






Elastofibroma dorsi is a benign, uncommon fibroelastic tissue condition, more common in women after the fifth decade of life. It is usually located in the subscapular region, and can sometimes be bilateral. We present 4 patients, between 53 and 73 years of age, with this disease. It is often an asymptomatic lesion that can manifest, even at its apex, with mild pain when moving the scapula. All our patients had pain. The diagnosis is based on clinical findings and imaging studies, especially ultrasound, computed tomography (CT), and nuclear magnetic resonance. The biopsy is reserved for patients who have no characteristic signs on imaging. In our series, surgical excision was necessary in one of the patients, and in the others, clinical and imaging studies allowed us to arrive at a definitive diagnosis.
El elastofibroma dorsi es un tumor benigno, poco frecuente, de tejido fibroelástico, más común en mujeres luego de la quinta década de vida. Se suele localizar en la región subescapular, pudiendo en ocasiones ser bilateral. Presentamos 4 pacientes, entre 53 y 73 años de edad, con esta patología. Frecuentemente es una lesión asintomática, aunque puede observarse dolor leve con resalto de la escápula al realizar movimientos. Todas nuestras pacientes presentaron dolor y una de ellas además resalto de la escápula. El diagnóstico se basa en los hallazgos clínicos y los estudios por imágenes, especialmente la ecografía, la tomografía computarizada y la resonancia magnética nuclear. La biopsia se reserva para los casos sospechosos que no presentan en los estudios por imágenes el patrón característico. En nuestra serie, la extirpación de la lesión fue necesaria en una de las enfermas, ya que en las demás la clínica y los estudios por imágenes permitieron arribar a un diagnostico definitivo.
Elastofibroma dorsi is an uncommon benign tumor of fibroelastic tissue, more common in women after fifty. It is commonly located in the subscapular region and can sometimes be bilateral.1 It usually manifests as a palpable lump with pain on mobilization of the shoulder. Diagnosis is based on physical examination and imaging studies, although histopathology is usually necessary. The differential diagnosis includes other benign tumors and neoplasias.2 Keeping it in mind is important in order not to subject patients to unnecessary tests and procedures. We present4 patients with this rare pathology.
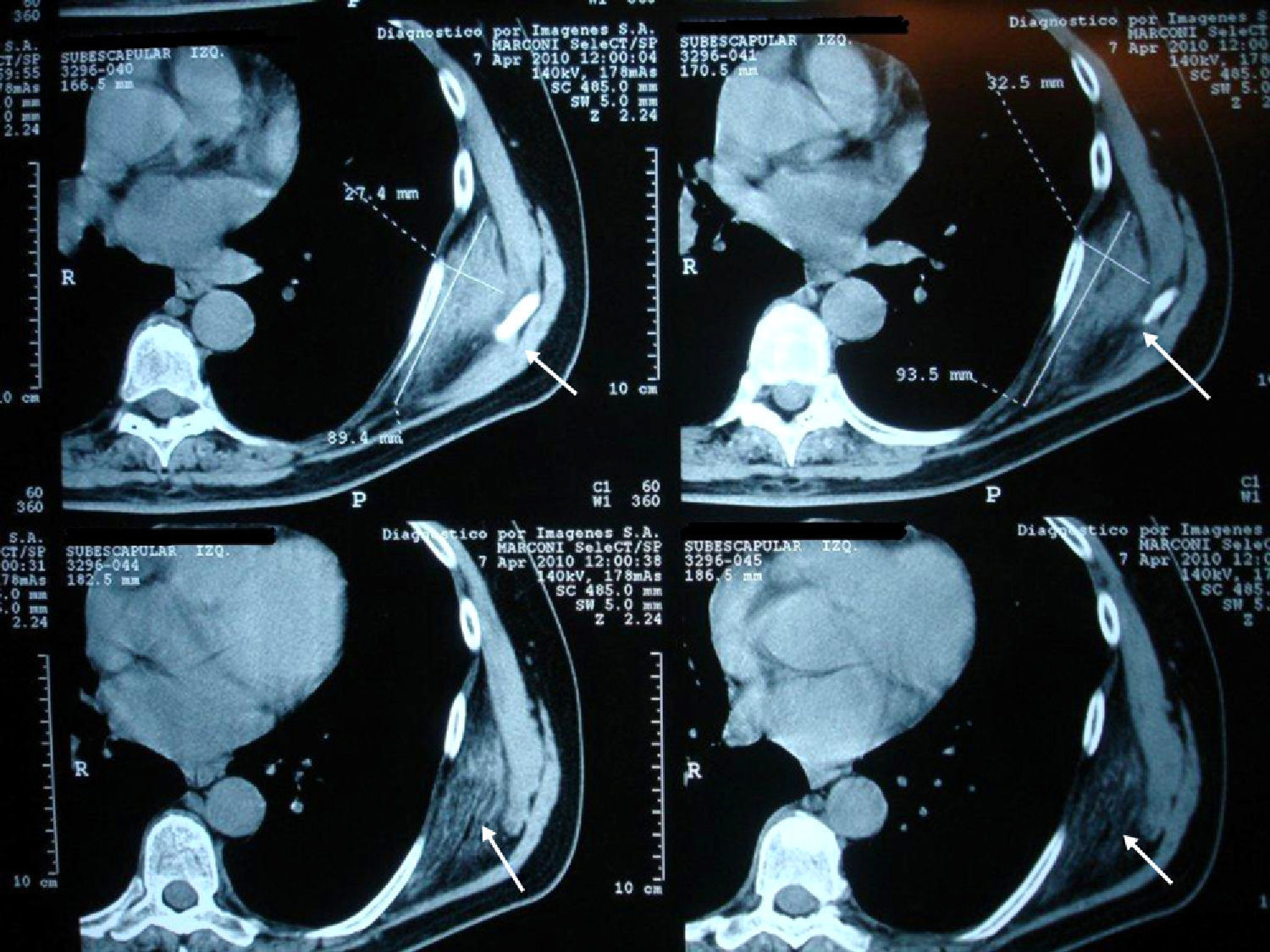
Clinical CasesCase 1A 73-year-old patient with a history of osteoarthritis in their hands presented with pain in the left scapular region of 3 months duration, which was exacerbated by physical activity, referring the pain to the scapular area of the shoulder after movement. Physical examination found a hard consistency, elastic, painless mass approximately 7cm in diameter in the left subscapular region. Ultrasonography of the affected region reported a solid mass of the chest wall, which was below the serratus anterior (Fig. 1). CT scan showed a unencapsulated occupying mass with density similar to muscle, mixed with adipose tissue bands in the left infrascapular region of 8.8 by 2.4cm (Fig. 2). Hematological and biochemical analyzes were normal. The orthopedics department suggested excision of the lesion, but the patient refused surgery. A control CT scan 2 years later showed no changes.

