




A case is presented of a hemarthrosis associated with osteochondritis dissecans in a young man who arrived in the emergency unit due to tender and swelling of his right knee 1h after a slightly rotational gesture of the lower limb. Many years before the patient suffered a sports injury in the same knee, but it was never assessed. Radiography studies showed bone fragments inside the synovial capsule, and the joint aspiration was compatible with hemarthrosis. A review of the available information of this uncommon condition is also presented.
Presentamos el caso de una hemartrosis de rodilla asociada a osteocondritis disecante en un adulto joven que consultó por urgencias debido a dolor y tumefacción de su rodilla derecha media hora después de un gesto rotacional del miembro inferior. Varios años antes el paciente sufrió un accidente deportivo en la misma rodilla por la que nunca consultó. El estudio radiológico mostró 2 fragmentos dentro de la cápsula sinovial y una artrocentesis demostró hemartrosis. Realizamos una revisión de la información disponible de esta patología infrecuente.
Osteochondritis dissecans (OCD), or König disease, is a rare form of osteochondrosis in which, as a consequence of the necrosis of a small fragment of subchondral bone, the bone sequestrum and the articular cartilage that covers it ultimately break loose from the adjacent bone and cartilage, and become lodged in the joint as a loose body.1,2 A prevalence of less than 0.1% has been established among children participating in sports3 and the prevalence in the general population is unknown, whereas the incidence is estimated to be between 1.5 and 1.6 new cases per 100 000 population/year.4–6 Although the pathophysiology is not fully understood, it is considered to be a consequence of a vulnerable subchondral area being subjected to repetitive microtrauma. It is for this reason that its prevalence appears to be higher among children than among adults.2,3,7,8 There have been reports of cases of the simultaneous involvement of both knees or even of different joints, a fact that indicates that there may be etiologies other than trauma.9–11
Case ReportA previously healthy 23-year-old man presented with a 3-h history of pain associated with swelling and functional limitation of his right knee, with onset a half an hour after twisting it while walking. He did not participate in sports because running long distances produced knee pain. He had stopped playing soccer at the age of 13 years due to multiple injuries to his right knee. He had not been examined by a physician at that time.
Physical examination revealed that the knee was warm to the touch, swollen and painful. Arthrocentesis yielded 10cc of serosanguineous fluid. This fluid was examined under a polarized light microscope to rule out microcrystal deposition disease. Other studies performed were Gram stain and culture of the fluid, which also excluded joint infection.
Three radiographs revealed the presence of 2 radiopaque intra-articular loose bodies (Fig. 1).
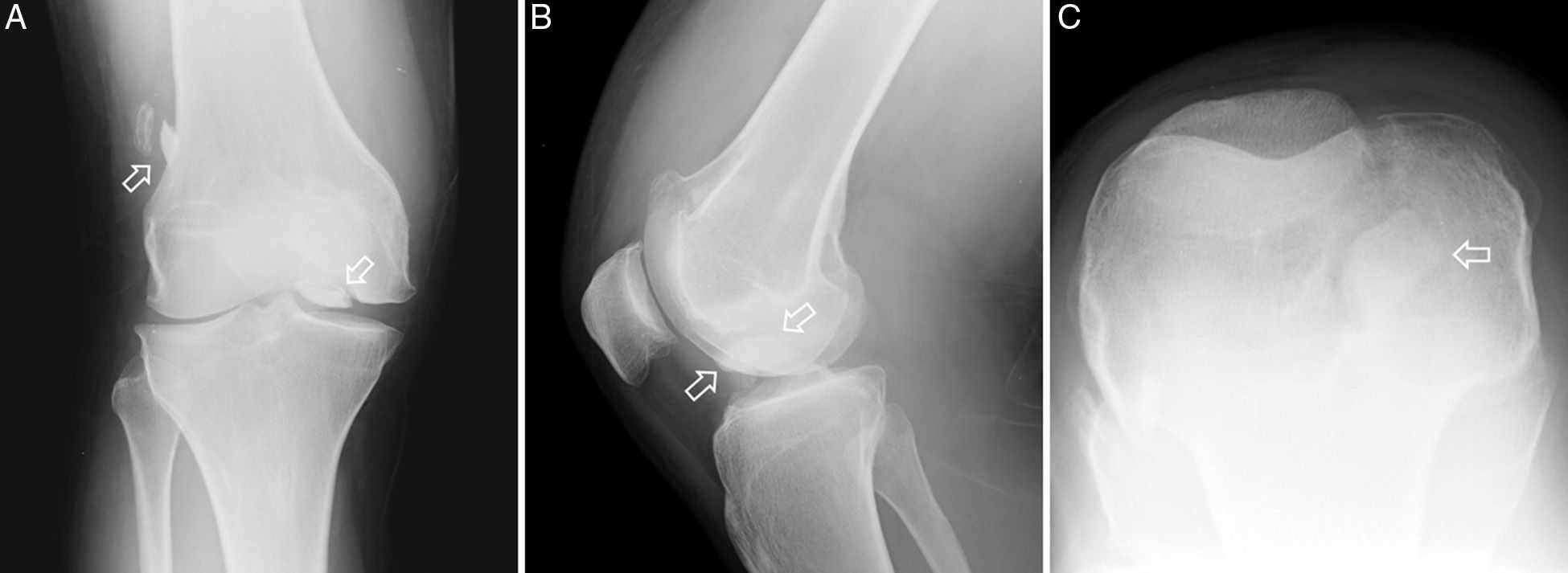
