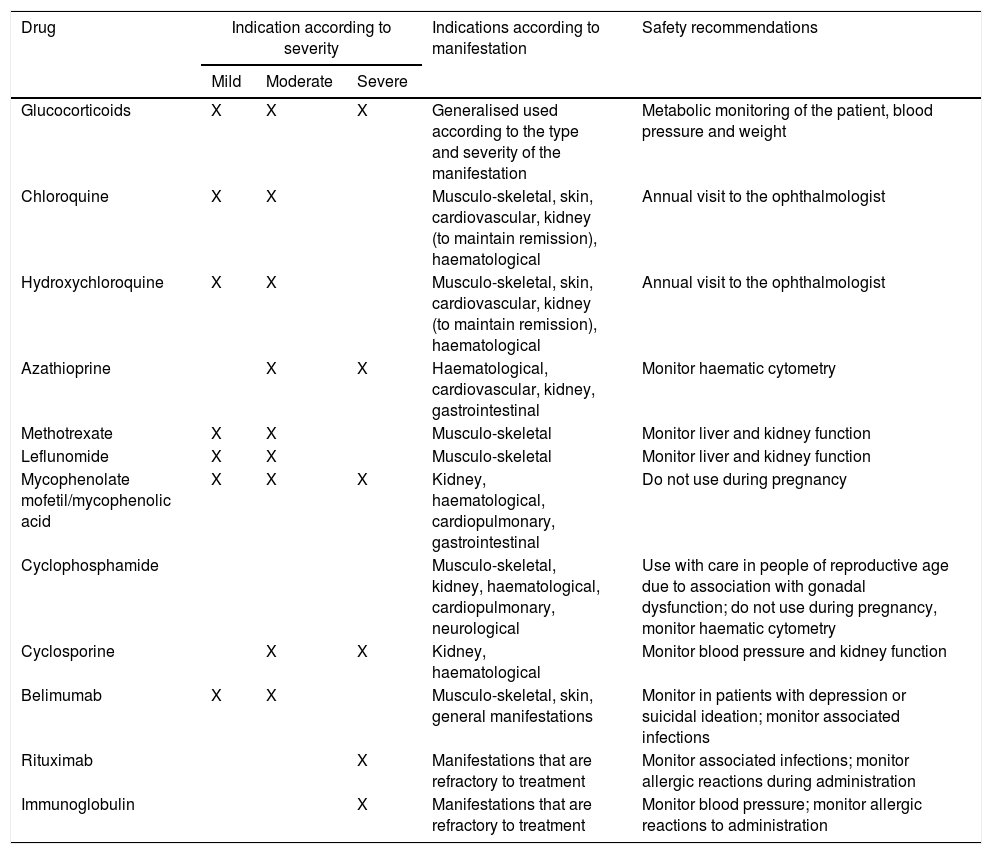
The evidence-based recommendations for each type of manifestation that form part of this CPG for the management of SLE are found in the tables of recommendations for each manifestation. In addition, the section below and Table 2 present some generalities regarding the drug groups most used in the treatment of SLE.
General Considerations on the Use of Drugs for the Treatment of SLE.
| Drug | Indication according to severity | Indications according to manifestation | Safety recommendations | ||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||
| Glucocorticoids | X | X | X | Generalised used according to the type and severity of the manifestation | Metabolic monitoring of the patient, blood pressure and weight |
| Chloroquine | X | X | Musculo-skeletal, skin, cardiovascular, kidney (to maintain remission), haematological | Annual visit to the ophthalmologist | |
| Hydroxychloroquine | X | X | Musculo-skeletal, skin, cardiovascular, kidney (to maintain remission), haematological | Annual visit to the ophthalmologist | |
| Azathioprine | X | X | Haematological, cardiovascular, kidney, gastrointestinal | Monitor haematic cytometry | |
| Methotrexate | X | X | Musculo-skeletal | Monitor liver and kidney function | |
| Leflunomide | X | X | Musculo-skeletal | Monitor liver and kidney function | |
| Mycophenolate mofetil/mycophenolic acid | X | X | X | Kidney, haematological, cardiopulmonary, gastrointestinal | Do not use during pregnancy |
| Cyclophosphamide | Musculo-skeletal, kidney, haematological, cardiopulmonary, neurological | Use with care in people of reproductive age due to association with gonadal dysfunction; do not use during pregnancy, monitor haematic cytometry | |||
| Cyclosporine | X | X | Kidney, haematological | Monitor blood pressure and kidney function | |
| Belimumab | X | X | Musculo-skeletal, skin, general manifestations | Monitor in patients with depression or suicidal ideation; monitor associated infections | |
| Rituximab | X | Manifestations that are refractory to treatment | Monitor associated infections; monitor allergic reactions during administration | ||
| Immunoglobulin | X | Manifestations that are refractory to treatment | Monitor blood pressure; monitor allergic reactions to administration | ||
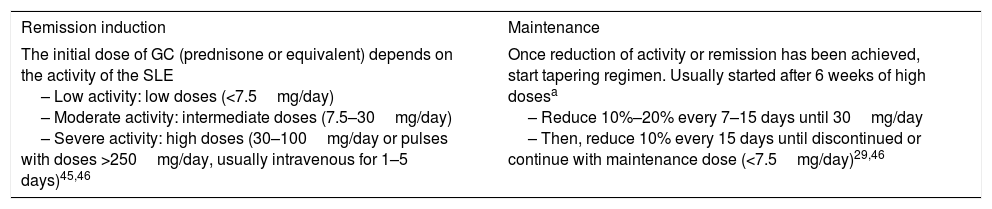
GC are the cornerstone of treatment for SLE. It is common for GC pulses to be administered that, for the purposes of this document and unless otherwise specified, will be defined as the intravenous administration of high doses of steroids. Generally 1g of methylprednisolone succinate is administered over a period of 2h; an average of 3 pulses is given, one per day, for 3 consecutive days. Although there is no consensus on standardised recommendations, comorbidities and risk factors for adverse advents should be assessed in patients treated with GC, and treated if appropriate. During treatment the patient's body weight, blood pressure, peripheral oedema, heart failure, serum lipids and glucose must be monitored, and they must undergo an ophthalmological assessment. If the patient has a dose >75mg/day of prednisone and requires treatment for more than 3 months, a calcium and vitamin D supplement should be started. The use of antiresorptive agents must be assessed based on the patient's risk factors.29 Considerations on their use in the remission induction and maintenance schemes are shown in Table 3.
Considerations on the Use of Glucocorticoids in the Remission Induction and Maintenance Regimen for SLE.
| Remission induction | Maintenance |
|---|---|
| The initial dose of GC (prednisone or equivalent) depends on the activity of the SLE – Low activity: low doses (<7.5mg/day) – Moderate activity: intermediate doses (7.5–30mg/day) – Severe activity: high doses (30–100mg/day or pulses with doses >250mg/day, usually intravenous for 1–5 days)45,46 | Once reduction of activity or remission has been achieved, start tapering regimen. Usually started after 6 weeks of high dosesa – Reduce 10%–20% every 7–15 days until 30mg/day – Then, reduce 10% every 15 days until discontinued or continue with maintenance dose (<7.5mg/day)29,46 |
Antimalarials have been used in the treatment of SLE since the nineteenth century and, although there are few studies that aim to demonstrate their efficacy, the current evidence suggests the use of hydroxychloroquine (HCQ) (at 20–400mg/day) or chloroquine (at 150–300mg/day). There is no evidence that higher doses are more effective than low doses, and the appropriate dose must be left to the judgement of the clinician. Antimalarials have photoprotective, lipid lowering, antiangiogenic, antithrombotic effects, and also inhibit the function of the B cell-activating factor and phospholipase A2-activating factor, which means that they are indicated in the treatment of skin lupus, of SLE with mild to moderate activity, as concomitant treatment to prevent relapses and damage to major organs.30 Provided there are no contradictions, antimalarials are recommended for all patients with SLE. HCQ is associated with longer damage-free survival than when it is not used (45.1% vs 26.5%; P<.001), and correlates negatively with accumulated damage measured by SLICC (r=−.22; P=.015),31 reducing the probability of accumulated renal damage (HR .68; 95% CI: .53–.93)32 (OR .38; 95% CI: .25–.58)33 in those who use them compared to those who do not. They are also useful in the prevention of morbidity due to atherosclerosis, and in the management of antiphospholipid antibody syndrome associated with SLE.34,35 Discontinuing HCQ has been reported to increase the relative risk of relapse by 2.5 (95% CI: 1.08–5.58) over a period of 6 months.36 A baseline and subsequent annual ophthalmological assessment should be performed to monitor adverse events.
