

To determine the impact of the disease in patients with PsA in daily clinical practice and to evaluate its relationship with its axial activity.
MethodsA cross-sectional study was conducted in consecutive patients attended from January 2021 to December 2021 who met the CASPAR criteria, with clinical of inflammatory back pain and positive axial imaging, with or without peripheral involvement. Demographic, clinical, analytical data, HAQ index, PsAID12 and activity index (BASDAI and ASDAS-PCR) were also collected. Patients were divided into two groups, those with high impact and those with low impact according to PsAID results. Continuous variables are shown as median (Q1–Q3) and categorical variables as percentages and frequencies.
ResultsOf the 269 patients evaluated with PsA, 72 patients with axial involvement were included, 40 men (55.6%), with a median age of 54.1 years and disease duration of 7 years. 28.3% of the patients were obese and serum CRP level was 0.45 mg/dl (0.08–1.10). BASDAI was 4.2 (2.0–6.2) and ASDAS-PCR was 2.4 (1.5–3.2), which translates into 39.6% of patients in low activity or remission. The median PsAID total score was 3.9 (1.6–5.4), evaluated in 61 patients. The patients who achieved a PsAID12 ≤ 4 were 63%, mostly men and with lower CRP levels than PsAID ≥ 4 patients. In addition, low impact measured by the PsAID12 was associated with low results in BASDAI and ASDAS-PCR.
ConclusionsAxial involvement reflected lower impact of the disease measured by PsAID12 and it is correlated with low activity measured by BASDAI and ASDAS-PCR.
Determinar el impacto de la enfermedad en pacientes con artritis psoriásica (APs) en la práctica clínica diaria, y evaluar su relación con la actividad axial.
MétodosSe realizó un estudio transversal multicéntrico en pacientes consecutivos vistos desde enero 2021 hasta diciembre 2021 que cumplieron con los criterios CASPAR, con clínica dolor lumbar inflamatorio y prueba de imagen positiva, con o sin afectación periférica. También se recogieron datos demográficos, clínicos, analíticos, índice Health Assessment Questionnaire, PsAID12 e índices de actividad axial (BASDAI y ASDAS-PCR). Se dividió a los pacientes en 2 grupos según el alto o bajo impacto del cuestionario PsAID. Las variables continuas se mostraron como mediana (Q1–Q3) y las categóricas como porcentajes y frecuencias.
ResultadosSe incluyeron 72 pacientes con afectación axial de los 269 evaluados con APs, 40 varones (55,6%), con una mediana de edad de 54,1 años y duración de la enfermedad de 7 años. El 28,3% de los pacientes eran obesos y el nivel sérico de PCR fue de 0,45 mg/dl (0,08–1,10). El BASDAI fue de 4,2 (2,0–6,2) y el ASDAS-PCR de 2,4 (1,5–3,2), estando en baja actividad o remisión el 39,6%. La mediana de la puntuación total de PsAID fue de 3,9 (1,6–5,4), evaluado en 61 pacientes. Los pacientes que alcanzaron un PsAID12 ≤ 4 fueron el 63%, predominantemente varones, presentaron valores de PCR menores y se asoció a una menor puntuación de BASDAI y ASDAS-PCR.
ConclusionesLos pacientes con afectación axial reflejaban un bajo impacto de la enfermedad medido por PsAID12 y este se correlacionaba con baja actividad medido por BASDAI y el ASDAS-PCR.
Psoriatic arthritis (PsA) is an inflammatory disease within psoriatic diseases with diverse clinical manifestations which affect the quality of life of patients.1
Estimates of the worldwide prevalence of PsA range from 0.05% to 0.25% in the general population, and more than 30% of patients with cutaneous psoriasis have PsA. This percentage may be higher, as between 5% and 15.5% may go undiagnosed, as well as the fact that there may be a diagnostic delay of 6 months from the onset of symptoms.2,3
Its key domains are cutaneous and nail psoriasis, peripheral arthritis, axial disease, enthesitis and dactylitis, leading to bone damage, deformity and dysfunction.4
Axial involvement typically manifests as inflammatory low back pain (LBP). Accompanying these clinical symptoms are inflammatory structural changes that are manifested radiologically, both in the spine and the sacroiliac joints, with the combination of these two providing us with a diagnosis. Occasionally, this association may appear sub clinically or not be reported, so it is necessary to actively seek this in the patient interview.3,5
The high prevalence of the disease, as well as the clinical symptoms and delayed diagnosis reveal a major impact on the patient’s health. The PsA Impact of Disease (PsAID) questionnaire was developed to assess patients’ perspective on the disease in 12 domains, both physical and psychological, including pain, fatigue, work impairment or feelings of anxiety, depression, sleep disturbances or embarrassment,6 with scores associated with the importance of the effect of each on the patient. It is expected that the impact of the disease will improve (lower scores) when the patient is in remission or has low disease activity.
