




Alkaptonuria is a hereditary metabolic disorder caused by homogentisate 1,2-dioxygenase (HGD) deficiency. Oxidative conversion of HGD leads to the production of a melanin polymer, whose accumulation in the connective tissue causes a characteristic pigmentation known as ochronosis. The fusion of the ochronotic pigment to the conjunctive tissue causes a multisystem disorder characterized by premature spondyloarthritis. Other systemic characteristics include calculi (salivary, renal, biliary), renal failure, respiratory failure, hearing loss, aortic valve disease, osteoporosis and rupture of tendons, muscles and ligaments.1–4 Prolapsed discs are rare5 and vertebral fracture is an exceptional complication, with only one case reported in the literature.6
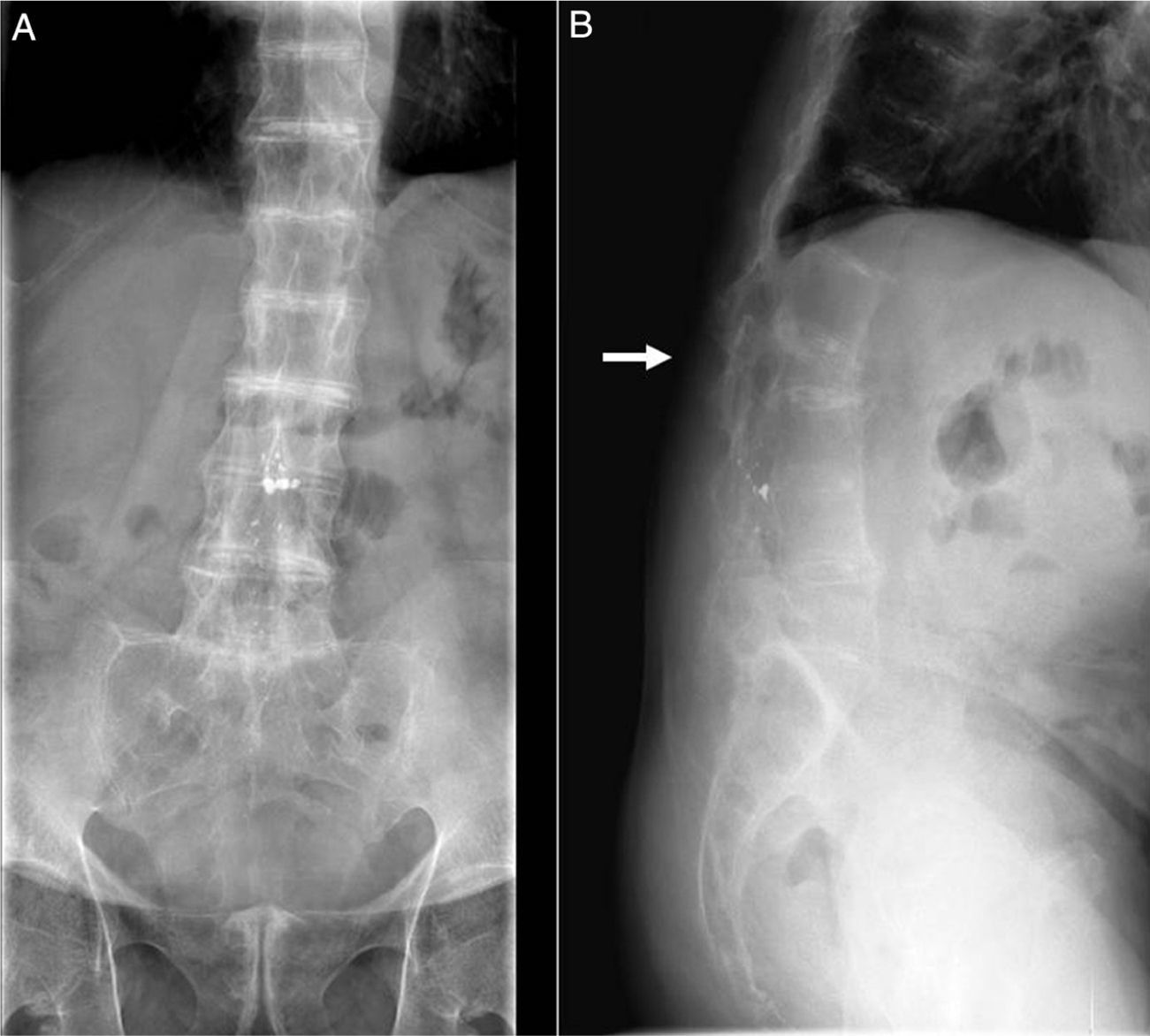
We present the case of a 55-year-old male patient who had been referred to our consultation to evaluate chronic thoracolumbar pain. Findings of the physical examination included an important reduction in spinal column mobility and grey-brown pigmentation of both sclerae. After the radiology study (Fig. 1), we decided to measure HGD levels in urine (4218.0mg/L; normal<10mg/L), which confirmed the suspected diagnosis of ochronosis. The patient began with physical therapy sessions, and the improvement was noticeable. At that time (January 2004), dual-energy X-ray absorptiometry was used to determine the bone mineral density (BMD) of the lumbar spine (LS), which showed a T-score of −3.0 SD. The patient initiated treatment with risedronate (75mg weekly). In March 2005, BMD was evaluated once again, with a T-score of −2.4 SD in the LS, −30 SD in the femoral neck (FN) and −2.7 SD in the total hip (TH). Treatment was continued with bisphosphonates, and then changed to alendronate (70mg weekly). In June 2007, BMD showed improved T-scores in the LS (−1.7 SD) and TH (−2.3 SD) and stabilization in the FN (−3.0 SD). In January 2013, the patient came to our emergency department with acute back pain, but reported having had no trauma. Lateral LS radiography revealed a fracture of the third lumbar vertebra (Fig. 1). After that incident, we opted to begin treatment with subcutaneous teriparatide. To date (November 2014), no new vertebral fractures have appeared.
There are several hypotheses that attempt to explain how the accumulation of HGD leads to ochronosis and arthropathy. These include the interference of HGD with the intertwining of collagen fibres and inflammatory response triggered by free radicals formed by the oxidation of HGD.2 As for the development of osteoporosis, Aliberti et al. indicated that ochronosis can be associated with a higher rate of bone resorption, which would involve accelerated bone mass loss.7 The same authors showed the ineffectiveness of alendronate for reverting the process of bone mass loss in a considerable number of patients with ochronosis and osteoporosis. This suggests that the existence of a specific physiopathological mechanism (microlesions of the matrix, viability of the osteocytes and deterioration of the collagen network), not involved in the pharmacodynamics of bisphosphonates, could be responsable.8 Although our patient had advanced-stage disease (stage IV, osseous ankylosis9) and in spite of the reported general tendency, his BMD progressively increased thanks to treatment with bisphosphonates. It did not, however, prevent the appearance of a vertebral fracture due to fragility. Given that treatment with bisphosphonates is well tolerated and can improve BMD in some cases, this treatment could be useful in patients with ochronosis and osteoporosis. Its indication should be individualized until new scientific evidence is reported.
Please cite this article as: Calero Paniagua I, Montilla Morales CA, Carranco Medina TE, Sánchez González MD. Ocronosis y osteoporosis: a propósito de un caso. Reumatol Clin. 2015;11:330–331.