Non-steroidal Anti-inflammatory DrugsNSAIDs are recommended in rheumatic diseases for treating pain and inflammation. The consensus on the use of NSAIDs of the Spanish Rheumatology Society and the MCR recommends individualising their use based on each patient's variability of response, gastrointestinal toxicity, cardiovascular, renal and hepatic risk factors. One NSAID cannot be considered better than another (traditional or COXIBS). Simultaneous use of more than one NSAID must be avoided, since this only increases toxicity, and does not increase efficacy (ceiling effect). In acute processes, they should be used for the shortest possible time at the maximum recommended dose, and in chronic processes, the minimum dose necessary to maintain the desired clinical response should be used. Risk factors, adverse effects and indication for use should be assessed periodically. Concomitant use with GC increases gastrointestinal toxicity. Interactions with other drugs such as antihypertensives, glucose-lowering drugs, oral anticoagulants, etc. should be assessed.37
ImmunosuppressantsMost rheumatologists agree on the use of immunomodulators for moderate to severe SLE during an intense period of immunosuppression known as induction therapy, followed by a longer period of maintenance therapy. The three main objectives of induction therapy are to halt damage, recover function, and control immunological activity. Maintenance therapy is used to consolidate remission and prevent relapse with a treatment programme with a low risk of complications and more convenient for the patient, under the current concept of “personalised treatment”. The drugs that are traditionally used with these aims are the following:
- –
Mycophenolic acid (MMF): the dose varies widely depending on the organ involved and the severity of the manifestation; it can range from 1 to 3g. Adverse events that must be monitored are cytopenia, altered LFT, diarrhoea and teratogenicity.38–41
- –
Cyclophosphamide (CYC): the dose can vary from 500 to 1000mg/m2 of body surface area. Adverse events that must be monitored are cytopenia, teratogenicity, infertility, myeloproliferative disorders, haemorrhagic cystitis, and bladder cancer.40
- –
Azathioprine: the dose varies between 1 and 3mg/kg/day and the adverse events to be monitored are myelosuppression, hepatotoxicity, lymphoproliferative disorders and teratogenicity.41,42
- –
Methotrexate: can be used in doses from 7.5 to 25mg, orally or parenterally, and the adverse events to be monitored are myelosuppression, hepatotoxicity, pneumonitis, alopecia, stomatitis, and teratogenicity.39–42
- –
Cyclosporine: principally used in resistant nephropathy, and the main adverse events are gingival hyperplasia, high blood pressure, hirsutism, renal failure, and anaemia.43
Other drugs used in SLE are the biologics belimumab and rituximab. Belimumab is used in mild to moderate manifestations such as arthritis, serositis or if there is a skin infection (dsDNA+ or C3/C4 consumption). B-lymphocyte depletion is the most common adverse event with this biologic. Rituximab is also used when there is joint involvement resistant to conventional treatment, haematological involvement, involvement of the central nervous system or resistant nephritis, and the principal adverse events are allergy, serum sickness, and progressive multifocal leukoencephalopathy.44
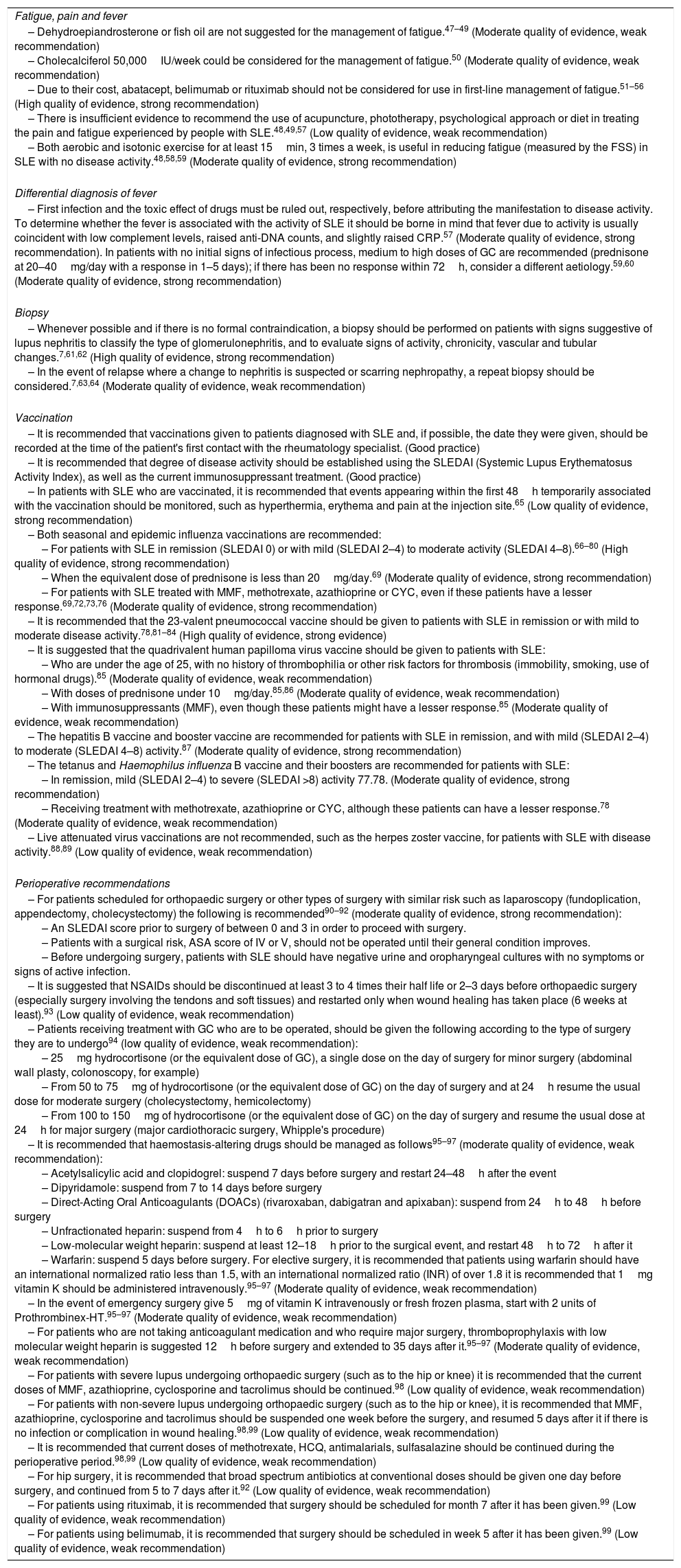
Recommendations Based on the Review of the Scientific EvidenceThe tables below show the recommendations resulting from the literature review and the work by consensus of the participants in the working group who are the signatories of this CPG. Table 4 presents the recommendations for managing the general manifestations of SLE, and Tables 5–10 present the recommendations for the treatment of the renal, cardiovascular, pulmonary, neurological, haematological, and gastrointestinal manifestations of the disease.
Recommendations for the Management of the General Manifestations of SLE.
| Fatigue, pain and fever |
| – Dehydroepiandrosterone or fish oil are not suggested for the management of fatigue.47–49 (Moderate quality of evidence, weak recommendation) – Cholecalciferol 50,000IU/week could be considered for the management of fatigue.50 (Moderate quality of evidence, weak recommendation) – Due to their cost, abatacept, belimumab or rituximab should not be considered for use in first-line management of fatigue.51–56 (High quality of evidence, strong recommendation) – There is insufficient evidence to recommend the use of acupuncture, phototherapy, psychological approach or diet in treating the pain and fatigue experienced by people with SLE.48,49,57 (Low quality of evidence, weak recommendation) – Both aerobic and isotonic exercise for at least 15min, 3 times a week, is useful in reducing fatigue (measured by the FSS) in SLE with no disease activity.48,58,59 (Moderate quality of evidence, strong recommendation) |
| Differential diagnosis of fever |
| – First infection and the toxic effect of drugs must be ruled out, respectively, before attributing the manifestation to disease activity. To determine whether the fever is associated with the activity of SLE it should be borne in mind that fever due to activity is usually coincident with low complement levels, raised anti-DNA counts, and slightly raised CRP.57 (Moderate quality of evidence, strong recommendation). In patients with no initial signs of infectious process, medium to high doses of GC are recommended (prednisone at 20–40mg/day with a response in 1–5 days); if there has been no response within 72h, consider a different aetiology.59,60 (Moderate quality of evidence, strong recommendation) |
| Biopsy |
| – Whenever possible and if there is no formal contraindication, a biopsy should be performed on patients with signs suggestive of lupus nephritis to classify the type of glomerulonephritis, and to evaluate signs of activity, chronicity, vascular and tubular changes.7,61,62 (High quality of evidence, strong recommendation) – In the event of relapse where a change to nephritis is suspected or scarring nephropathy, a repeat biopsy should be considered.7,63,64 (Moderate quality of evidence, weak recommendation) |
| Vaccination |
| – It is recommended that vaccinations given to patients diagnosed with SLE and, if possible, the date they were given, should be recorded at the time of the patient's first contact with the rheumatology specialist. (Good practice) – It is recommended that degree of disease activity should be established using the SLEDAI (Systemic Lupus Erythematosus Activity Index), as well as the current immunosuppressant treatment. (Good practice) – In patients with SLE who are vaccinated, it is recommended that events appearing within the first 48h temporarily associated with the vaccination should be monitored, such as hyperthermia, erythema and pain at the injection site.65 (Low quality of evidence, strong recommendation) – Both seasonal and epidemic influenza vaccinations are recommended: – For patients with SLE in remission (SLEDAI 0) or with mild (SLEDAI 2–4) to moderate activity (SLEDAI 4–8).66–80 (High quality of evidence, strong recommendation) – When the equivalent dose of prednisone is less than 20mg/day.69 (Moderate quality of evidence, strong recommendation) – For patients with SLE treated with MMF, methotrexate, azathioprine or CYC, even if these patients have a lesser response.69,72,73,76 (Moderate quality of evidence, strong recommendation) – It is recommended that the 23-valent pneumococcal vaccine should be given to patients with SLE in remission or with mild to moderate disease activity.78,81–84 (High quality of evidence, strong evidence) – It is suggested that the quadrivalent human papilloma virus vaccine should be given to patients with SLE: – Who are under the age of 25, with no history of thrombophilia