A 67-year-old, previously healthy patient, presented with pain in his right shoulder lasting 5 months, which was exacerbated by physical activity. On physical examination there was a hard, elastic, painless mass of about 10cm in diameter below the right scapular region. He underwent a bone scan that was compatible with arthritis. The shoulders X-ray was normal, whereas ultrasonography showed a mass in the shoulder supporting the diagnosis of a vertex elastofibroma dorsi. Magnetic resonance imaging (MRI) showed an infrascapular mass of 9 by 3cm in the right region, characterized by the interposition of areas of dense connective tissue and fat tissue. After 2 years the lesion showed no changes.
Case 3A woman of 53 years of age with a history of emphysema, presented with pain in the right interscapular region lasting 2 months. Physical examination showed a hard, elastic, painless tumor, about 5cm in diameter. Ultrasound of the region showed a formation of 6 by 2cm compatible with elastofibroma dorsi, confirming the diagnosis by CT. Hematological and biochemical analyzes were normal. No changes were observed in the lesion in the past 3 years.
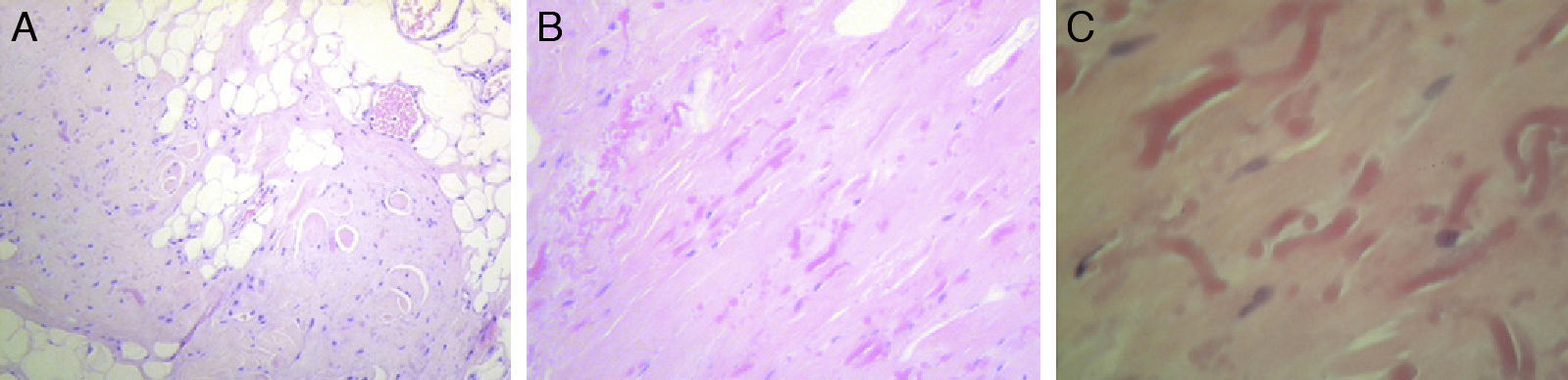
Case 4A 60-year-old with a history of osteoarthritis in the hands and thyroid nodules with hypothyroidism treated with levothyroxine consulted in January 2008 due to pain in the left subscapular region since one month earlier, which was increasing in size and spreading to the pectoral region, with limited movement of the left shoulder. Physical examination showed a painless mass of soft consistency with irregular margins of about 5cm in diameter but with painful restriction of left shoulder movement. Ultrasound of the area showed a heterogeneous solid formation of 2.5 by 4.5cm in diameter, with partially defined contours, while in the right subscapular region a solid, ovoid formation was observed, 2.5 by 1cm diameter, with homogeneous margins, which occupied the right subcutaneous plane. Hematological and biochemical analyzes were normal. In April 2008, the patient underwent surgery for the left lesion, it being a heterogeneous tumor, adhered to deep planes, ribs, and pleura. The pathologist described a proliferation composed of abundant dense collagen tissue of myxoid aspect, which included rare spindle cells with minimal nuclear irregularity and numerous fragmented elastic fibers intermingled with mature adipose tissue, consistent with elastofibroma dorsi (Fig. 3A–C).
Due to shoulder and right dorsal region pain, the second tumor was excised in May 2009 with a good recuperation of function and decreased pain. Histology was also consistent with elastofibroma dorsi.
DiscussionAlthough elastofibroma dorsi is regarded as an uncommon, Brandser et al. reported a prevalence of 2% in people over 60 years, studied by CT,3 while an autopsy study found a prevalence of 24% in women and 11% in men.4