The main objective of this study was to determine the impact of the disease in a cohort of patients, measured through PsAID12, with axial involvement, and whether this impact was related to axial activity indices in clinical practice.
MethodsA multicentre, observational cross-sectional study was carried out in patients from a regional psoriatic arthritis register (SUEIRO register), seen consecutively in surgery visits from January 2021 to December 2021, who met CASPAR criteria for PsA,7 with clinical signs of non-specific low back pain and changes in imaging techniques at the axial level, both on plain radiography and positive magnetic resonance imaging (X-ray/MRI). All imaging tests run were assessed by the radiology department, and patients with possible confounding factors such as spondylarthrosis and Forestier’s disease were excluded. Patients could have peripheral involvement or otherwise and were treated according to clinical practice guidelines using the latest SER/EULAR recommendations.8,9
Demographic data were collected, including age, patient sex, body mass index (BMI; kg/m2), duration of disease measured in years, clinical symptoms, concomitant presence of fibromyalgia, laboratory parameters (CRP [mg/dl]), indices of disease activity both cutaneous by BSA and BASDAI, plus ASDAS-PCR for axial activity, the HAQ index (0–3) and PsAID12 (0–10).
Patients were divided into 2 groups: those with a PsAID above 4 (high impact) or below 4 (low impact).
Continuous variables were shown as median and interquartile range (IQR, Q1–Q3) and categorical variables as percentages and frequencies. Their normality adjustment was tested using the Kolmogorov–Smirnov–Lilliefords test. To determine whether there was an association between variables, classic bivariate analysis tests were run. In the case of categorical variables, the Chi-square test was used, and if not figuring in its use cases, the Fisher’s exact test. For continuous variables, Student’s t-test was used when the assumptions of use were met and, in its absence, the Mann–Whitney U test. All analyses were run using SPSS®23 software. Differences were considered statistically significant if p < 0.05.
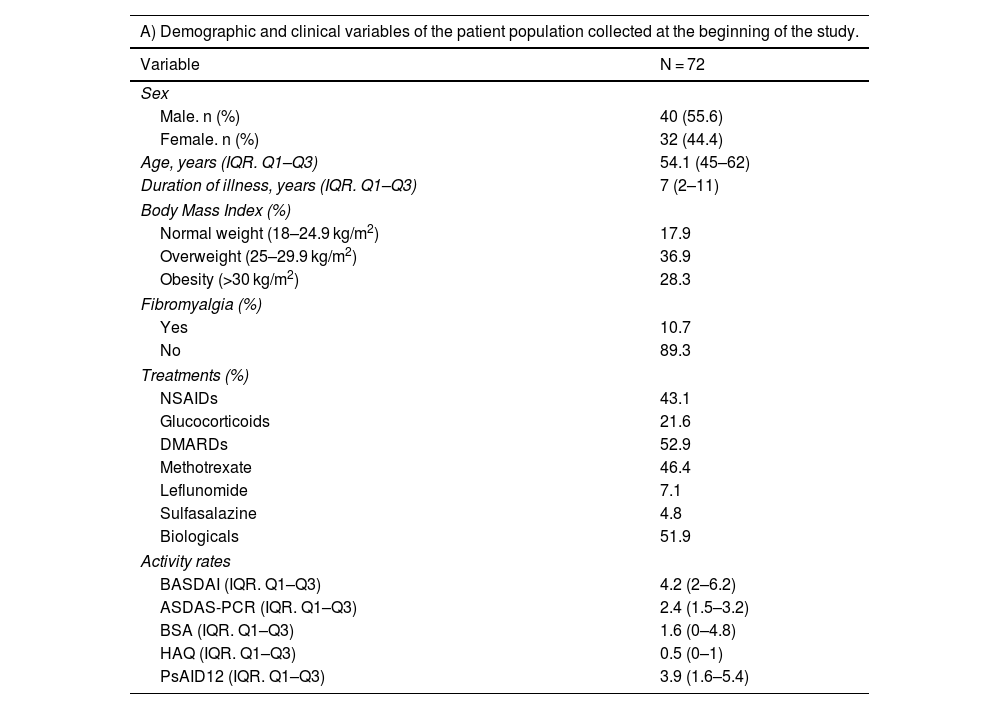
ResultsA total of 72 patients with axial involvement were included (Table 1A). Of these, 40 patients were male (55.6%) and 32 female (44.4%), with a median age of 54.1 years (IQR: 45.0–62.0) and a median duration of disease of 7 years (IQR: 2–11). Patients with normal weight accounted for 17.9% of the cases, 36.9% were overweight and 28.3% were obese. The mean serum CRP level was 0.45 mg/dl (IQR: 0.08–1.10). The treatments received by the patients were: NSAIDs (43.1%), glucocorticoids (21.6%), DMARDs (52.9%, the most frequent being methotrexate [46.4%], followed by leflunomide [7.1%] and sulfasalazine [4.8%]), and biological therapy (51.9%). A total of 10.7% of patients had a diagnosis of fibromyalgia in their medical history.