or other risk factors for thrombosis (immobility, smoking, use of hormonal drugs).85 (Moderate quality of evidence, weak recommendation) – With doses of prednisone under 10mg/day.85,86 (Moderate quality of evidence, weak recommendation) – With immunosuppressants (MMF), even though these patients might have a lesser response.85 (Moderate quality of evidence, weak recommendation) – The hepatitis B vaccine and booster vaccine are recommended for patients with SLE in remission, and with mild (SLEDAI 2–4) to moderate (SLEDAI 4–8) activity.87 (Moderate quality of evidence, strong recommendation) – The tetanus and Haemophilus influenza B vaccine and their boosters are recommended for patients with SLE: – In remission, mild (SLEDAI 2–4) to severe (SLEDAI >8) activity 77.78. (Moderate quality of evidence, strong recommendation) – Receiving treatment with methotrexate, azathioprine or CYC, although these patients can have a lesser response.78 (Moderate quality of evidence, weak recommendation) – Live attenuated virus vaccinations are not recommended, such as the herpes zoster vaccine, for patients with SLE with disease activity.88,89 (Low quality of evidence, weak recommendation) |
| Perioperative recommendations |
| – For patients scheduled for orthopaedic surgery or other types of surgery with similar risk such as laparoscopy (fundoplication, appendectomy, cholecystectomy) the following is recommended90–92 (moderate quality of evidence, strong recommendation): – An SLEDAI score prior to surgery of between 0 and 3 in order to proceed with surgery. – Patients with a surgical risk, ASA score of IV or V, should not be operated until their general condition improves. – Before undergoing surgery, patients with SLE should have negative urine and oropharyngeal cultures with no symptoms or signs of active infection. – It is suggested that NSAIDs should be discontinued at least 3 to 4 times their half life or 2–3 days before orthopaedic surgery (especially surgery involving the tendons and soft tissues) and restarted only when wound healing has taken place (6 weeks at least).93 (Low quality of evidence, weak recommendation) – Patients receiving treatment with GC who are to be operated, should be given the following according to the type of surgery they are to undergo94 (low quality of evidence, weak recommendation): – 25mg hydrocortisone (or the equivalent dose of GC), a single dose on the day of surgery for minor surgery (abdominal wall plasty, colonoscopy, for example) – From 50 to 75mg of hydrocortisone (or the equivalent dose of GC) on the day of surgery and at 24h resume the usual dose for moderate surgery (cholecystectomy, hemicolectomy) – From 100 to 150mg of hydrocortisone (or the equivalent dose of GC) on the day of surgery and resume the usual dose at 24h for major surgery (major cardiothoracic surgery, Whipple's procedure) – It is recommended that haemostasis-altering drugs should be managed as follows95–97 (moderate quality of evidence, weak recommendation): – Acetylsalicylic acid and clopidogrel: suspend 7 days before surgery and restart 24–48h after the event – Dipyridamole: suspend from 7 to 14 days before surgery – Direct-Acting Oral Anticoagulants (DOACs) (rivaroxaban, dabigatran and apixaban): suspend from 24h to 48h before surgery – Unfractionated heparin: suspend from 4h to 6h prior to surgery – Low-molecular weight heparin: suspend at least 12–18h prior to the surgical event, and restart 48h to 72h after it – Warfarin: suspend 5 days before surgery. For elective surgery, it is recommended that patients using warfarin should have an international normalized ratio less than 1.5, with an international normalized ratio (INR) of over 1.8 it is recommended that 1mg vitamin K should be administered intravenously.95–97 (Moderate quality of evidence, weak recommendation) – In the event of emergency surgery give 5mg of vitamin K intravenously or fresh frozen plasma, start with 2 units of Prothrombinex-HT.95–97 (Moderate quality of evidence, weak recommendation) – For patients who are not taking anticoagulant medication and who require major surgery, thromboprophylaxis with low molecular weight heparin is suggested 12h before surgery and extended to 35 days after it.95–97 (Moderate quality of evidence, weak recommendation) – For patients with severe lupus undergoing orthopaedic surgery (such as to the hip or knee) it is recommended that the current doses of MMF, azathioprine, cyclosporine and tacrolimus should be continued.98 (Low quality of evidence, weak recommendation) – For patients with non-severe lupus undergoing orthopaedic surgery (such as to the hip or knee), it is recommended that MMF, azathioprine, cyclosporine and tacrolimus should be suspended one week before the surgery, and resumed 5 days after it if there is no infection or complication in wound healing.98,99 (Low quality of evidence, weak recommendation) – It is recommended that current doses of methotrexate, HCQ, antimalarials, sulfasalazine should be continued during the perioperative period.98,99 (Low quality of evidence, weak recommendation) – For hip surgery, it is recommended that broad spectrum antibiotics at conventional doses should be given one day before surgery, and continued from 5 to 7 days after it.92 (Low quality of evidence, weak recommendation) – For patients using rituximab, it is recommended that surgery should be scheduled for month 7 after it has been given.99 (Low quality of evidence, weak recommendation) – For patients using belimumab, it is recommended that surgery should be scheduled in week 5 after it has been given.99 (Low quality of evidence, weak recommendation) |
Recommendations for Renal Manifestations.
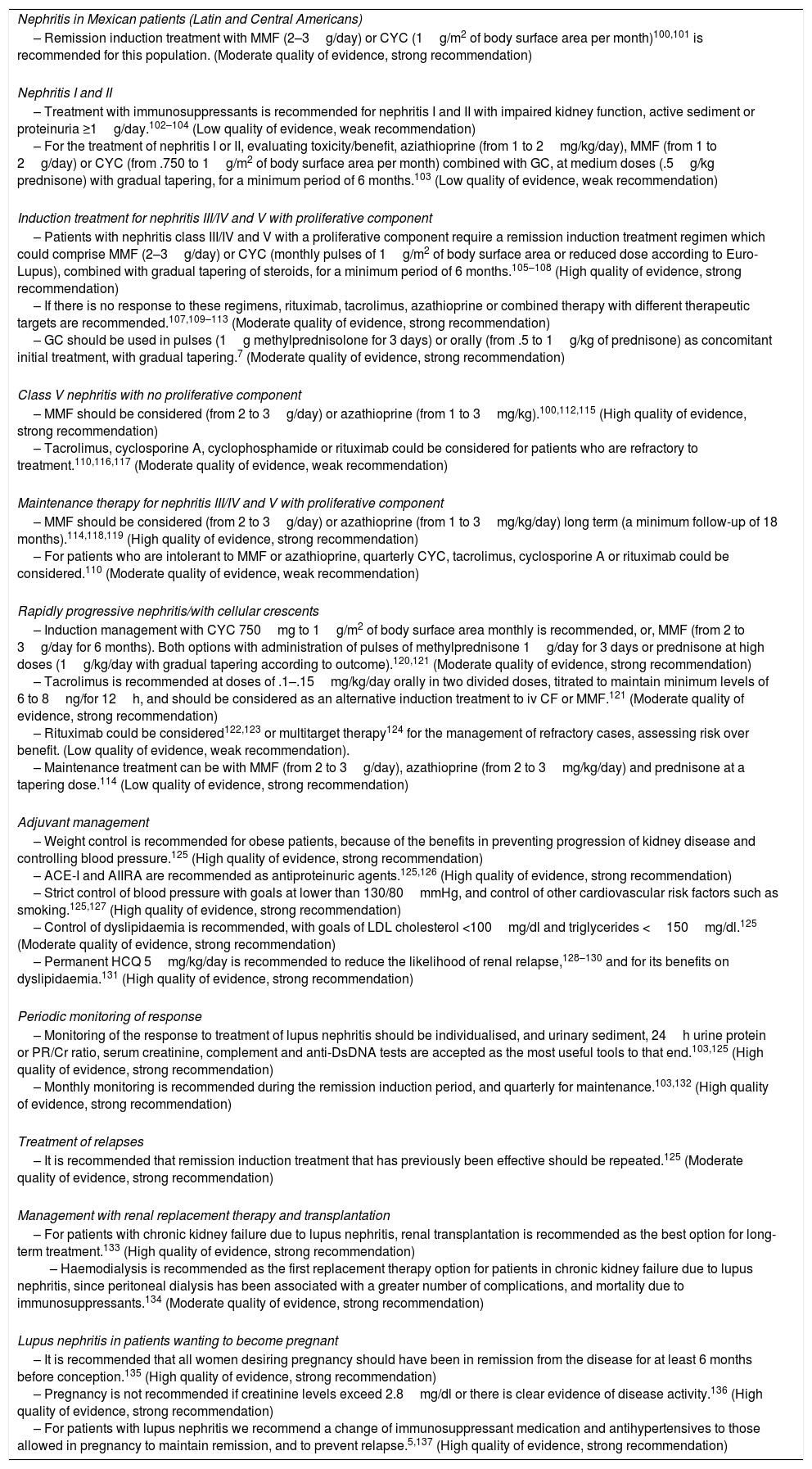
| Nephritis in Mexican patients (Latin and Central Americans) |
| – Remission induction treatment with MMF (2–3g/day) or CYC (1g/m2 of body surface area per month)100,101 is recommended for this population. (Moderate quality of evidence, strong recommendation) |
| Nephritis I and II |
| – Treatment with immunosuppressants is recommended for nephritis I and II with impaired kidney function, active sediment or proteinuria ≥1g/day.102–104 (Low quality of evidence, weak recommendation) – For the treatment of nephritis I or II, evaluating toxicity/benefit, aziathioprine (from 1 to 2mg/kg/day), MMF (from 1 to 2g/day) or CYC (from .750 to 1g/m2 of body surface area per month) combined with GC, at medium doses (.5g/kg prednisone) with gradual tapering, for a minimum period of 6 months.103 (Low quality of evidence, weak recommendation) |
| Induction treatment for nephritis III/IV and V with proliferative component |
| – Patients with nephritis class III/IV and V with a proliferative component require a remission induction treatment regimen which could comprise MMF (2–3g/day) or CYC (monthly pulses of 1g/m2 of body surface area or reduced dose according to Euro-Lupus), combined with gradual tapering of steroids, for a minimum period of 6 months.105–108 (High quality of evidence, strong recommendation) – If there is no response to these regimens, rituximab, tacrolimus, azathioprine or combined therapy with different therapeutic targets are recommended.107,109–113 (Moderate quality of evidence, strong recommendation) – GC should be used in pulses (1g methylprednisolone for 3 days) or orally (from .5 to 1g/kg of prednisone) as concomitant initial treatment, with gradual tapering.7 (Moderate quality of evidence, strong recommendation) |
| Class V nephritis with no proliferative component |
| – MMF should be considered (from 2 to 3g/day) or azathioprine (from 1 to 3mg/kg).100,112,115 (High quality of evidence, strong recommendation) – Tacrolimus, cyclosporine A, cyclophosphamide or rituximab could be considered for patients who are refractory to treatment.110,116,117 (Moderate quality of evidence, weak recommendation) |