It usually occurs in women after age 50, with a slight predominance in the right subscapular region below the serratus muscle, although it has also been found in the suprascapular region, deltoid, trochanter, ischial tuberosity, olecranon, and feet and may be bilateral in 10%–66% of cases, 2.5 In our series, 4 women presented it, between 53 and 73 years of age. Two of them showed a right side location, one had it in left side and one was bilateral. Three of them had subscapular tumors and only one presented an interscapular location.
The lesion is usually asymptomatic, but may present with mild pain at the shoulder or with scapular movement and the pain may radiate to the shoulder, which sometimes leads to an erroneous diagnosis of rotator cuff injuries or subacromial6 bursitis. All our patients had pain and, in addition, one had referred pain of the scapula with movements.
Imaging studies are useful for diagnosis, with ultrasound showing an alternating pattern of fasciculated type or laminar, hypo- and hyperechoic lines parallel to the chest wall and the Doppler signal is usually negative, demonstrating the absence of intrinsic vascularity. These data are usually sufficient to make a diagnosis.2,7 Ultrasound images of our patients were indicative of the lesion, although no Doppler study was performed. CT shows the alternation of adipose tissue and fibrous tissue with muscle density, not enhanced by contrast.8 MRI reported an alternating pattern of adipose and fibrous tissue and, in T1 and T2 sequences, fibrous tissue shows signs of low intensity similar to muscle. Adipose tissue shows signs of high signal intensity on T1 and intermediate T2. STIR sequences of the lesion observed areas of high and low intensity, enhanced with the use of gadolinium.9 Biopsy is reserved for suspicious cases that do not exhibit a characteristic pattern. The macroscopic appearance of the tumor is hard, elastic, yellowish-white tissue, about 5–10cm. The size of tumors in our series ranged from 2 to 9cm, coincident with what is described in the literature.2 Histopathological studies show the interposition of collagen fibers with mature adipose tissue without an inflammatory infiltrate.8 One of the patients underwent a surgical excision, but clinical and imaging studies allowed a definitive diagnosis in the others.
In conclusion, elastofibroma dorsi is an uncommon tumor, occurring in women over 50 years and has a characteristic sonographic pattern. In doubtful cases, one must perform a CT or MRI, and it rarely requires surgical treatment, except in those patients with pain or functional limitation.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data. The authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consent. The authors have obtained the informed consent of the patients and /or subjects mentioned in the article. The author for correspondence is in possession of this document.
Conflict of InterestThe authors declare no conflict of interest.
Please cite this article as: Cavallasca JA, et al. Elastofibroma dorsi: revisión de 4 casos. Reumatol Clin. 2012;8:358–60.


