


This study assesses the relationship between the ability to perform productive activities and the clinical characteristics of RA, such as disease activity, quality of life, functional capacity, workload, pharmacotherapy, and comorbidities.
Materials and methodsA cross-sectional, observational and descriptive study was conducted. Patients aged 18–75 years with a diagnosis of RA according to ACR/EULAR 2010 criteria who attended regularly to the Rheumatology service in the period between January and March 2017 were included. The questionnaires, WPAI-AR, HAQ-DI and RAQoL, were applied. RA disease activity was measured by DAS28-PCR. Correlations were made between the clinical data obtained and work productivity and activity impairment measured by WPAI-AR.
ResultsTwo hundred four patients with a diagnosis of RA were included, of whom 92.6% were women. Mean age was 54.46±9.3 years. Regarding the percentage of impairment of daily life activities, we found a significant difference between employed and unemployed patients (P≤.002). A positive correlation was found between RA activity measured by DAS28-PCR, quality of life, and functional ability with the percentages of absenteeism, presenteeism, overall productivity loss, and impairment of daily life activities.
ConclusionA correlation between RA disease activity, functional capacity, quality of life, and working impairment was found. The strongest association was established with the degree of functional capacity.
Valorar la relación entre la productividad laboral y diversos factores propios de la artritis reumatoide (AR) como grado de actividad de la enfermedad, nivel de discapacidad, calidad de vida, carga laboral, farmacoterapia recibida y comorbilidades asociadas.
Material y métodosSe realizó un estudio transversal, observacional y descriptivo. Se incluyeron pacientes de 18 a 75 años con diagnóstico de AR según criterios ACR/EULAR 2010 que acudieron consecutivamente a la consulta de Reumatología del Hospital Universitario en el periodo comprendido entre enero y marzo del año 2017. Se aplicaron los cuestionarios WPAI-AR, HAQ-DI y RAQoL; el grado de actividad de la AR se calculó mediante DAS28-PCR. Se realizaron correlaciones entre las características clínicas obtenidas y la capacidad laboral por WPAI-AR.
ResultadosSe incluyeron 204 pacientes con AR, de los cuales el 92,6% fueron mujeres; la edad media fue de 54,46±9,3 años. En el porcentaje de déficit en actividades básicas de la vida diaria (ABVD) se encontró diferencia estadísticamente significativa entre pacientes empleados y desempleados (p≤0,002). Se encontró correlación positiva entre actividad de la enfermedad por DAS28-PCR, nivel de calidad de vida por RAQoL y capacidad funcional por HAQ-DI con los porcentajes de ausentismo y presentismo laboral, pérdida de la productividad laboral total y déficit en ABVD.
ConclusiónExiste correlación entre el grado de actividad de la AR, calidad de vida y capacidad funcional con el rendimiento laboral de la población estudiada. La asociación más fuerte encontrada fue con la capacidad funcional.
Rheumatoid arthritis (RA) is a chronic inflammatory systemic disease of unknown aetiology characterised by joint destruction which mostly presents in the productive age group. Most incidents occur between the ages of 35 and 45 and it affects between .03% and 1.5% of the population worldwide, predominantly women in the ratio of 3:1.1 In Mexico, RA has an estimated prevalence of 1.6% in the adult population2; this disease is currently a public health problem due to the high rates of occupational disability and disability pensions involved,3 with a catastrophic impact on family finances and health institutions.4–6
The impact of RA for paid work is described as a loss of effective working time (absenteeism), reduced performance during working hours (presenteeism) and changes to timetables or loss of employment (change of employment status). The impact on unpaid labour refers to the individual's difficulties in carrying out routine activities at home, going shopping or caring for children.7
It has been described that the majority of patients with RA will present with some type of occupational disability during the course of the disease.8 Nearly 80% of adults of working age with this disease will experience limitations in carrying out activities at work and major restrictions in undertaking social roles,9 and this has been linked to a lower functional capacity, lower quality of life and a higher degree of RA activity.10,11 Despite the degree of functional disability and pain which have been consistently associated with problems in employment since the early stages of the disease, only a few studies provide information on the determining factors of this effect.12
The Work Productivity and Activity Impairment Questionnaire in Rheumatoid Arthritis (WPAI-AR) is a tool that has been validated into Spanish in Spain and this allows us to measure the difficulty in carrying out work activities and basic everyday life activities (BDLA) in patients with RA.13,14 By using this test it is possible to measure performance at work and difficulties when undertaking unpaid work for 7 days prior to its application – the period of time reported as an appropriate estimation to represent the negative effects on work productivity due to the disease.15
Absenteeism and presenteeism are common phenomena in RA patients but have not been described in the Mexican population. This study aims to assess the relationship between work productivity and several factors pertaining to the disease, such as degree of RA activity, the level of disability, quality of life, work load, pharmacotherapy received and associated comorbidities.