| Maintenance therapy for nephritis III/IV and V with proliferative component |
| – MMF should be considered (from 2 to 3g/day) or azathioprine (from 1 to 3mg/kg/day) long term (a minimum follow-up of 18 months).114,118,119 (High quality of evidence, strong recommendation) – For patients who are intolerant to MMF or azathioprine, quarterly CYC, tacrolimus, cyclosporine A or rituximab could be considered.110 (Moderate quality of evidence, weak recommendation) |
| Rapidly progressive nephritis/with cellular crescents |
| – Induction management with CYC 750mg to 1g/m2 of body surface area monthly is recommended, or, MMF (from 2 to 3g/day for 6 months). Both options with administration of pulses of methylprednisone 1g/day for 3 days or prednisone at high doses (1g/kg/day with gradual tapering according to outcome).120,121 (Moderate quality of evidence, strong recommendation) – Tacrolimus is recommended at doses of .1–.15mg/kg/day orally in two divided doses, titrated to maintain minimum levels of 6 to 8ng/for 12h, and should be considered as an alternative induction treatment to iv CF or MMF.121 (Moderate quality of evidence, strong recommendation) – Rituximab could be considered122,123 or multitarget therapy124 for the management of refractory cases, assessing risk over benefit. (Low quality of evidence, weak recommendation). – Maintenance treatment can be with MMF (from 2 to 3g/day), azathioprine (from 2 to 3mg/kg/day) and prednisone at a tapering dose.114 (Low quality of evidence, strong recommendation) |
| Adjuvant management |
| – Weight control is recommended for obese patients, because of the benefits in preventing progression of kidney disease and controlling blood pressure.125 (High quality of evidence, strong recommendation) – ACE-I and AIIRA are recommended as antiproteinuric agents.125,126 (High quality of evidence, strong recommendation) – Strict control of blood pressure with goals at lower than 130/80mmHg, and control of other cardiovascular risk factors such as smoking.125,127 (High quality of evidence, strong recommendation) – Control of dyslipidaemia is recommended, with goals of LDL cholesterol <100mg/dl and triglycerides <150mg/dl.125 (Moderate quality of evidence, strong recommendation) – Permanent HCQ 5mg/kg/day is recommended to reduce the likelihood of renal relapse,128–130 and for its benefits on dyslipidaemia.131 (High quality of evidence, strong recommendation) |
| Periodic monitoring of response |
| – Monitoring of the response to treatment of lupus nephritis should be individualised, and urinary sediment, 24h urine protein or PR/Cr ratio, serum creatinine, complement and anti-DsDNA tests are accepted as the most useful tools to that end.103,125 (High quality of evidence, strong recommendation) – Monthly monitoring is recommended during the remission induction period, and quarterly for maintenance.103,132 (High quality of evidence, strong recommendation) |
| Treatment of relapses |
| – It is recommended that remission induction treatment that has previously been effective should be repeated.125 (Moderate quality of evidence, strong recommendation) |
| Management with renal replacement therapy and transplantation |
| – For patients with chronic kidney failure due to lupus nephritis, renal transplantation is recommended as the best option for long-term treatment.133 (High quality of evidence, strong recommendation) – Haemodialysis is recommended as the first replacement therapy option for patients in chronic kidney failure due to lupus nephritis, since peritoneal dialysis has been associated with a greater number of complications, and mortality due to immunosuppressants.134 (Moderate quality of evidence, strong recommendation) |
| Lupus nephritis in patients wanting to become pregnant |
| – It is recommended that all women desiring pregnancy should have been in remission from the disease for at least 6 months before conception.135 (High quality of evidence, strong recommendation) – Pregnancy is not recommended if creatinine levels exceed 2.8mg/dl or there is clear evidence of disease activity.136 (High quality of evidence, strong recommendation) – For patients with lupus nephritis we recommend a change of immunosuppressant medication and antihypertensives to those allowed in pregnancy to maintain remission, and to prevent relapse.5,137 (High quality of evidence, strong recommendation) |
Recommendations for Cardiovascular Manifestations.
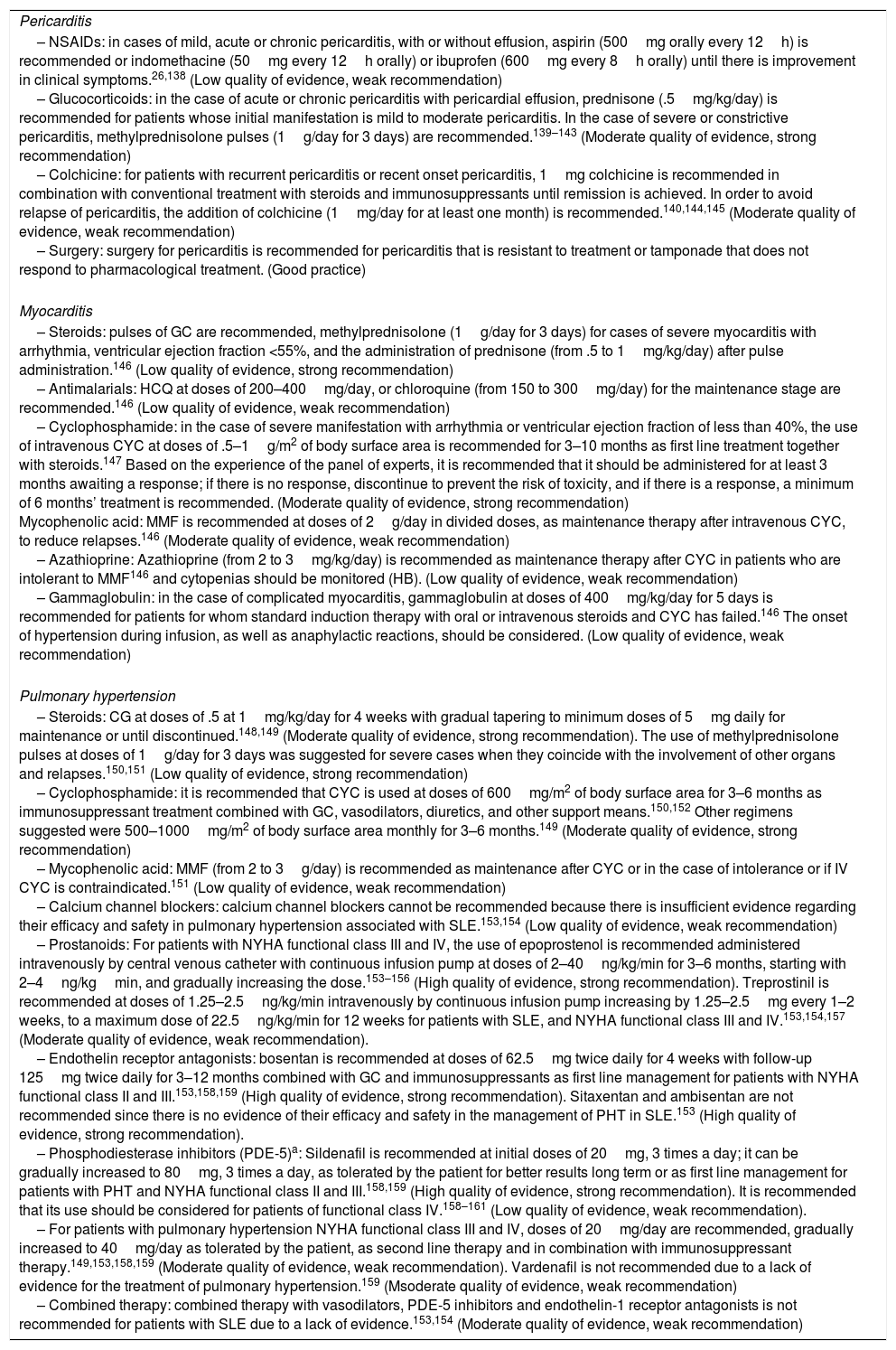
| Pericarditis |
| – NSAIDs: in cases of mild, acute or chronic pericarditis, with or without effusion, aspirin (500mg orally every 12h) is recommended or indomethacine (50mg every 12h orally) or ibuprofen (600mg every 8h orally) until there is improvement in clinical symptoms.26,138 (Low quality of evidence, weak recommendation) – Glucocorticoids: in the case of acute or chronic pericarditis with pericardial effusion, prednisone (.5mg/kg/day) is recommended for patients whose initial manifestation is mild to moderate pericarditis. In the case of severe or constrictive pericarditis, methylprednisolone pulses (1g/day for 3 days) are recommended.139–143 (Moderate quality of evidence, strong recommendation) – Colchicine: for patients with recurrent pericarditis or recent onset pericarditis, 1mg colchicine is recommended in combination with conventional treatment with steroids and immunosuppressants until remission is achieved. In order to avoid relapse of pericarditis, the addition of colchicine (1mg/day for at least one month) is recommended.140,144,145 (Moderate quality of evidence, weak recommendation) – Surgery: surgery for pericarditis is recommended for pericarditis that is resistant to treatment or tamponade that does not respond to pharmacological treatment. (Good practice) |
| Myocarditis |
| – Steroids: pulses of GC are recommended, methylprednisolone (1g/day for 3 days) for cases of severe myocarditis with arrhythmia, ventricular ejection fraction <55%, and the administration of prednisone (from .5 to 1mg/kg/day) after pulse administration.146 (Low quality of evidence, strong recommendation) – Antimalarials: HCQ at doses of 200–400mg/day, or chloroquine (from 150 to 300mg/day) for the maintenance stage are recommended.146 (Low quality of evidence, weak recommendation) – Cyclophosphamide: in the case of severe manifestation with arrhythmia or ventricular ejection fraction of less than 40%, the use of intravenous CYC at doses of .5–1g/m2 of body surface area is recommended for 3–10 months as first line treatment together with steroids.147 Based on the experience of the panel of experts, it is recommended that it should be administered for at least 3 months awaiting a response; if there is no response, discontinue to prevent the risk of toxicity, and if there is a response, a minimum of 6 months’ treatment is recommended. (Moderate quality of evidence, strong recommendation) Mycophenolic acid: MMF is recommended at doses of 2g/day in divided doses, as maintenance therapy after intravenous CYC, to reduce relapses.146 (Moderate quality of evidence, weak recommendation) – Azathioprine: Azathioprine (from 2 to 3mg/kg/day) is recommended as maintenance therapy after CYC in patients who are intolerant to MMF146 and cytopenias should be monitored (HB). (Low quality of evidence, weak recommendation) – Gammaglobulin: in the case of complicated myocarditis, gammaglobulin at doses of 400mg/kg/day for 5 days is recommended for patients for whom standard induction therapy with oral or intravenous steroids and CYC has failed.146 The onset of hypertension during infusion, as well as anaphylactic reactions, should be considered. (Low quality of evidence, weak recommendation) |
| Pulmonary hypertension |
