




The biological disease-modifying anti-rheumatic drugs (DMARDs) have shown great efficacy in the treatment of certain autoimmune diseases. However, due to the immunosuppression they entail, the patient may be affected by opportunistic germs. We present the rare case, in our setting, of a patient with rheumatoid arthritis complicated by mucocutaneous leishmaniasis in the context of treatment with adalimumab.
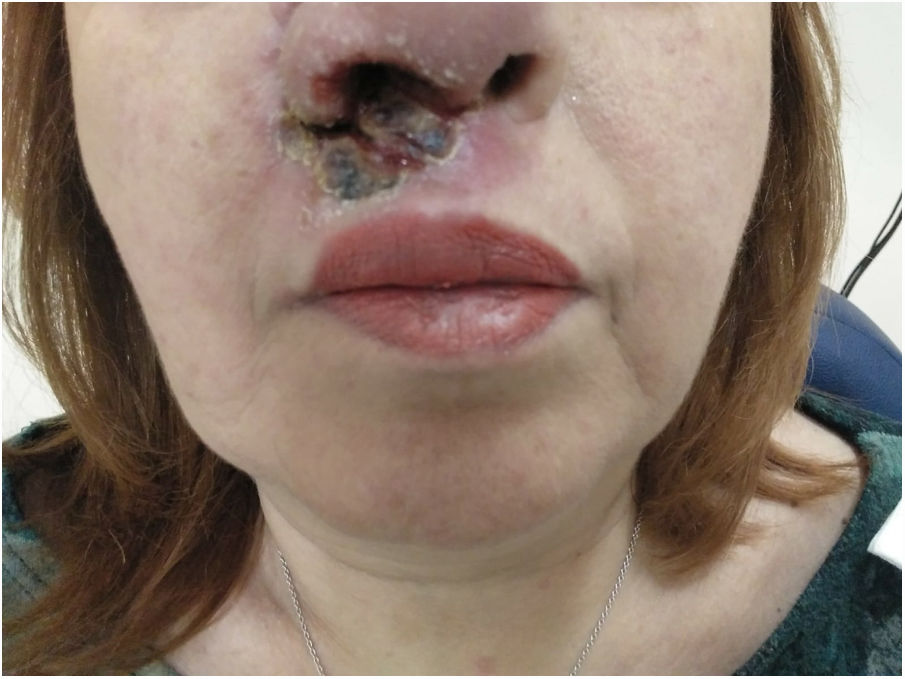
This is a 53-year-old woman who was diagnosed with seropositive rheumatoid arthritis and treated with methotrexate in 2000. In 2013, adalimumab (one injection/15 days) plus methotrexate (10mg/week) was used due to poor progress. Since then, she has not required steroids and has remained asymptomatic with this therapeutic approach. She recently presented a mucocutaneous, erythematous and ulcerous lesion in the nasal vestibule and the upper lip that has deformed her nose (Fig. 1). For this reason, she was referred to the ENT department, where a biopsy was performed and the subsequent anatomopathological study was diagnostic of leishmaniasis, both by direct vision with the Giemsa technique and by nested polymerase chain reaction. The patient had not travelled to particularly endemic areas of this disease, nor lived with animals, nor had she any record of a bite. Adalimumab was then suspended, and she was referred to the infectious disease department, where visceral involvement was ruled out and she was treated with liposomal amphotericin B, which solved the problem.
This disease is a zoonosis caused by Leishmania, its infantum variety being the most prevalent in Spain. It is endemic in India, Bangladesh, Sudan and Brazil and it is seen, to a lesser extent, in Southern Europe. The dog is the main reservoir, and it is transmitted through the bite of the female Phlebotomus mosquito. After its bite, there can be a mucocutaneous involvement with erythematous and ulcerous lesions in the face, arms and legs. In our case it was centred in the nose, forcing us to rule out a Wegener's granulomatosis. There can also be an exclusively cutaneous form and another visceral form (kala-azar) that usually presents with fever, constitutional syndrome, adenopathy, visceromegaly and pancytopenia. Diagnosis is established by means of culture, direct vision (Giemsa technique) or polymerase chain reaction testing. Treatment is generally with amphotericin B.1–10
The biological DMARDs were initially used in rheumatoid arthritis and, later, their indication was extended to other autoimmune diseases (spondyloarthropathies, juvenile idiopathic arthritis, skin psoriasis, Crohn’s disease, ulcerative colitis, uveitis and suppurative hidradenitis in the case of adalimumab). These drugs have the disadvantage of immunosuppression and, consequently, of encouraging infections by opportunistic germs, especially mycobacteria. More exceptionally, infections by other germs have been described, as in this case. However, they can appear not only with the biological DMARDs, since leishmaniasis has also been described in the context of treatment with conventional steroids and DMARDs. The problem is reintroducing an immunosuppressant in the event of rheumatic flare-up, since leishmaniasis relapses have been described. In this case, some authors advise using etanercept as the most recommended drug and, perhaps, it would also be a good idea to consider therapeutic targets other than anti-TNF. In any case, stricter monitoring for reactivation of leishmaniasis is always necessary.1–10
Therefore, any patient presenting skin lesions of the characteristics described in the text and being treated with immunosuppressant drugs such as those used in autoimmune rheumatic disease, especially anti-TNF-α, should first be considered for leishmaniasis. In addition, patients treated with these drugs who travel to endemic areas of this disease should be particularly monitored.
Please cite this article as: Bruscas Izu C, Lázaro Sánchez A, Alonso Alonso ML, Álvarez Alegret R. Leishmaniasis cutánea: a propósito de un caso en el contexto del tratamiento con adalimumab. Reumatol Clin. 2021;17:304–305.