Materials and methodsStudy designThis was a cross-sectional, observational and descriptive study which was approved by the Research Ethics Committee of the University Hospital Dr. José Eleuterio González.
Patient selectionAll patients between 18 and 75 years of age with a diagnosis of RA according to the AmeIQRan College of Rheumatology (ACR) criteria from 1987 and/or the European League Against Rheumatism (EULAR)/ACR from 201016,17 who regularly attended the outpatients service of the Rheumatology Department of the University Hospital Dr. José Eleuterio González during the period between January and March 2017 were included. Any individuals who presented with visual, auditive, verbal or cognitive disability were excluded, as were those who refrained from participating in the study.
VariablesAfter obtaining verbal consent, the WPAI-RA test translated into Spanish was applied to all study subjects as part of their routine consultation. The level of functional disability in RA was measured using the Health Assessment Questionnaire Disability Index (HAQ-DI), which comprised 20 questions for expressing and assessing 8 basic aspects of daily life such as getting dressed, eating or walking; a higher score signified greater functional limitation.18 The patients’ quality of life was measured by the Rheumatoid Arthritis Quality of Life Scale (RAQoL), a tool comprising 30 responses to statements written in the first person with dichotomist answers to assess different aspects of the quality of life of the individuals who are affected by RA; the higher the score, the worse the quality of life.19 Estimation of RA activity was made by the Disease Activity Score scale of 28 articulations (DAS-28 score) by CRP.20,21 Demographic characteristics of the patients were among the variables studied, and included age, sex, body mass index (BMI), civil status, type of work, workload, time of evolution of RA, comorbidities and treatment. The degree of physical workload was calculated using the scale described by Pujol,22 and the type of employment using the International Standard Classification of Occupations 2008 of the International Labour Organisation (CIUO-08).23 People were considered employees when their productive activities were financially rewarded (self employment or third party contract). All tools were applied by the same resident doctor in their fourth year of internal medicine. The data obtained were stored on an electronic database.
DataThe normality of quantitative variable distribution was measured with the Shapiro–Wilk test. Variables with normal distribution were described using the standard deviation (SD)±mean; variables with non normal distribution were described with median and interquartile range (IQR) of 25 and 75 percentile. Spearman's rho was used to measure the correlation between work productivity and the results obtained by the tools used. Comparison of variables was made using the ANOVA test. A multivariable lineal regression analysis was made with the baseline characteristics of the patients. Data were analysed using the statistical package SPSS version 22 (IBM, New York, United States).