| – Steroids: CG at doses of .5 at 1mg/kg/day for 4 weeks with gradual tapering to minimum doses of 5mg daily for maintenance or until discontinued.148,149 (Moderate quality of evidence, strong recommendation). The use of methylprednisolone pulses at doses of 1g/day for 3 days was suggested for severe cases when they coincide with the involvement of other organs and relapses.150,151 (Low quality of evidence, strong recommendation) – Cyclophosphamide: it is recommended that CYC is used at doses of 600mg/m2 of body surface area for 3–6 months as immunosuppressant treatment combined with GC, vasodilators, diuretics, and other support means.150,152 Other regimens suggested were 500–1000mg/m2 of body surface area monthly for 3–6 months.149 (Moderate quality of evidence, strong recommendation) – Mycophenolic acid: MMF (from 2 to 3g/day) is recommended as maintenance after CYC or in the case of intolerance or if IV CYC is contraindicated.151 (Low quality of evidence, weak recommendation) – Calcium channel blockers: calcium channel blockers cannot be recommended because there is insufficient evidence regarding their efficacy and safety in pulmonary hypertension associated with SLE.153,154 (Low quality of evidence, weak recommendation) – Prostanoids: For patients with NYHA functional class III and IV, the use of epoprostenol is recommended administered intravenously by central venous catheter with continuous infusion pump at doses of 2–40ng/kg/min for 3–6 months, starting with 2–4ng/kgmin, and gradually increasing the dose.153–156 (High quality of evidence, strong recommendation). Treprostinil is recommended at doses of 1.25–2.5ng/kg/min intravenously by continuous infusion pump increasing by 1.25–2.5mg every 1–2 weeks, to a maximum dose of 22.5ng/kg/min for 12 weeks for patients with SLE, and NYHA functional class III and IV.153,154,157 (Moderate quality of evidence, weak recommendation). – Endothelin receptor antagonists: bosentan is recommended at doses of 62.5mg twice daily for 4 weeks with follow-up 125mg twice daily for 3–12 months combined with GC and immunosuppressants as first line management for patients with NYHA functional class II and III.153,158,159 (High quality of evidence, strong recommendation). Sitaxentan and ambisentan are not recommended since there is no evidence of their efficacy and safety in the management of PHT in SLE.153 (High quality of evidence, strong recommendation). – Phosphodiesterase inhibitors (PDE-5)a: Sildenafil is recommended at initial doses of 20mg, 3 times a day; it can be gradually increased to 80mg, 3 times a day, as tolerated by the patient for better results long term or as first line management for patients with PHT and NYHA functional class II and III.158,159 (High quality of evidence, strong recommendation). It is recommended that its use should be considered for patients of functional class IV.158–161 (Low quality of evidence, weak recommendation). – For patients with pulmonary hypertension NYHA functional class III and IV, doses of 20mg/day are recommended, gradually increased to 40mg/day as tolerated by the patient, as second line therapy and in combination with immunosuppressant therapy.149,153,158,159 (Moderate quality of evidence, weak recommendation). Vardenafil is not recommended due to a lack of evidence for the treatment of pulmonary hypertension.159 (Msoderate quality of evidence, weak recommendation) – Combined therapy: combined therapy with vasodilators, PDE-5 inhibitors and endothelin-1 receptor antagonists is not recommended for patients with SLE due to a lack of evidence.153,154 (Moderate quality of evidence, weak recommendation) |
Recommendations for Pulmonary Manifestations.
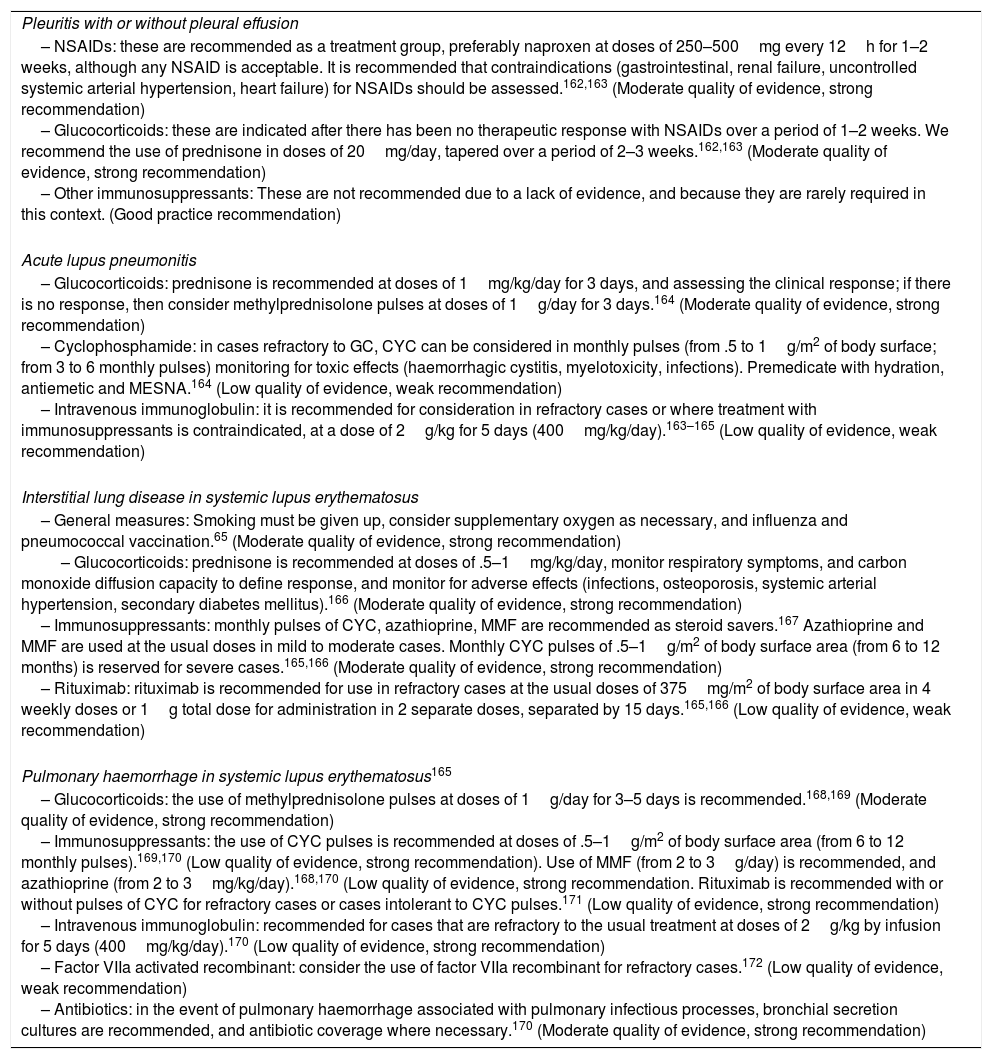
| Pleuritis with or without pleural effusion |
| – NSAIDs: these are recommended as a treatment group, preferably naproxen at doses of 250–500mg every 12h for 1–2 weeks, although any NSAID is acceptable. It is recommended that contraindications (gastrointestinal, renal failure, uncontrolled systemic arterial hypertension, heart failure) for NSAIDs should be assessed.162,163 (Moderate quality of evidence, strong recommendation) – Glucocorticoids: these are indicated after there has been no therapeutic response with NSAIDs over a period of 1–2 weeks. We recommend the use of prednisone in doses of 20mg/day, tapered over a period of 2–3 weeks.162,163 (Moderate quality of evidence, strong recommendation) – Other immunosuppressants: These are not recommended due to a lack of evidence, and because they are rarely required in this context. (Good practice recommendation) |
| Acute lupus pneumonitis |
| – Glucocorticoids: prednisone is recommended at doses of 1mg/kg/day for 3 days, and assessing the clinical response; if there is no response, then consider methylprednisolone pulses at doses of 1g/day for 3 days.164 (Moderate quality of evidence, strong recommendation) – Cyclophosphamide: in cases refractory to GC, CYC can be considered in monthly pulses (from .5 to 1g/m2 of body surface; from 3 to 6 monthly pulses) monitoring for toxic effects (haemorrhagic cystitis, myelotoxicity, infections). Premedicate with hydration, antiemetic and MESNA.164 (Low quality of evidence, weak recommendation) – Intravenous immunoglobulin: it is recommended for consideration in refractory cases or where treatment with immunosuppressants is contraindicated, at a dose of 2g/kg for 5 days (400mg/kg/day).163–165 (Low quality of evidence, weak recommendation) |
| Interstitial lung disease in systemic lupus erythematosus |
| – General measures: Smoking must be given up, consider supplementary oxygen as necessary, and influenza and pneumococcal vaccination.65 (Moderate quality of evidence, strong recommendation) – Glucocorticoids: prednisone is recommended at doses of .5–1mg/kg/day, monitor respiratory symptoms, and carbon monoxide diffusion capacity to define response, and monitor for adverse effects (infections, osteoporosis, systemic arterial hypertension, secondary diabetes mellitus).166 (Moderate quality of evidence, strong recommendation) – Immunosuppressants: monthly pulses of CYC, azathioprine, MMF are recommended as steroid savers.167 Azathioprine and MMF are used at the usual doses in mild to moderate cases. Monthly CYC pulses of .5–1g/m2 of body surface area (from 6 to 12 months) is reserved for severe cases.165,166 (Moderate quality of evidence, strong recommendation) – Rituximab: rituximab is recommended for use in refractory cases at the usual doses of 375mg/m2 of body surface area in 4 weekly doses or 1g total dose for administration in 2 separate doses, separated by 15 days.165,166 (Low quality of evidence, weak recommendation) |
| Pulmonary haemorrhage in systemic lupus erythematosus165 |
| – Glucocorticoids: the use of methylprednisolone pulses at doses of 1g/day for 3–5 days is recommended.168,169 (Moderate quality of evidence, strong recommendation) – Immunosuppressants: the use of CYC pulses is recommended at doses of .5–1g/m2 of body surface area (from 6 to 12 monthly pulses).169,170 (Low quality of evidence, strong recommendation). Use of MMF (from 2 to 3g/day) is recommended, and azathioprine (from 2 to 3mg/kg/day).168,170 (Low quality of evidence, strong recommendation. Rituximab is recommended with or without pulses of CYC for refractory cases or cases intolerant to CYC pulses.171 (Low quality of evidence, strong recommendation) – Intravenous immunoglobulin: recommended for cases that are refractory to the usual treatment at doses of 2g/kg by infusion for 5 days (400mg/kg/day).170 (Low quality of evidence, strong recommendation) – Factor VIIa activated recombinant: consider the use of factor VIIa recombinant for refractory cases.172 (Low quality of evidence, weak recommendation) – Antibiotics: in the event of pulmonary haemorrhage associated with pulmonary infectious processes, bronchial secretion cultures are recommended, and antibiotic coverage where necessary.170 (Moderate quality of evidence, strong recommendation) |
Recommendations for Neurological Manifestations.
