



The remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome was described by McCarty et al. in 1985.1 It refers to a clinical syndrome of unknown etiology which is often seen in older patients, characterized by acute and symmetric polyarthritis and intense edema of the hands and feet. It responds to low dose steroids and its prognosis is usually favorable. Therefore, it has traditionally been considered as a benign disease, although in the past few years it has acquired a certain importance when associated with other diseases, particularly neoplasia.
We present an RS3PE syndrome associated with a bladder carconoma, a little-known association.
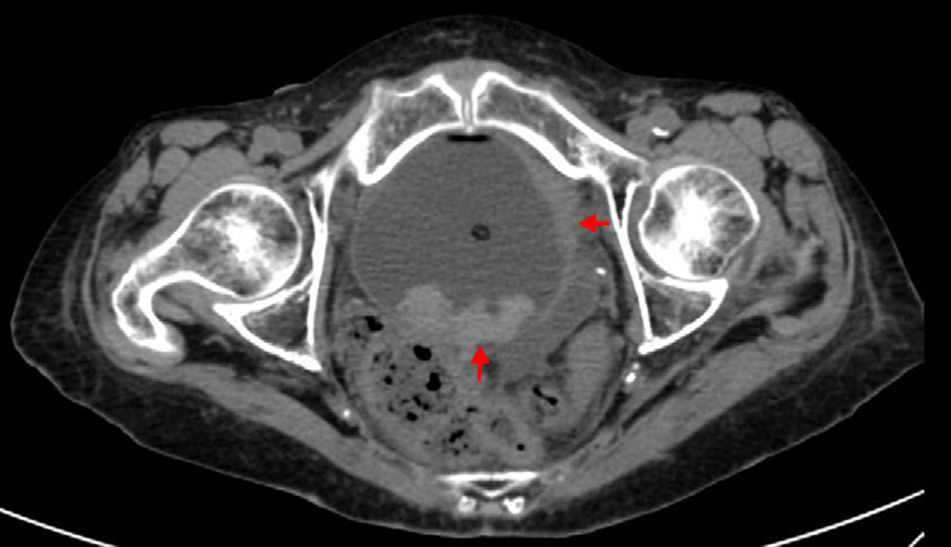
The patient, a 72-year-old woman with no history of interest, came to the rheumatology clinic due to nocturnal pain and morning stiffness of the hands and feet, which had been present for a month, accompanied by diffuse pitting edema and loss of function. She had no general symptoms, temporal arteritis, ulcers, uveitis or skin lesions. Laboratory showed an erythorsedimentation rate of 120mm, C reactive protein of 11mg/l and hemoglobin of 8.6mg/dl. Rheumatoid factor, anti-ctrullinated peptide antibodies and HLA B27 were all negative. No protein, immunoglobulin or 24 hour urine alterations were seen. Hand and feet X-rays found distal interphalangeal osteoarthritis of the hands and an increase in the opacity of soft tissue of the hands and feet. With this data and using the criteria proposed by los Olivo2 she was diagnosed with an RS3PE syndrome. Treatment was begun with prednisone (10mg/day), non-steroidal anti-inflammatory drugs and, after 4 weeks with little improvement, hydroxicloroquine (200mg/day), with progressive improvement. After 3 months symptoms had disappeared and acute phase reactants had returned to normal. Taking into account the possibility of a paraneoplastic syndrome, a chest X-ray was performed and was found normal, and an abdominal ultrasound done which revealed a bladder tumor confirmed using a thoraco-abdominal computed tomography (Fig. 1). A cystoscopy was performed and a biopsy obtained. Pathology reported a transitional cell carcinoma with infiltration of the bladder wall, with a bone scan that revealed no metastasis. From the rheumatology standpoint, the patient worsened. At a general level, the severe and rapid deterioration she showed contraindicated a radical cystostomy and the patient died 6 months after rheumatology reached its diagnosis.
The RS3PE syndrome appears more commonly in older patients.3 Its cause is unknown but some authors associate it with a genetic predisposition (HLA-B7 and HLA-A2), infectious agents, growth factors (vascular endothelial growth factor), or mediators such as interleukin 6 or tumor necrosis factors released by certain tumors.4 Acute phase reactants are usually increased and does not cause bone lesions observable in radiologic studies. The diagnosis is usually clinical and the criteria proposed by Olivo2: are usually applied: age >65 years, negative rheumatoid factor, symmetric arthritis which usually affects the wrists, metacarpophalangeal and proximal interphalangeal joints and extensor tendon sheaths of the hands, with “orange skin” pitting edema of the affected zones, morning stiffness, a rapid response to steroids and the exclusion of other diseases. The differential diagnosis must be done with other rheumatic diseases, mainly rheumatoid arthritis and late onset spondyloarthritis, polymyalgia rheumatica, temporal arteritis and chondrocalcinosis.5,6 Treatment is based on low dose steroids and, sometimes, antimalarial drugs.6 Its benign nature has recently been questioned and it has been associated to digestive tract, gynecologic, nephrourologic and hematologic malignancy.7,8 Rusell described, in the US, a greater incidence of cancer in these patients and recent publications indicate a higher than usual risk with respect to patients with similar characteristics.9,10 Therefore, we consider it important to systematically search for neoplasia when faced with this syndrome.
Please, cite this article as: Bruscas Izu C, et al. Síndrome RS3PE como primera manifestación de un carcinoma de vejiga. Cartas al Editor / Reumatol Clin. 2013;9:72–74.