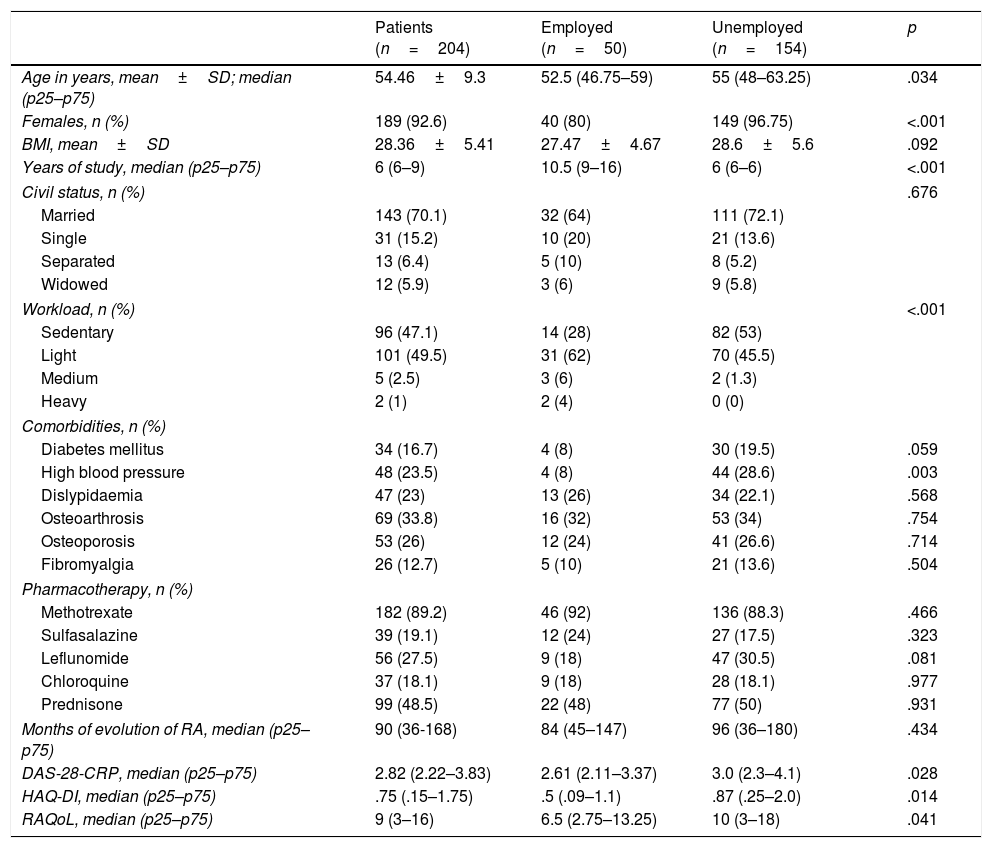
ResultsClinical and demographic traits of both groups are described in Table 1. Two hundred and four subjects were included in the study, the majority of whom were women (92.6%). Mean age was 54.46±9.3 years, with a BMI of 28.36±5.41kg/m2. The median evolution of RA was 90 months (IQR 36–168), with a level of activity measured by the DAS-28-CRP of 2.82 (IQR 2.22–3.83). Functional capacity measured by HAQ-DI, obtained a median of 0.75 points (IQR .15–1.75), whilst in quality of life a score of 9 (IQR 3–16) was made using the RAQoL. Fifty patients were engaged in remunerated employment activities, which corresponded to 24.5% of the total sample. On comparing the groups of employees and the unemployed a statistically significant difference was found in age, sex, years of study, workload, prevalence of high blood pressure, level of RA activity measured by DAS-28-CRP, functional capacity by HAQ-DI and quality of life by RAQoL.
Clinical and demographic characteristics.