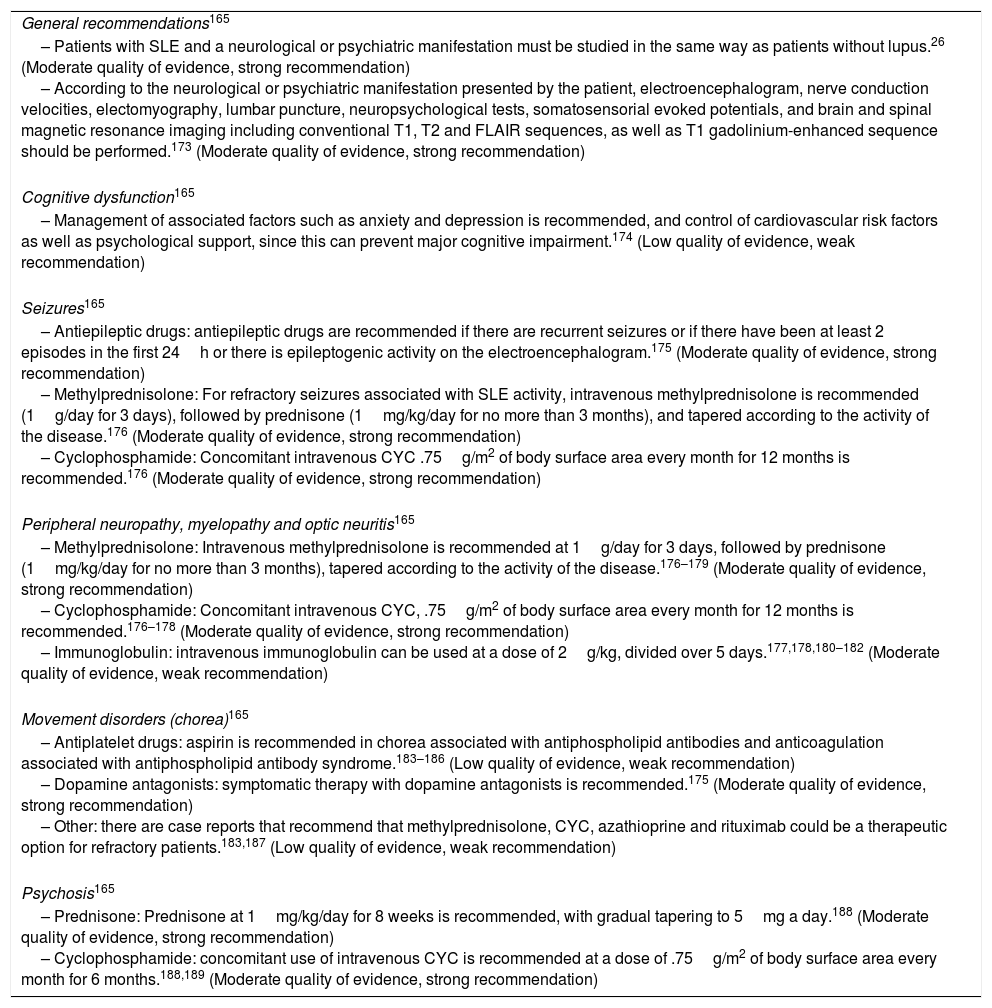
| General recommendations165 |
| – Patients with SLE and a neurological or psychiatric manifestation must be studied in the same way as patients without lupus.26 (Moderate quality of evidence, strong recommendation) – According to the neurological or psychiatric manifestation presented by the patient, electroencephalogram, nerve conduction velocities, electomyography, lumbar puncture, neuropsychological tests, somatosensorial evoked potentials, and brain and spinal magnetic resonance imaging including conventional T1, T2 and FLAIR sequences, as well as T1 gadolinium-enhanced sequence should be performed.173 (Moderate quality of evidence, strong recommendation) |
| Cognitive dysfunction165 |
| – Management of associated factors such as anxiety and depression is recommended, and control of cardiovascular risk factors as well as psychological support, since this can prevent major cognitive impairment.174 (Low quality of evidence, weak recommendation) |
| Seizures165 |
| – Antiepileptic drugs: antiepileptic drugs are recommended if there are recurrent seizures or if there have been at least 2 episodes in the first 24h or there is epileptogenic activity on the electroencephalogram.175 (Moderate quality of evidence, strong recommendation) – Methylprednisolone: For refractory seizures associated with SLE activity, intravenous methylprednisolone is recommended (1g/day for 3 days), followed by prednisone (1mg/kg/day for no more than 3 months), and tapered according to the activity of the disease.176 (Moderate quality of evidence, strong recommendation) – Cyclophosphamide: Concomitant intravenous CYC .75g/m2 of body surface area every month for 12 months is recommended.176 (Moderate quality of evidence, strong recommendation) |
| Peripheral neuropathy, myelopathy and optic neuritis165 |
| – Methylprednisolone: Intravenous methylprednisolone is recommended at 1g/day for 3 days, followed by prednisone (1mg/kg/day for no more than 3 months), tapered according to the activity of the disease.176–179 (Moderate quality of evidence, strong recommendation) – Cyclophosphamide: Concomitant intravenous CYC, .75g/m2 of body surface area every month for 12 months is recommended.176–178 (Moderate quality of evidence, strong recommendation) – Immunoglobulin: intravenous immunoglobulin can be used at a dose of 2g/kg, divided over 5 days.177,178,180–182 (Moderate quality of evidence, weak recommendation) |
| Movement disorders (chorea)165 |
| – Antiplatelet drugs: aspirin is recommended in chorea associated with antiphospholipid antibodies and anticoagulation associated with antiphospholipid antibody syndrome.183–186 (Low quality of evidence, weak recommendation) – Dopamine antagonists: symptomatic therapy with dopamine antagonists is recommended.175 (Moderate quality of evidence, strong recommendation) – Other: there are case reports that recommend that methylprednisolone, CYC, azathioprine and rituximab could be a therapeutic option for refractory patients.183,187 (Low quality of evidence, weak recommendation) |
| Psychosis165 |
| – Prednisone: Prednisone at 1mg/kg/day for 8 weeks is recommended, with gradual tapering to 5mg a day.188 (Moderate quality of evidence, strong recommendation) – Cyclophosphamide: concomitant use of intravenous CYC is recommended at a dose of .75g/m2 of body surface area every month for 6 months.188,189 (Moderate quality of evidence, strong recommendation) |
Recommendations for Haematological Manifestations.