Clinical-epidemiological characteristics of patients with psoriatic arthritis included in the study.
| A) Demographic and clinical variables of the patient population collected at the beginning of the study. | |
|---|---|
| Variable | N = 72 |
| Sex | |
| Male. n (%) | 40 (55.6) |
| Female. n (%) | 32 (44.4) |
| Age, years (IQR. Q1–Q3) | 54.1 (45–62) |
| Duration of illness, years (IQR. Q1–Q3) | 7 (2–11) |
| Body Mass Index (%) | |
| Normal weight (18–24.9 kg/m2) | 17.9 |
| Overweight (25–29.9 kg/m2) | 36.9 |
| Obesity (>30 kg/m2) | 28.3 |
| Fibromyalgia (%) | |
| Yes | 10.7 |
| No | 89.3 |
| Treatments (%) | |
| NSAIDs | 43.1 |
| Glucocorticoids | 21.6 |
| DMARDs | 52.9 |
| Methotrexate | 46.4 |
| Leflunomide | 7.1 |
| Sulfasalazine | 4.8 |
| Biologicals | 51.9 |
| Activity rates | |
| BASDAI (IQR. Q1–Q3) | 4.2 (2–6.2) |
| ASDAS-PCR (IQR. Q1–Q3) | 2.4 (1.5–3.2) |
| BSA (IQR. Q1–Q3) | 1.6 (0–4.8) |
| HAQ (IQR. Q1–Q3) | 0.5 (0–1) |
| PsAID12 (IQR. Q1–Q3) | 3.9 (1.6–5.4) |
| B) Characteristics of the population with axial PsA that had performed PsAID12 | |
|---|---|
| Variable | N = 61 |
| Test the Schober (median (Q1–Q3) | 4.5 (4.1–4.6) |
| Sacroiliac involvement in plain radiology | 24 (39.3%) |
| Symmetrical | 16 (66.6%) |
| Asymmetricala | 8 (33.3%) |
| Involvement in NMRb | 12 (19.6%) |
| Vertebral | 4 (33.3%) |
| Sacroiliac | 8 (66.6%) |
NSAIDs: nonsteroidal anti-inflammatory drugs; PsA, psoriatic arthritis; IQR, interquartile range; NMR, nuclear magnetic resonance imaging.
The median BASDAI calculated from the sample was 4.2 (IQR: 2.0–6.2) and the median ASDAS-CRP was 2.4 (IQR: 1.5–3.2), with 39.6% in low activity or remission. The median BSA was 1.6% (IQR: 0–4.8) and the median HAQ was 0.5 (IQR: 0–1). The PsAID questionnaire was evaluated in 61 patients, with a median total score of 3.9 (IQR: 1.6–5.4). The characteristics of metrology and axial involvement in this population that had done PsAID12 are shown in Table 1B. There was no significant correlation between PsAID12 and the Schober test (r: 0.186; p = −0.144) or the mSASSS radiographical damage index (r: 0.202; p = −0.143). Patients who achieved a PASS state and those who did not differed significantly in terms of the degree of sacroiliitis (p = 0.256), Schober’s test (p = 0.548) or mSASSS (p = 0.155).
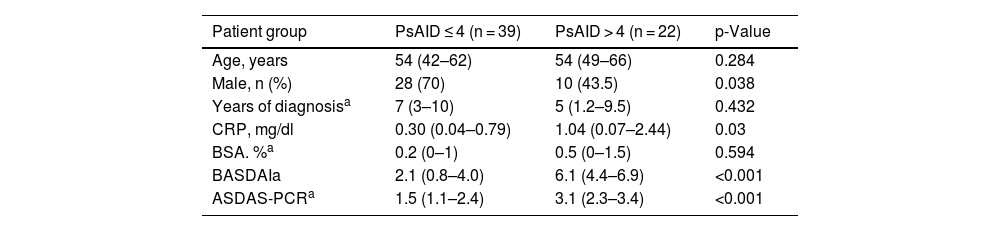
Patients who achieved a PsAID12 ≤ 4 totalled 63% (Table 2); more were males (70% vs. 43.5%; p = 0.038) and with a lower CRP (0.30 vs. 1.04 mg/dl; p = 0.03). In addition, the low impact measured by PsAID12 was associated with lower BASDAI (2.1 vs. 6.1; p < 0.001) and ASDAS-PCR (1.5 vs. 3.1; p < 0.001) compared to those with PsAID > 4 values, with no statistically significant differences found, and with the extent of skin involvement measured by BSA (p = 0.594), disease duration (p = 0.432) or age of patients (p = 0.284).