| Patients (n=204) | Employed (n=50) | Unemployed (n=154) | p | |
|---|---|---|---|---|
| Age in years, mean±SD; median (p25–p75) | 54.46±9.3 | 52.5 (46.75–59) | 55 (48–63.25) | .034 |
| Females, n (%) | 189 (92.6) | 40 (80) | 149 (96.75) | <.001 |
| BMI, mean±SD | 28.36±5.41 | 27.47±4.67 | 28.6±5.6 | .092 |
| Years of study, median (p25–p75) | 6 (6–9) | 10.5 (9–16) | 6 (6–6) | <.001 |
| Civil status, n (%) | .676 | |||
| Married | 143 (70.1) | 32 (64) | 111 (72.1) | |
| Single | 31 (15.2) | 10 (20) | 21 (13.6) | |
| Separated | 13 (6.4) | 5 (10) | 8 (5.2) | |
| Widowed | 12 (5.9) | 3 (6) | 9 (5.8) | |
| Workload, n (%) | <.001 | |||
| Sedentary | 96 (47.1) | 14 (28) | 82 (53) | |
| Light | 101 (49.5) | 31 (62) | 70 (45.5) | |
| Medium | 5 (2.5) | 3 (6) | 2 (1.3) | |
| Heavy | 2 (1) | 2 (4) | 0 (0) | |
| Comorbidities, n (%) | ||||
| Diabetes mellitus | 34 (16.7) | 4 (8) | 30 (19.5) | .059 |
| High blood pressure | 48 (23.5) | 4 (8) | 44 (28.6) | .003 |
| Dislypidaemia | 47 (23) | 13 (26) | 34 (22.1) | .568 |
| Osteoarthrosis | 69 (33.8) | 16 (32) | 53 (34) | .754 |
| Osteoporosis | 53 (26) | 12 (24) | 41 (26.6) | .714 |
| Fibromyalgia | 26 (12.7) | 5 (10) | 21 (13.6) | .504 |
| Pharmacotherapy, n (%) | ||||
| Methotrexate | 182 (89.2) | 46 (92) | 136 (88.3) | .466 |
| Sulfasalazine | 39 (19.1) | 12 (24) | 27 (17.5) | .323 |
| Leflunomide | 56 (27.5) | 9 (18) | 47 (30.5) | .081 |
| Chloroquine | 37 (18.1) | 9 (18) | 28 (18.1) | .977 |
| Prednisone | 99 (48.5) | 22 (48) | 77 (50) | .931 |
| Months of evolution of RA, median (p25–p75) | 90 (36-168) | 84 (45–147) | 96 (36–180) | .434 |
| DAS-28-CRP, median (p25–p75) | 2.82 (2.22–3.83) | 2.61 (2.11–3.37) | 3.0 (2.3–4.1) | .028 |
| HAQ-DI, median (p25–p75) | .75 (.15–1.75) | .5 (.09–1.1) | .87 (.25–2.0) | .014 |
| RAQoL, median (p25–p75) | 9 (3–16) | 6.5 (2.75–13.25) | 10 (3–18) | .041 |
RAR: rheumatoid arthritis; DAS-28-CRP: Disease Activity Score of 28 articulations; SD: standard deviation; HAQ-DI: Health Assessment Questionnaire Disability Index; BMI: body mass index; HAQ-DIRAQoL: Rheumatoid Arthritis Quality of Life Scale.
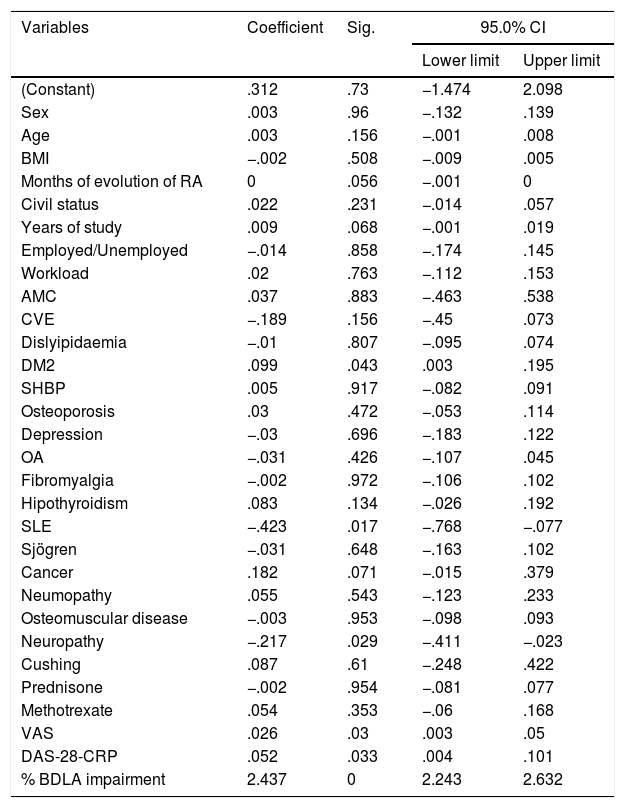
Multivariable analysis was carried out, relating the baseline characteristics for the patients with their level of functional capacity. With regard to the HAQ-DI scale, a statistically significant association was found with the presence of diabetes mellitus type 2 (p=.043), systemic lupus erythematosus (p=.017) and neuropathy (p=.029). Among the indicators that were measured in this study we found a statistically significant relationship with the analogous assessment of pain (p=.03), RA activity by DAS-28-CRP (p=.033) and percentage of deficit in BDLA (p=.001) (Table 2).
