







The rheumatology service of Ciudad Real Hospital, located in an autonomous community of that same name that is nearly in the center of Spain, implemented a self-management model of successive appointments more than 10 years ago. Since then, the physicians of the department schedule follow-up visits for their patients depending on the disease, its course and ancillary tests.
The purpose of this study is to evaluate and compare the self-management model for successive appointments in the rheumatology service of Ciudad Real Hospital versus the model of external appointment management implemented in 8 of the hospital's 15 medical services.
Material and methodsA comparative and multivariate analysis was performed to identify variables with statistically significant differences, in terms of activity and/or performance indicators and quality perceived by users. The comparison involved the self-management model for successive appointments employed in the rheumatology service of Ciudad Real Hospital and the model for external appointment management used in 8 hospital medical services between January 1 and May 31, 2016.
ResultsIn a database with more than 100,000 records of appointments involving the set of services included in the study, the mean waiting time and the numbers of non-appearances and rescheduling of follow-up visits in the rheumatology department were significantly lower than in the other services. The number of individuals treated in outpatient rheumatology services was 7768, and a total of 280 patients were surveyed (response rate 63.21%). They showed great overall satisfaction, and the incidence rate of claims was low.
ConclusionOur results show that the self-management model of scheduling appointments has better results in terms of activity indicators and in quality perceived by users, despite the intense activity. Thus, this study could be fundamental for decision making in the management of health care organizations.
El Servicio de Reumatología del Hospital de Ciudad Real tiene implementado un modelo de autogestión de citaciones de consultas sucesivas desde hace más de 10 años, en el que son los facultativos del propio servicio los que gestionan las citas de revisión de los pacientes en función de su enfermedad, evolución, pruebas complementarias…
El propósito del presente estudio es valorar y comparar el modelo de autogestión de citas sucesivas del Servicio de Reumatología del Hospital de Ciudad Real frente al modelo de gestión externa de citas implantado en 8 de los 15 servicios médicos del hospital.
Material y métodosSe realizó un análisis comparativo y multivariante para la identificación de variables con diferencias estadísticamente significativas, en términos de indicadores de actividad/rendimiento y de calidad percibida por los usuarios, entre el modelo de autogestión de citas sucesivas del Servicio de Reumatología del Hospital de Ciudad Real, y el modelo de gestión externa de citas de 8 servicios médicos del hospital, entre el 1 de enero y el 31 de mayo de 2016.
ResultadosEn una base de datos con más de 100.000 registros de las citaciones del conjunto de servicios incluidos en el estudio, el tiempo medio de espera y los números de incomparecencias y reprogramaciones para consultas sucesivas del servicio de reumatología fueron significativamente inferiores al resto de servicios. El número de pacientes atendidos en consultas externas de reumatología fue de 7.768 y, de estos, se le realizó una encuesta a un total de 280 pacientes (tasa de respuesta del 63,21%), donde destaca una gran satisfacción global, además de una tasa de incidencia de reclamaciones baja.
ConclusiónNuestros resultados denotan que el modelo de autogestión de citaciones tiene mejores resultados, tanto en indicadores de actividad como en la calidad percibida por los usuarios, a pesar de la intensa actividad, por lo que este estudio puede ser fundamental para la toma de decisiones en la mesogestión de organizaciones sanitarias.
The self-management model stands out among the different appointment management systems for out-patient visits to hospital. In this model, the doctors in the department itself manage the appointments for patient check-ups, depending on their disease, evolution and complementary tests…On the other hand there is the external management model, in which the out-patient admission service manages appointments according to organizational criteria, such as the availability of time slots or the types of tests requested, among others.
At the current time no evidence has been found to indicate which of the 2 models is the most efficient and best-appreciated by users.
The Rheumatology Department of the Integrated Care Management System of Ciudad Real (ICM CR) uses an external management model for initial visits and a self-management model for following visits. In the ICM CR 8 departments use the external appointments management system for first visits as well as for subsequent ones.
This study aims to perform a comparative analysis, in terms of activity and user-perceived care quality indicators, between the self-management model for successive visits to the rheumatology service and the external appointment management model used in 8 of the 15 medical departments of the ICM CR.
Material and MethodsActivity/performance data were obtained for this study from the management system. They refer to the patient visits from 1 January 2015 to 31 May of the same year, for the rheumatology department and the 8 medical departments with no self-management model selected for the study. A total of 36,799 visits were selected.
Apart from the rheumatology department, the medical departments included in the study were: cardiology, digestive system, endocrinology, geriatrics, internal medicine, pneumology, neurology and pediatrics.
The following variables were included as activity/performance data: number of first visits, number of subsequent visits, average waiting time for the first visit and for subsequent visits, number of patients discharged from out-patient departments, number of failures to appear and number of rescheduled first and subsequent visits. These data were supplied by the management monitoring service and recorded in a large database. The SPSS 21 program was used for statistical analysis. Completed visits were selected as the unit of analysis, and the data were subjected to descriptive analysis. The existence of statistically significant differences between departments with different outpatient appointment management models was analyzed in connection with 2 variables identified by multivariate analysis: waiting time for first and subsequent visits, and the number of appointment changes for first and subsequent visits. These variables were considered to be directly associated with the quality of care and perceived satisfaction of service users.
The following data were obtained in the analysis of perceived quality:
- •
Complaints incidence rate (CIR), as well as the main categories/reasons for complaints in the first six months of 2016, through the user services department. A comparative analysis between departments was undertaken.
- •
The rheumatology department nursing staff carried out a telephonic satisfaction survey. An ad hoc questionnaire was designed, composed of questions on a Lickert-type scale with 10 alternatives answers (from disagree very strongly to agree very strongly, scoring from 0 to 10. It also contains open questions with user suggestions and comments.
The reference population consisted of all the patients who had been seen in the rheumatology outpatient department from 1 January 2016 to 31 May of the same year, i.e., 7768 patients. The calculated size of sample was 280 patients, and this number ensures representativeness at a 95% confidence level. The sample was selected randomly using the patients’ clinical history numbers.
The telephonic surveys took place in August and September 2016. They included the items considered to have the greatest specific weighting in level of satisfaction: degree of satisfaction with the waiting time before the first and subsequent visits, with appointment rescheduling (accessibility), with appointment cancelation or delays, and with the information received about visit cancelations/delays. The survey also covered overall satisfaction with how patients were treated in their visits to the rheumatology department.
ResultsThere were a total of 36,799 visits by patients during the period from 1 January to 31 May 2016, to the rheumatology department and the other departments included in the study.
To analyze activity/performance a database was designed containing more than 100,000 records of appointments in all of the medical departments that were included.
There were 2886 first visits and 7331 subsequent visits to the rheumatology department. A total of 912 patients (8.02%) were discharged from the outpatient department, without the possibility of distinguishing between first and subsequent visits in this respect.
The waiting time before the first visit was found to be significantly longer for rheumatology than it was for all of the other departments included in the study (P<.0001) (Fig. 1). In comparison with the other departments, the waiting time for subsequent visits to the rheumatology department was found to be significantly shorter. The exceptions to this were the geriatric and internal medicine departments (for which the differences were not statistically significant) (Fig. 2).