Comparison of variables in patients, based on PsAID results.
| Patient group | PsAID ≤ 4 (n = 39) | PsAID > 4 (n = 22) | p-Value |
|---|---|---|---|
| Age, years | 54 (42–62) | 54 (49–66) | 0.284 |
| Male, n (%) | 28 (70) | 10 (43.5) | 0.038 |
| Years of diagnosisa | 7 (3–10) | 5 (1.2–9.5) | 0.432 |
| CRP, mg/dl | 0.30 (0.04–0.79) | 1.04 (0.07–2.44) | 0.03 |
| BSA. %a | 0.2 (0–1) | 0.5 (0–1.5) | 0.594 |
| BASDAIa | 2.1 (0.8–4.0) | 6.1 (4.4–6.9) | <0.001 |
| ASDAS-PCRa | 1.5 (1.1–2.4) | 3.1 (2.3–3.4) | <0.001 |
PsAID: Psoriatic Arthritis Impact of Disease.
Finally, patients diagnosed with fibromyalgia had PsAID12 values above 4 compared to those without a diagnosis (p = 0.015).
DiscussionThe axial involvement of psoriatic arthritis is sometimes asymptomatic and its diagnosis is reached in many cases by an active search motivated by high suspicion, unlike in ankylosing spondylitis, where low back pain is the first symptom for which the patient is referred to rheumatology consultations.10 In this regard, its diagnosis in routine clinical practice is not always easy.11
On the other hand, some studies have observed a relationship between axial involvement and earlier age of onset of the disease, greater presence of enthesitis, increased extent of skin involvement, depression, and the early need for biological treatment, when compared to exclusively peripheral joint involvement.12,13
Although these are 2 different conditions, in genetics and clinical and radiological findings,14 activity indices designed for ankylosing spondylitis are used in the assessment of axial involvement of psoriatic arthritis, making it difficult in clinical practice to use instruments that cover the broad spectrum of disease.15–17
The PsAID questionnaire was designed to assess quality of life and functionality from the perspective of patients with PsA,18 and has a solid basis and wide use as an assessment instrument in clinical trials.15 This data is evaluated mainly on peripheral involvement,19,20 with less information on the use of this index in axial involvement.
In our study, the data obtained from PsAID was correlated with data on disease activity, measured by both BASDAI and ASDAS and with the change in inflammatory parameters (measured by serum CRP levels), although no association with patient age or years of disease duration, etc. was confirmed, nor with the severity of skin involvement. These results are consistent with other published studies,21,22 where the results obtained from BASDAI and ASDAS were adjusted with the patient’s perception measured by PsAID and correlated with disease activity.
On the other hand, the presence of comorbidities can negatively affect the patient’s subjective perception of their disease, which may be reflected in the worsening of some indices, regardless of the activity of the psoriatic disease itself and the response to treatment. One of these comorbidities is fibromyalgia. In our study, although it was not included as the main objective, we found a greater impact of the disease in those patients diagnosed with fibromyalgia, compared to those who did not present this diagnosis. Lubrano et al. conducted a study on the impact of comorbidities, which supported their influence on disease control, therapeutic decisions, and strategies to be followed.23 Some comorbidities such as anxiety and fibromyalgia influence the measurement indices (DAPSA and PsAID) and these affect our decision-making in clinical practice.
Another potentially impactful factor is gender. In our sample, we found differences in PsAID values according to sex, so that a lower impact of the disease was confirmed in the male group, which is consistent with the results obtained in other studies.24
The results of this study support the use of the PsAID questionnaire not only in patients with PsA with peripheral or mixed involvement but they also confirm its usefulness in cases with axial involvement by demonstrating that there is a relationship between the findings obtained from axial activity indices (both BASDAI and ASDAS-PCR) and the patient’s perceived impact of their disease.
The limitations of this study derive from the cross-sectional and observational nature of its design, so it would be necessary to validate these findings in more studies with designs aimed at specifically exploring these results.
ConclusionsThe results of this study show that there is a relationship between axial activity indices measured by BASDAI and ASDAS-PCR and the impact of the disease perceived by the patient, as measured by PsAID. The use of PsAID in PsA patients with axial involvement could provide relevant information from the point of view of the patient’s perception.
Ethical responsibilitiesThe source register, code 2015/671, was approved by committee and patients signed informed consent for inclusion.
FundingNone of the authors received financial support or any other benefits from commercial sources for the work reported in this manuscript.
AuthorshipAll authors contributed equally to this research.
Conflict of interestThere are no conflicts of interest in the production of this article.
The authors would like to thank the Galician Research Group on Psoriatic Arthritis and the Galician Society of Rheumatology for their advice in the design and review of the article. The authors are grateful for the assistance in medical writing provided by Medical Statistics Consulting S.L. (Valencia, Spain), within a PUBLIBECA programme.