Multivariable analysis acceding to HAQ-DI.
| Variables | Coefficient | Sig. | 95.0% CI | |
|---|---|---|---|---|
| Lower limit | Upper limit | |||
| (Constant) | .312 | .73 | −1.474 | 2.098 |
| Sex | .003 | .96 | −.132 | .139 |
| Age | .003 | .156 | −.001 | .008 |
| BMI | −.002 | .508 | −.009 | .005 |
| Months of evolution of RA | 0 | .056 | −.001 | 0 |
| Civil status | .022 | .231 | −.014 | .057 |
| Years of study | .009 | .068 | −.001 | .019 |
| Employed/Unemployed | −.014 | .858 | −.174 | .145 |
| Workload | .02 | .763 | −.112 | .153 |
| AMC | .037 | .883 | −.463 | .538 |
| CVE | −.189 | .156 | −.45 | .073 |
| Dislyipidaemia | −.01 | .807 | −.095 | .074 |
| DM2 | .099 | .043 | .003 | .195 |
| SHBP | .005 | .917 | −.082 | .091 |
| Osteoporosis | .03 | .472 | −.053 | .114 |
| Depression | −.03 | .696 | −.183 | .122 |
| OA | −.031 | .426 | −.107 | .045 |
| Fibromyalgia | −.002 | .972 | −.106 | .102 |
| Hipothyroidism | .083 | .134 | −.026 | .192 |
| SLE | −.423 | .017 | −.768 | −.077 |
| Sjögren | −.031 | .648 | −.163 | .102 |
| Cancer | .182 | .071 | −.015 | .379 |
| Neumopathy | .055 | .543 | −.123 | .233 |
| Osteomuscular disease | −.003 | .953 | −.098 | .093 |
| Neuropathy | −.217 | .029 | −.411 | −.023 |
| Cushing | .087 | .61 | −.248 | .422 |
| Prednisone | −.002 | .954 | −.081 | .077 |
| Methotrexate | .054 | .353 | −.06 | .168 |
| VAS | .026 | .03 | .003 | .05 |
| DAS-28-CRP | .052 | .033 | .004 | .101 |
| % BDLA impairment | 2.437 | 0 | 2.243 | 2.632 |
BDLA: basic daily life activities; RA: rheumatoid arthritis; DAS-28-CRP: Disease Activity Score de 28 articulations; DM2: diabetes mellitus type 2; VAS: visual analogue scale; CVE: cerebral vascular event; SHPB: systemic high blood pressure; AMI: acute myocardial infarction; CI: confidence interval; BMI: body mass index; SLE: systemic lupus erythematosus; OA: osteoarthrosis.
The indicators of work productivity calculated by WPAI-AR are described in Table 3. The percentage of deficit in BDLA was 20% (IQR 0–40%) in the group of workers, whilst in the group of unemployed it was en 40% (IQR 17.5–70). A statistically significant difference (p=.002) was found between the two groups.
