






Gout is a disorder of purine metabolism resulting in the deposition of urate crystals around joints.1,2 Chronic Gout is characterized by destructive arthritis, often with degenerative changes, bone erosions and development of tophi. Acute attacks can become polyarticular, additive and ascending; with a tendency to increase in severity.3 Tophi area cardinal feature of this entity; their structure consists of a conglomerate of urate crystals surrounded by4 fibrosis and inflammatory tissue.
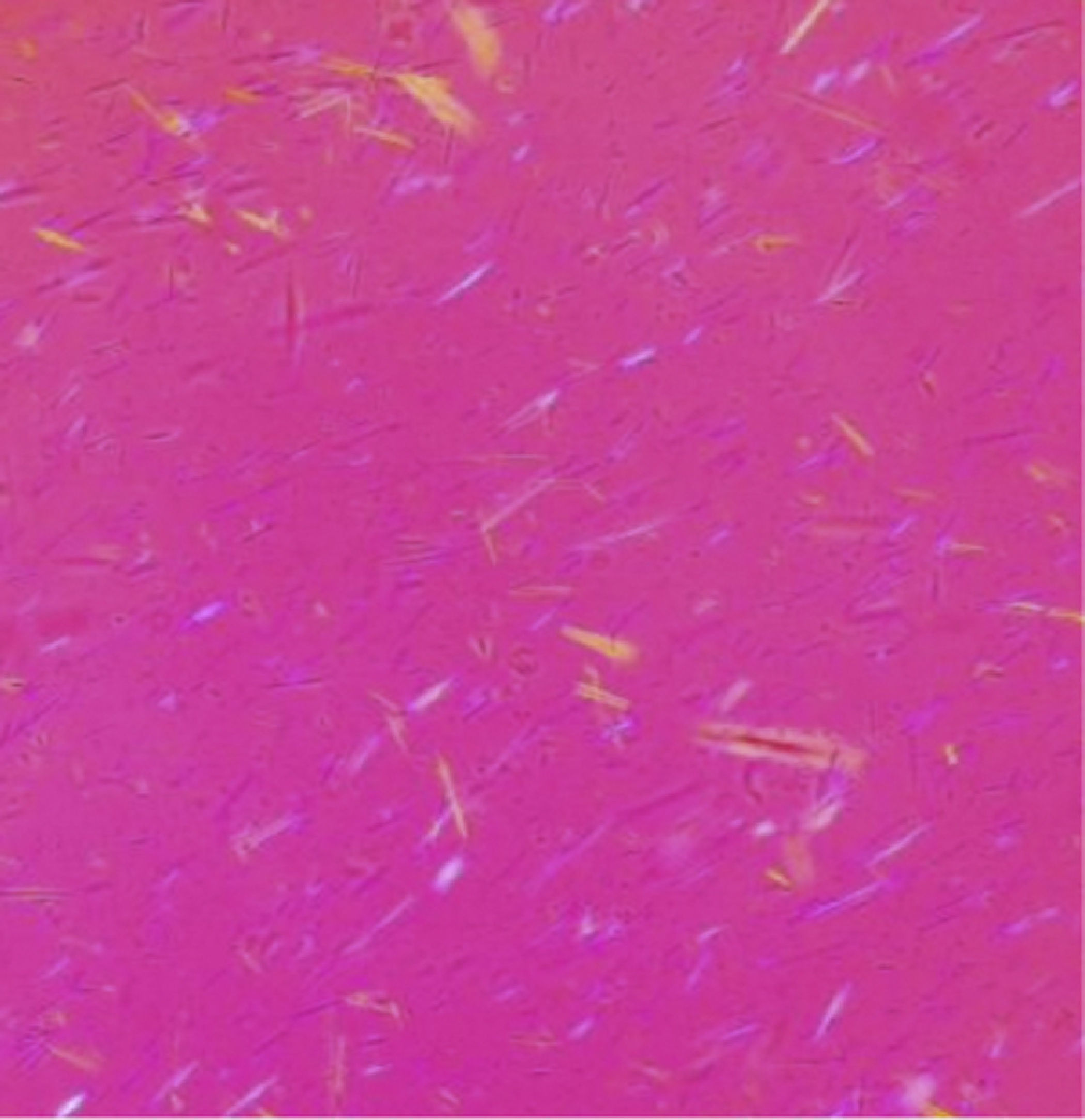
Clinical CaseThe patient is a 46-year-old male with a history of hyperuricemia, traumatic amputation of the 4th and 5th fingers of the left hand and chronic tophaceous gout which appeared eight months prior, self-medicated with corticosteroids. He was admitted with a history of 12 days of increased volume in the second finger of the left hand, with added pain, hyperemia and a discharge of purulent material. On physical examination, tophi were found in both elbows, hands and feet and flexor extensor surfaces, the largest covering the entire left second finger (Fig. 1). At admission, levels of uric acid and cortisol were 10.4mg/dl and 10.39mg/dl, respectively; the eGFR was 11.96ml/min.3 The exudative material found on tophi by needle aspiration was analyzed under polarized light microscopy, revealing abundant crystals of monosodium urate and a few leukocytes (Fig. 2). Aspirate cultures were reported negative for bacterial growth. Typical erosions were seen on hand X-rays (Fig. 3).