Radiographic study of right knee. (A) Anteroposterior view showing 2 fragments (arrows). (B) Lateral view. The arrows indicate the fragment that was more probably the cause of hemarthrosis. (C) Knee in hyperflexed position enabling the localization of the larger of the two fragments with respect to the axis of the knee.
Arthroscopy showed a tear measuring approximately 4mm in length over the weight-bearing cartilage from which a fragment with a maximum diameter of 16.1mm was removed. This lesion was not treated. Another loose body with a diameter of 9.6mm was removed from the joint cavity. In addition, there was a scar at the level of the posterolateral portion of the internal femoral condyle, which was assumed to correspond to the original lesion that gave rise to the OCD.
DiscussionHemarthrosis secondary to a tear as the presenting sign of long-standing OCD has not previously been reported. It is usually diagnosed immediately or shortly after the occurrence of a subchondral lesion in young athletes or children.6,7,10–12
Osteochondritis is considered to be a consequence of a temporary or permanent arrest of the blood flow in a section of subchondral tissue.4,6,7 As a result, this tissue becomes detached from the articular surface, further impeding the delivery of nutrients, until ultimately it dies and is reabsorbed.2,5–7 In rare situations, such as the case reported here, the ischemia involves a large section of subchondral tissue. The organic components of the bone fragment continue their natural history, whereas the inorganic portion breaks off and is converted into intra-articular loose bodies.4,6,7,12,13 These loose bodies can cause joint locking when they come into contact with other structures.6
At the present time, the development of the events that lead to OCD is considered to involve a multifactorial process: major trauma, repetitive microtrauma, abnormal bone formation processes, abnormal joint mechanics and genetic predisposition.2,6,7
Osteochondritis dissecans affects the posterolateral aspect of the medial femoral condyle in approximately 70% of the cases and the inferocentral portion of the lateral condyle in 10%–20%, whereas the sum of other sites represents less than 1% of the cases.5,6
Our hypothesis is that, in our patient, one of the fragments caused a tear that ultimately resulted in hemarthrosis and produced the signs that led to the diagnosis.
In OCD, the original lesion may have occurred months or years before the diagnosis, although the patient usually consults a physician immediately because of the pain.6,7 While the original lesion in our patient was not documented, his medical records indicate that it may have occurred around 10 years before the development of hemarthrosis.
ConclusionsThe case presented here highlights 2 important aspects to be taken into account when evaluating patients with knee pain: the importance of a medical record that focuses on past physical activity and injuries and the consideration of OCD in the differential diagnosis of hemarthrosis in young adults.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of InterestThe authors declare that there are no conflicts of interest.
Please cite this article as: Astete CG, Alva García P, Carpena Zafrilla M, Medina Quiñones C. Hemartrosis de rodilla secundaria a osteocondritis disecante (enfermedad de König). Reumatol Clin. 2015;11:322–324.