The percentage of patients who failed to appear for their first appointment in the rheumatology department was similar to that of all the departments, i.e., 14.29% vs 15.11%, respectively (in absolute terms, 420 vs 1455). For subsequent appointments in the rheumatology department the figure was lower than it was for the total of all the departments analyzed, at 7.35% vs 12.98%, respectively, (503 vs 3669 in absolute terms (Fig. 3).

The number (and percentage) of rescheduled first and subsequent appointments in rheumatology are significantly lower than the corresponding figure for all of the other departments analyzed, as a whole and individually (Figs. 4 and 5).


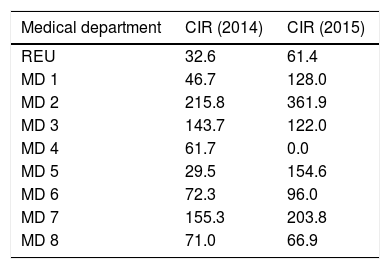
In the perceived quality analysis the CIR amounted to a total of 61.1 in the year 2015, and if the waiting list is excluded it stood at 4.2. This means that 93.13% of the CIR in rheumatology in the year 2015 was due to the waiting list (Fig. 6). When the rheumatology CIR is compared with those of the other medical departments analyzed it was found to be lower in all cases except for geriatrics in the year 2015 and internal medicine in 2014 (Table 1).

The telephone satisfaction survey gained a response from 177 patients of the 280 who had been selected, i.e., a response rate of 63.21%. The degree of satisfaction with the waiting time was 4.58 for the first appointment and 7.08 for subsequent ones. The degree of satisfaction with rescheduled appointments (accessibility) was 3.77. Appointment cancelation or delays due to the hospital occurred for 18.9% of those interviewed (n=53), and their satisfaction with the information they had received about cancelation/delay amounted to 7.17. In general the average overall level of satisfaction with the treatment received in the rheumatology outpatient department was 8.81.
DiscussionOur study found that the high number of referrals (higher than the average in the rest of Castile-La Mancha) led to a long waiting time for the first appointment. However, for subsequent appointments the waiting time was shorter than it was in the other departments, except for the geriatrics and internal medicine departments. This was due to the limitation of the lower number of patients seen by these departments and the fact that they have fewer available rooms and professionals. Stable planning of the agenda 6 months beforehand leads to fewer rescheduled appointments for the rheumatology department. Additionally, contacting patients personally by telephone gives rise to a fall in the percentage of failures to appear in subsequent appointments. This is not the case for the first appointment, given that this percentage is similar to those of the other departments. The vast majority of the CIR in the rheumatology department were found to be due to the waiting list, and even so, it is lower than those of the other departments without appointment self-management. Lastly, the telephonic survey of patients showed an outstandingly high level of satisfaction with the rheumatology department.
From the first the basic hypothesis was that the appointment self-management system gives better results, in activity indicators as well as in user-perceived quality indicators. Nevertheless, strategic decision-making for implementing one model or another requires robust analysis of the information, and it must be result-based.1,2 The results in our study were good. This study may form the basis for decision-making at the middle management level of healthcare organizations.
Conflict of InterestsThe authors have no conflict of interests to declare.
The authors would like to thank all of the departments involved in this study, as it would not have been possible without their help in data gathering, classification and analysis, as well as in interpreting them and applying them to achieve better organization of the healthcare system over the short term.
Please cite this article as: Castro Corredor D, Cuadra Díaz JL, Mateos Rodríguez JJ, Anino Fernández J, Mínguez Sánchez MD, de Lara Simón IM, et al. El modelo de autogestión en la agenda de consultas sucesivas en reumatología. Reumatol Clin. 2019;15:333–337.