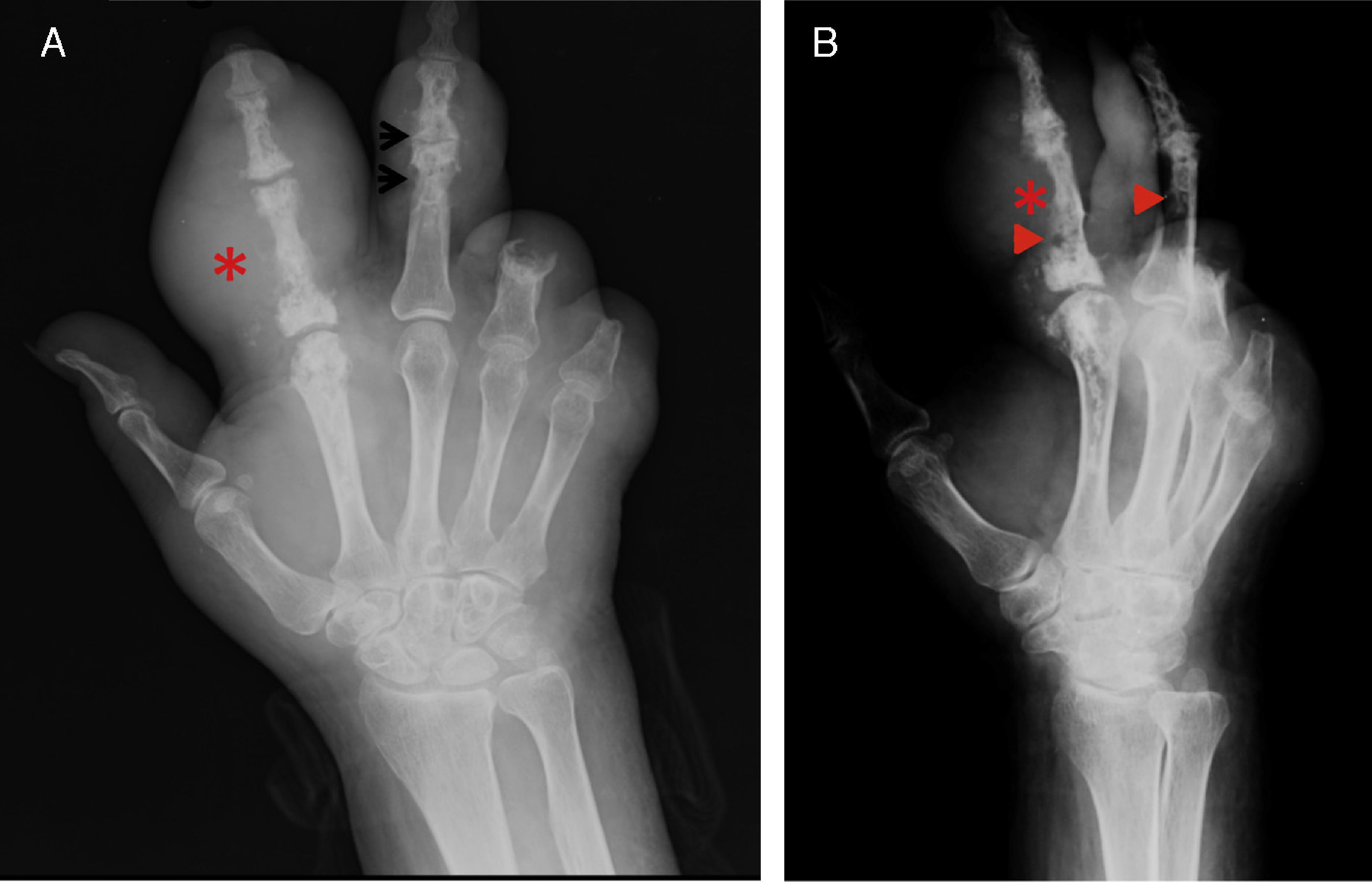
(A) Dorsopalmar X-ray of the left hand. (B) Lateral X-ray of the left hand. Both show a volume increase of soft tissue of the second and third finger corresponding with tophi (*). The bone tissue shows the presence of “punched-out” erosions with a sclerotic border (arrows) and with loss of the joint space.
Monosodium urate crystals trigger an intense inflammatory response that can perpetuate their presence. This inflammatory process is mediated by the release of cytokines, including: TNF, IL-6, and chemokines ligands CXC8 and CXC1.5,6
Their presence is considered the gold standard for diagnosis.7
The classic presentation of acute attacks is that of a self-limiting monoarticular arthritis, most often of the first metatarsophalangeal joint.7 In some cases, large deposits of urate can drain as a whitish calcareous material that is often confused with a drained abscess. This has been described mainly in the olecranon bursa or the first toe.8
Fever is often present as part of the clinical presentation of patients. Their identification can distinguish it from other diseases with similar clinical manifestations, e.g. infections, which is vital since treatment and prognosis are radically different.
Ethical ResponsibilitiesProtection of people and animalsThe authors declare this research did not perform experiments on humans or animals.
Data privacyThe authors state that no patient data appears in this article.
Right to privacy and informed consentThe authors state that no patient data appears in this article.
Please cite this article as: Zapata Bonilla SA, Jaquez Nevarez MR, López Reyes A, Rodríguez Henríquez P. Exudado en «arcilla blanca» en gota tofácea crónica. Reumatol Clin. 2015;11:328–329.