Work productivity according to WPAI-AR.
| Employed (n=50) | Unemployed (n=154) | |
|---|---|---|
| Percentage of absenteeism from work, median (p25–p75) | 0 (0–9.7) | N/A |
| Percentage of presenteeism at work, median (p25–p75) | 20 (0–50) | N/A |
| Percentage of loss of total work productivity, median (p25–p75) | 26.9 (0–56.2) | N/A |
| Percentage of impairment in BDLA, median (p25-p75) | 20 (0–40) | 40 (17.5–70) |
BDLA: basic everyday life activities.
Using Spearman's rho a weak positive correlation was found between the RA activity measure by DAS-28-CRP and the percentages of presenteeism (r=.400; p=.004), loss of total work productivity (r=.388; p=.005) and percentage of deficit in BDLA (r=.486; p≤.001).
Correlations were made according to the classification of the RA activity index by DAS-28-CRP and the WPAI-AR questionnaire, separating them into patient groups in clinical remission, slight, moderate or high activity. No lineal relationship was found between the different groups of disease activity and performance at work.
A weak positive correlation was found between a high score in the RAQoL questionnaire and the percentage of absenteeism from work (r=.414; P=.003); a moderate positive correlation with the percentage of absenteeism from work (r=.641; P≤.001), percentage of loss of total productivity (r=.653; P≤.001) and percentage of deficit in BDLA (r=.728; P≤.001).
Functional capacity obtained using HAQ-DI had a positive correlation with the percentage of absenteeism at work (r=.448; P≤.001) and a strong positive correlation with the percentages of presenteeism (r=.911; P≤.001), percentage of total loss of productivity (r=.894; P≤.001) and percentage of deficit in BDLA (r=.945; P≤.001).
The duration of the disease had a weak negative correlation with the percentage of absenteeism from work (r=−.320; P=.023). The BMI had a weak negative correlation with the duration of the disease (r=−.343; P=.015).
According to the CIUO-2008, the type of employment of the group of workers was classified mainly as trader (34%), domestic cleaner (16%), office worker (10%) and secretary (8%). Most patients assessed perceived that the level of demand for physical activity in their employment was sedentary (28%) or slight (62%). The degree of workload was not associated with a higher percentage in deficit in overall working capacity. Furthermore, educational level lacked any significant association with regard to absenteeism or presenteeism and BDLA, with a median of 10.5 (IQR 9–16) years of study in the employed group. No statistically significant correlation was found between the gender of the patients, nor age, or civil status with the indicators of unemployment described in the WPAI-AR.
All the people of the employed group presented with at least one associated comorbidity, the most common of osteoarthrosis (32%), dislypidaemia (13%), osteoporosis (24%), osteomuscular diseases (24%) and fibromyalgia (10%). In the analysis by pathologies a statistically significant association was found between the presence of fibromyalgia and the percentage of deficit in BDLA (P=.018). The other individual comorbidites described did not show any association with work productivity or unemployment of BDLA. The presence of two or more accumulated comorbidities in the same patient had no statistically significant correlation either with work performance.
In accordance with the prescribed medication in the group of employees, in the patient population with RA, 92% used methotrexate, 48% prednisone, 24% sulfasalazine, 18% leflunomide, 24% chloroquine or its derivatives and 2% biological agents. No statistically significant correlation was found between the indicators of work productivity and the type of pharmacotherapy received by the patients, with each drug being individually assessed.
DiscussionA relationship may be established between the quality of life of patients with RA and their performance at work using different clinical triggers represented in the questionnaires HAQ-DI, RAQoL and WPAI-AR. The results obtained in the questionnaire WPAI-AR show that the patient group who were employed demonstrated greater capacity in performing BDLA compared with the group of unemployed people. A series of factors may be determined which can contribute to explaining this phenomenon, such as lower age, better control of the disease, better quality of life and type of physical work undertaken depending on educational level and functional capacity.
In the prospective study of González et al.8 in Mexican patients it was demonstrate that a quarter of the subjects with RA who were included presented with at least one episode of occupational disability during a year of follow-up whilst 4% developed permanent occupational disability. Our study systematically assesses absenteeism and presenteeism, which had not previously been described in our population.