| Thrombocytopenia |
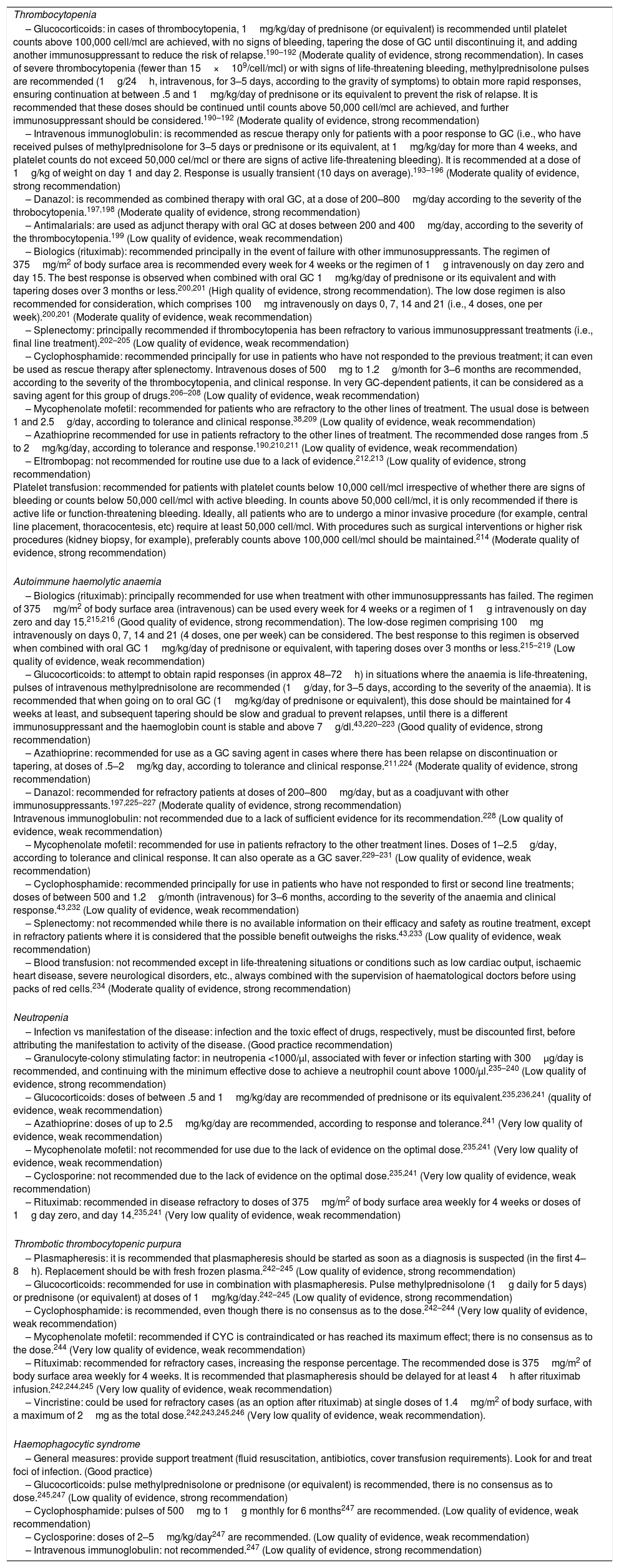
| – Glucocorticoids: in cases of thrombocytopenia, 1mg/kg/day of prednisone (or equivalent) is recommended until platelet counts above 100,000 cell/mcl are achieved, with no signs of bleeding, tapering the dose of GC until discontinuing it, and adding another immunosuppressant to reduce the risk of relapse.190–192 (Moderate quality of evidence, strong recommendation). In cases of severe thrombocytopenia (fewer than 15×109/cell/mcl) or with signs of life-threatening bleeding, methylprednisolone pulses are recommended (1g/24h, intravenous, for 3–5 days, according to the gravity of symptoms) to obtain more rapid responses, ensuring continuation at between .5 and 1mg/kg/day of prednisone or its equivalent to prevent the risk of relapse. It is recommended that these doses should be continued until counts above 50,000 cell/mcl are achieved, and further immunosuppressant should be considered.190–192 (Moderate quality of evidence, strong recommendation) – Intravenous immunoglobulin: is recommended as rescue therapy only for patients with a poor response to GC (i.e., who have received pulses of methylprednisolone for 3–5 days or prednisone or its equivalent, at 1mg/kg/day for more than 4 weeks, and platelet counts do not exceed 50,000 cel/mcl or there are signs of active life-threatening bleeding). It is recommended at a dose of 1g/kg of weight on day 1 and day 2. Response is usually transient (10 days on average).193–196 (Moderate quality of evidence, strong recommendation) – Danazol: is recommended as combined therapy with oral GC, at a dose of 200–800mg/day according to the severity of the throbocytopenia.197,198 (Moderate quality of evidence, strong recommendation) – Antimalarials: are used as adjunct therapy with oral GC at doses between 200 and 400mg/day, according to the severity of the thrombocytopenia.199 (Low quality of evidence, weak recommendation) – Biologics (rituximab): recommended principally in the event of failure with other immunosuppressants. The regimen of 375mg/m2 of body surface area is recommended every week for 4 weeks or the regimen of 1g intravenously on day zero and day 15. The best response is observed when combined with oral GC 1mg/kg/day of prednisone or its equivalent and with tapering doses over 3 months or less.200,201 (High quality of evidence, strong recommendation). The low dose regimen is also recommended for consideration, which comprises 100mg intravenously on days 0, 7, 14 and 21 (i.e., 4 doses, one per week).200,201 (Moderate quality of evidence, weak recommendation) – Splenectomy: principally recommended if thrombocytopenia has been refractory to various immunosuppressant treatments (i.e., final line treatment).202–205 (Low quality of evidence, weak recommendation) – Cyclophosphamide: recommended principally for use in patients who have not responded to the previous treatment; it can even be used as rescue therapy after splenectomy. Intravenous doses of 500mg to 1.2g/month for 3–6 months are recommended, according to the severity of the thrombocytopenia, and clinical response. In very GC-dependent patients, it can be considered as a saving agent for this group of drugs.206–208 (Low quality of evidence, weak recommendation) – Mycophenolate mofetil: recommended for patients who are refractory to the other lines of treatment. The usual dose is between 1 and 2.5g/day, according to tolerance and clinical response.38,209 (Low quality of evidence, weak recommendation) – Azathioprine recommended for use in patients refractory to the other lines of treatment. The recommended dose ranges from .5 to 2mg/kg/day, according to tolerance and response.190,210,211 (Low quality of evidence, weak recommendation) – Eltrombopag: not recommended for routine use due to a lack of evidence.212,213 (Low quality of evidence, strong recommendation) Platelet transfusion: recommended for patients with platelet counts below 10,000 cell/mcl irrespective of whether there are signs of bleeding or counts below 50,000 cell/mcl with active bleeding. In counts above 50,000 cell/mcl, it is only recommended if there is active life or function-threatening bleeding. Ideally, all patients who are to undergo a minor invasive procedure (for example, central line placement, thoracocentesis, etc) require at least 50,000 cell/mcl. With procedures such as surgical interventions or higher risk procedures (kidney biopsy, for example), preferably counts above 100,000 cell/mcl should be maintained.214 (Moderate quality of evidence, strong recommendation) |
| Autoimmune haemolytic anaemia |
| – Biologics (rituximab): principally recommended for use when treatment with other immunosuppressants has failed. The regimen of 375mg/m2 of body surface area (intravenous) can be used every week for 4 weeks or a regimen of 1g intravenously on day zero and day 15.215,216 (Good quality of evidence, strong recommendation). The low-dose regimen comprising 100mg intravenously on days 0, 7, 14 and 21 (4 doses, one per week) can be considered. The best response to this regimen is observed when combined with oral GC 1mg/kg/day of prednisone or equivalent, with tapering doses over 3 months or less.215–219 (Low quality of evidence, weak recommendation) – Glucocorticoids: to attempt to obtain rapid responses (in approx 48–72h) in situations where the anaemia is life-threatening, pulses of intravenous methylprednisolone are recommended (1g/day, for 3–5 days, according to the severity of the anaemia). It is recommended that when going on to oral GC (1mg/kg/day of prednisone or equivalent), this dose should be maintained for 4 weeks at least, and subsequent tapering should be slow and gradual to prevent relapses, until there is a different immunosuppressant and the haemoglobin count is stable and above 7g/dl.43,220–223 (Good quality of evidence, strong recommendation) – Azathioprine: recommended for use as a GC saving agent in cases where there has been relapse on discontinuation or tapering, at doses of .5–2mg/kg day, according to tolerance and clinical response.211,224 (Moderate quality of evidence, strong recommendation) – Danazol: recommended for refractory patients at doses of 200–800mg/day, but as a coadjuvant with other immunosuppressants.197,225–227 (Moderate quality of evidence, strong recommendation) Intravenous immunoglobulin: not recommended due to a lack of sufficient evidence for its recommendation.228 (Low quality of evidence, weak recommendation) – Mycophenolate mofetil: recommended for use in patients refractory to the other treatment lines. Doses of 1–2.5g/day, according to tolerance and clinical response. It can also operate as a GC saver.229–231 (Low quality of evidence, weak recommendation) – Cyclophosphamide: recommended principally for use in patients who have not responded to first or second line treatments; doses of between 500 and 1.2g/month (intravenous) for 3–6 months, according to the severity of the anaemia and clinical response.43,232 (Low quality of evidence, weak recommendation) – Splenectomy: not recommended while there is no available information on their efficacy and safety as routine treatment, except in refractory patients where it is considered that the possible benefit outweighs the risks.43,233 (Low quality of evidence, weak recommendation) – Blood transfusion: not recommended except in life-threatening situations or conditions such as low cardiac output, ischaemic heart disease, severe neurological disorders, etc., always combined with the supervision of haematological doctors before using packs of red cells.234 (Moderate quality of evidence, strong recommendation) |
| Neutropenia |
| – Infection vs manifestation of the disease: infection and the toxic effect of drugs, respectively, must be discounted first, before attributing the manifestation to activity of the disease. (Good practice recommendation) – Granulocyte-colony stimulating factor: in neutropenia <1000/μl, associated with fever or infection starting with 300μg/day is recommended, and continuing with the minimum effective dose to achieve a neutrophil count above 1000/μl.235–240 (Low quality of evidence, strong recommendation) – Glucocorticoids: doses of between .5 and 1mg/kg/day are recommended of prednisone or its equivalent.235,236,241 (quality of evidence, weak recommendation) – Azathioprine: doses of up to 2.5mg/kg/day are recommended, according to response and tolerance.241 (Very low quality of evidence, weak recommendation) – Mycophenolate mofetil: not recommended for use due to the lack of evidence on the optimal dose.235,241 (Very low quality of evidence, weak recommendation) – Cyclosporine: not recommended due to the lack of evidence on the optimal dose.235,241 (Very low quality of evidence, weak recommendation) – Rituximab: recommended in disease refractory to doses of 375mg/m2 of body surface area weekly for 4 weeks or doses of 1g day zero, and day 14.235,241 (Very low quality of evidence, weak recommendation) |
| Thrombotic thrombocytopenic purpura |
| – Plasmapheresis: it is recommended that plasmapheresis should be started as soon as a diagnosis is suspected (in the first 4–8h). Replacement should be with fresh frozen plasma.242–245 (Low quality of evidence, strong recommendation) – Glucocorticoids: recommended for use in combination with plasmapheresis. Pulse methylprednisolone (1g daily for 5 days) or prednisone (or equivalent) at doses of 1mg/kg/day.242–245 (Low quality of evidence, strong recommendation) – Cyclophosphamide: is recommended, even though there is no consensus as to the dose.242–244 (Very low quality of evidence, weak recommendation) – Mycophenolate mofetil: recommended if CYC is contraindicated or has reached its maximum effect; there is no consensus as to the dose.244 (Very low quality of evidence, weak recommendation) – Rituximab: recommended for refractory cases, increasing the response percentage. The recommended dose is 375mg/m2 of body surface area weekly for 4 weeks. It is recommended that plasmapheresis should be delayed for at least 4h after rituximab infusion.242,244,245 (Very low quality of evidence, weak recommendation) – Vincristine: could be used for refractory cases (as an option after rituximab) at single doses of 1.4mg/m2 of body surface, with a maximum of 2mg as the total dose.242,243,245,246 (Very low quality of evidence, weak recommendation). |
| Haemophagocytic syndrome |
| – General measures: provide support treatment (fluid resuscitation, antibiotics, cover transfusion requirements). Look for and treat foci of infection. (Good practice) – Glucocorticoids: pulse methylprednisolone or prednisone (or equivalent) is recommended, there is no consensus as to dose.245,247 (Low quality of evidence, strong recommendation) – Cyclophosphamide: pulses of 500mg to 1g monthly for 6 months247 are recommended. (Low quality of evidence, weak recommendation) – Cyclosporine: doses of 2–5mg/kg/day247 are recommended. (Low quality of evidence, weak recommendation) – Intravenous immunoglobulin: not recommended.247 (Low quality of evidence, strong recommendation) |
Recommendations for Gastrointestinal Manifestations.