On studying the group of employed patients we found a positive correlation between the level of RA activity, quality of life and functional capacity with the indicators of performance at work described in the WPAI-AR. This coincides with that found by Chaparro et al.10 in the Argentinean population. Even when the majority of correlations found between RA activity and quality of life were statistically poor, the functional capacity assessed using HAQ-DI had a strong degree of correlation with work capacity, conferring this test with an excellent predictive value for detecting impairment in undertaking these activities. As pointed out by Nagasawa and Kameda,24 different factors such as functionality and an appropriate adherence to treatment have repercussion on carrying out work activities and BDLA.
The negative correlation found between disease duration and percentage of absenteeism from work in the simple could be explained by adaptation to their symptoms, with them being able to undertake activities at work to a greater extent with the passing of time, in contrast to that previously described.9,10 Furthermore, negative correlation found between BMI and disease duration may be explained by RA's rheumatic cachexia which has been reported in the literature.25
The multivariable analysis carried out in this study refers to several comorbidities including diabetes, neuropathy and generalised lupus erythematosus having negative effects on undertaking BDLA. An association has been reported between the presence of comorbidities in patients with RA and poorer overall outcomes.26 However, according to the correlation analyses undertaken, only fibromyalgia predisposed greater impairment in carrying out BDLA, without having any significant impact on employment capacity. The other comorbidities described have no significant impact on overall performance, in contrast to that described by Dougados et al.27 This may be explained by the fact that RA symptoms in the majority of these diseases are treated comprehensively. The type of work carried out by patients with RA (being mainly light in load) may also be the reason for this finding.
We should highlight that there was low use of biological agents in the study population, which may have been associated with socioeconomic factors. On being assessed individually, specific pharmacotherapy for RA treatment was not related to greater difficulty in carrying out work activities. However, greater analysis of this point is required, including the medication used to treat the other existing comorbidities and the role of the polypharmacy in this context, which was associated with poorer outcomes in these patients.28
After correlation analysis no significant relationship could be established between gender, age, physical work demand or educational level and the degree of impairment in work performance of the individuals assessed. It is important to point out that in this study over 90% of patients were women and a large percentage of them had no paid work. Even though this study focused on employed patients, a large number of the sample analysed were working in activities connected to household hygiene and cleaning. In this respect the study highlighted that socioeconomic factors and the level of disease activity have a great impact on the ability to undertake BDLA.29
One of the limitations of this study is that patients were only recruited from one centre of reference and the cross-sectional design did not enable the establishment of a temporary relationship between the effects of the factors assessed and overall work capacity. As there were so many factors affecting the outcome, weighted analysis of all related variables was complex. The tools used did not allow for any discernment between people undertaking employment activates under their own initiative (self-employed) and those working under a contract remunerated by a third party. This is something that needs to be evaluated in future studies, since the patient's employment profile is of influence here.
One of the study strengths is that it is the first study of its type in Mexican patients, due to the number of tools used for assessment and the number of people included, which was greater than any previous publication.
Absenteeism and presenteeism are factors which are present in this RA patient group, mainly for those whose disease is more active and who have a lower functional capacity or poorer quality of life. The level of functional capacity was the most strongly associated factor in this respect. For the sake of reducing the economic and social impact of absenteeism and presenteeism we would recommend assessing the level of performance at work when assessing response to treatment in these patients.
Conflict of interestsThe authors have no conflicts of interest to declare.
The authors would like to thank the valuable collaboration of the Department of Internal medicine of the University, Mr. José Eleuterio González, directed by Dr. Homero Náñez Terreros.
Please cite this article as: Salazar-Mejía CE, Galarza-Delgado DÁ, Colunga-Pedraza IJ, Azpiri-López JR, Wah-Suárez M, Wimer-Castillo BO, et al. Relación entre productividad laboral y características clínicas de la artritis reumatoide. Reumatol Clin 2019;15:327–332.