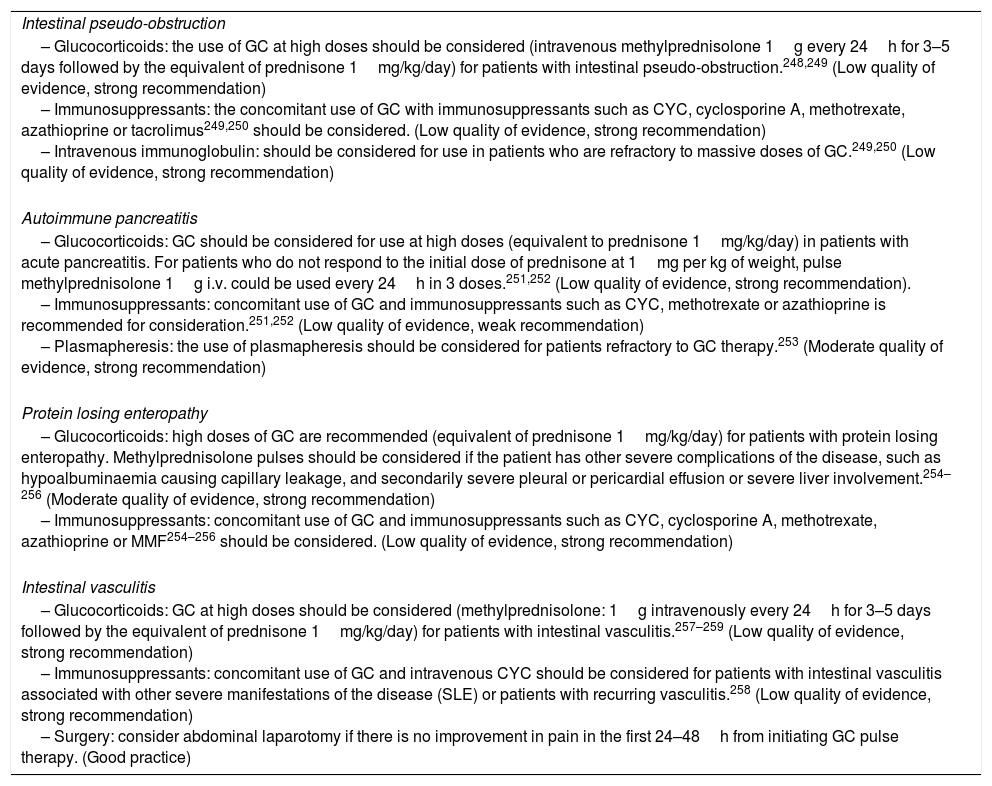
| Intestinal pseudo-obstruction |
| – Glucocorticoids: the use of GC at high doses should be considered (intravenous methylprednisolone 1g every 24h for 3–5 days followed by the equivalent of prednisone 1mg/kg/day) for patients with intestinal pseudo-obstruction.248,249 (Low quality of evidence, strong recommendation) – Immunosuppressants: the concomitant use of GC with immunosuppressants such as CYC, cyclosporine A, methotrexate, azathioprine or tacrolimus249,250 should be considered. (Low quality of evidence, strong recommendation) – Intravenous immunoglobulin: should be considered for use in patients who are refractory to massive doses of GC.249,250 (Low quality of evidence, strong recommendation) |
| Autoimmune pancreatitis |
| – Glucocorticoids: GC should be considered for use at high doses (equivalent to prednisone 1mg/kg/day) in patients with acute pancreatitis. For patients who do not respond to the initial dose of prednisone at 1mg per kg of weight, pulse methylprednisolone 1g i.v. could be used every 24h in 3 doses.251,252 (Low quality of evidence, strong recommendation). – Immunosuppressants: concomitant use of GC and immunosuppressants such as CYC, methotrexate or azathioprine is recommended for consideration.251,252 (Low quality of evidence, weak recommendation) – Plasmapheresis: the use of plasmapheresis should be considered for patients refractory to GC therapy.253 (Moderate quality of evidence, strong recommendation) |
| Protein losing enteropathy |
| – Glucocorticoids: high doses of GC are recommended (equivalent of prednisone 1mg/kg/day) for patients with protein losing enteropathy. Methylprednisolone pulses should be considered if the patient has other severe complications of the disease, such as hypoalbuminaemia causing capillary leakage, and secondarily severe pleural or pericardial effusion or severe liver involvement.254–256 (Moderate quality of evidence, strong recommendation) – Immunosuppressants: concomitant use of GC and immunosuppressants such as CYC, cyclosporine A, methotrexate, azathioprine or MMF254–256 should be considered. (Low quality of evidence, strong recommendation) |
| Intestinal vasculitis |
| – Glucocorticoids: GC at high doses should be considered (methylprednisolone: 1g intravenously every 24h for 3–5 days followed by the equivalent of prednisone 1mg/kg/day) for patients with intestinal vasculitis.257–259 (Low quality of evidence, strong recommendation) – Immunosuppressants: concomitant use of GC and intravenous CYC should be considered for patients with intestinal vasculitis associated with other severe manifestations of the disease (SLE) or patients with recurring vasculitis.258 (Low quality of evidence, strong recommendation) – Surgery: consider abdominal laparotomy if there is no improvement in pain in the first 24–48h from initiating GC pulse therapy. (Good practice) |
SLE, because it is a rare disease, is a less frequent subject of research than other diseases. Therefore, there is a significant need for evidence on effective treatments that also have a lower rate of adverse events. The working panel identified a series of knowledge gaps, and made recommendations so that clinicians, researchers and the pharmaceutical industry can focus their efforts on these research needs to provide increasingly better treatments for patients with this disease.
- 1)
In general, the following need to be designed:
- a)
National multicentre prospective cohort studies.
- b)
Comparative studies with populations from other countries.
- c)
Controlled clinical trials on treatment of the neuropsychiatric manifestations of lupus.
- a)
- 2)
There is a need for clinical trials for the treatment of the articular manifestations of SLE.
- 3)
More evidence is required on the efficacy and safety of tacrolimus in severe SLE, calcium antagonists and immunosuppressant medication (MMF and CYC) in patients with pulmonary hypertension, of CYC, azathioprine, mycophenolate mofetil, danazol, antimalarials in the treatment of patients with SLE and thrombocytopenia or haemolytic anaemia, of CYC for haemophagocytic syndrome and thrombotic thrombocytopenic purpura, giving multiple vaccinations at one visit and tetanus vaccination, recombinant human papilloma virus quadrivalent vaccine, hepatitis B virus and zoster herpes in patients with moderate and severe disease activity.
- 4)
Therapeutic evidence of the use of splenectomy will require more evidence from retrospective studies, since it is not very feasible to undertake a controlled clinical trial.
- 5)
Studies are required on the optimal duration of treatment, and dose tapering schemes when remission of symptoms has been achieved.
- 6)
Studies with greater statistical power are required on gastrointestinal involvement in lupus, since the current studies are case series.
- 7)
Studies are required to determine the required dose of CYC for haemophagocytic syndrome, and thrombotic thrombocytopenic purpura.
Daniel Xibille-Friedman has received honoraria from GlaxoSmithKline for training activities and in clinical trials. Sandra Carrillo-Vázquez has received honoraria from Abbvie, Bristol Myers Squibb, Eli Lilly, Novartis, Pfizer, Roche, Takeda and Janssen. Lilia Andrade-Ortega has received honoraria from Bristol Myers Squibb, Novartis, Pfizer, Roche, Janssen. Miguel Ángel Saavedra has received honoraria from UCB and Pfizer. Leonardo Limón-Camacho has received honoraria from Bristol Myers Squibb, UCB, Pfizer, Janssen, Roche, Lilly and Amgen. Leonor Barile Fabris has received honoraria from Abbvie, Jansen, Roche, Bristol Myers Squibb, UCB, Novartis, Pfizer and GlaxoSmithKline.
Marcela Pérez-Rodríguez, Everardo Álvarez-Hernández, Francisco Javier Aceves, Mario C. Ocampo-Torres, Conrado García-García, José Luis García-Figueroa, Javier Merayo-Chalico, Ana Barrera-Vargas, Margarita Portela-Hernández, Sandra Sicsik, Víctor Manuel Rosales-Don Pablo, Aline Martínez, Pilar Prieto-Seyffert, Mario Pérez-Cristóbal, Zully Castro-Colín, Azucena Ramos, Gabriela Huerta-Sil, María Fernanda Hernández-Cabrera, Luis Javier Jara and Lizbet Tinajero-Nieto have no conflict of interests to declare.
We would like to thank M. en C. Guadalupe Olvera Soto for her invaluable support in the search of the articles used in the literature review; we would also like to thank GlaxoSmithKline for their unconditional educational support.
Please cite this article as: Xibillé-Friedmann D, Pérez-Rodríguez M, Carrillo-Vázquez S, Álvarez-Hernández E, Aceves FJ, Ocampo-Torres MC, et al. Guía de práctica clínica para el manejo del lupus eritematoso sistémico propuesta por el Colegio Mexicano de Reumatología. Reumatol Clin. 2019;15:3–20.


