







Currently there are no clinimetric instruments for the measurement of the severity of iatrogenic Cushing's syndrome (ICS). Sonino et al. created a clinical severity index of endogenous Cushing’s disease (CSI) but it has not been applied to patients with ICS.
ObjectiveTo validate and determine the utility of the CSI and its correlation with clinical variables in rheumatological patients with continuous use of glucocorticoids (GC).
Subjects and methodspatients with a history of continuous systemic GC use (for at least 4 weeks) indicated for treatment of rheumatological disease were included. All the patients filled out a questionnaire on sociodemographic data, characteristics of the CG used; the way of use and the presence or absence of adverse events. The CSI was applied by 2 observers independently. Consistency, interobserver concordance and principal component analysis were calculated.
Results32 patients with an average age of 35.72 ± 12.8 years were studied; 29 were women (90.6%). The average CSI score by the first observer was 3.50 ± 2.02, and by the second observer was 2.31 ± 1.75 (P = .004). The interobserver concordance was low in the items with imprecise definitions; for which modifications were made in the definitions to improve their performance. The CSI scores correlated with the presence of adverse effects and the type of dose used.
ConclusionsThe CSI has an adequate correlation with clinical manifestations in patients with chronic use of GC. The clinimetric characteristics of the questionnaire improved by standardising the definitions of subjective clinical variables.
Actualmente no se cuenta con instrumentos clinimétricos para la medición de la gravedad del síndrome de Cushing iatrógeno (SCI). Sonino y cols crearon un índice clínico de gravedad de Cushing endógeno (IGC) pero no ha sido aplicado a pacientes con SCI.
ObjetivoValidar y determinar la utilidad del IGC y su correlación con variables clínicas en pacientes reumatológicos con uso de glucocorticoides (GC) de forma continua.
Sujetos y métodosSe incluyó a pacientes con antecedentes de uso de GC sistémicos de forma continua indicados para el tratamiento de la enfermedad reumatológica, por lo menos durante 4 semanas. Todos los pacientes llenaron un cuestionario sobre datos sociodemográficos, características de los GC empleados; la forma de uso y la presencia o ausencia de eventos adversos. Se aplicó el IGC por 2 observadores de forma independiente. Se calculó la consistencia, la concordancia interobservador y un análisis de componentes principales.
ResultadosSe estudió a 32 pacientes con edad promedio de 35,72 ± 12,8 años; 29 eran mujeres (90,6%). La calificación promedio del IGC por el primer observador fue de 3,50 ± 2,02, y del segundo observador fue de 2,31 ± 1,75 (p = 0,004). La concordancia interobservador fue baja en los ítems con definiciones imprecisas, por lo cual se hicieron modificaciones en las definiciones para mejorar su desempeño. Los puntajes del IGC correlacionaron con la presencia de efectos adversos y el tipo de dosis utilizada.
ConclusionesEl IGC tiene una adecuada correlación con manifestaciones clínicas en pacientes con uso crónico de GC. Las características clinimétricas del cuestionario mejoraron al estandarizar las definiciones de variables clínicas subjetivas.
Iatric Cushing’s syndrome (ICS) is caused by chronic exposure to excess synthetic glucocorticoids (GC) which inhibit the function of the hypothalamus-pituitary-adrenal gland axis.1 Symptoms are multisystem and signs and symptoms appear progressively, depending on usage time and dose. The most frequent clinical manifestations are central obesity (90%), which affects the face, neck, trunk and abdomen and causes “full moon face” and “buffalo hump”. Bruises may appear on the skin (35%), acne (35%), stretch marks (50%) and hirsutism (75%). High blood pressure may develop in 85% of cases, intolerance to glucose in 75% and diabetes in 20%. Patients may develop osteoporosis, proximal myopathy and neuropsychiatric changes.1–3
At present there are no clinical tools for the measurement of the seriousness of ICS. Sonino et al. created a clinical index of endogenous Cushing severity (Cushing’s syndrome severity index or CSI). This index includes 8 items which are classified from 0 to 3, with a score of 0–16.4 The grading of clinical signs is based on the physician’s judgement and experience. Validation was made in 14 patients with endocrine Cushing’s syndrome, assessed independently by 2 endocrinologists before and after treatment. The average score obtained prior to treatment was 8.5 ± 2.7 (observer 1) and 8.4 ± 2, 8 (observer 2) and after treatment 1.9 ± 1.6 for both observers (P < .001) in both cases. The interobserver concordance measured by Kappa was .45 (skin) to 1.00 (blood pressure, diabetes mellitus and hypopotassaemia). The intraclass correlation coefficient was .95 prior to treatment and .87 after, with appropriate post-treatment discrimination (P < .001). The CSI correlated with the urinary cortisol level and with 2 global scales: one of severity and another of change to treatment measured by the physician. This tool has not been used in patients with ICS, and the clinimetric characteristics in this patient group are therefore unknown although it is expected they would be similar to patients with endogenous Cushing’s syndrome.
The aim of this study was to validate and determine the usefulness of the CSI and its correlation with clinical variables in rheumatologic patients with continuous GC use.
Subjects and methodsThe direct transition into Spanish of the CSI was made by 2 bilingual translators whose mother tongue was Spanish. After this, one of the translations was chosen at the consensus meeting based on linguistic and semantic equivalence. Following this, an inverse translation was made by a bilingual translator whose mother tongue was English, with no previous knowledge of the instrument and this translation was compared with the original. In a consensus meeting the versions to be used in this study were chosen (Appendix I).
Patients with rheumatologic diseases were selected over a period of 6 months. Patients were both hospitalized and outpatients. Patients over 18 years of age who agreed to participate in the study were included. They had a background of continuous systemic GV use for the treatment of their rheumatologic disease, or through self-prescription, for at least 4 weeks and they were grouped together based on the GC dose: low if they were on ≤7.5 mg of prednisone, intermediate dose if they were on >7.5 and up to 30 mg of prednisone per day and high doses which were above 30 mg per day.5 All patients were given a questionnaire by an interviewer which encompassed sociodemographic data, and the characteristics of the GC used, the form of use and the presence or absence of adverse events.
Daily and accumulated doses of prednisone or an equivalent were calculated in milligrams. To assess interobserver concordance, 2 observers applied the CSI independently on the same day as the patient attended consultation. Serum cortisol was measured in all patients on an empty stomach by chemiluminescence, with reference values of 50–250 ng/ml. Quality of life was measured in everyone with the EuroQoL 5D, with a patient global health visual analogue scale from 0 to 100.
Modifications to the Cushing’s syndrome severity indexClinical variables such as central obesity, skin changes and muscle weakness were redefined and instead of using non-objective classification through appreciation of the observer, more objective definitions were created.
In item 1 (fat distribution) it was decided that the waist/hip index would be used as a measurement of central obesity.6 Normal values were considered to be .95 in men and .85 in women; mild central obesity was .95–1.0 in men and .85–.90 in women and marked central obesity were values of >1.0 in men and .95 in women. The existence of full moon face was considered an aggravation which increased one point in the normal categories (0), mild/moderate (1) and with no changes in the serious categories (2). In item 2 (skin lesions) it was decided that the rule of 9, used on burns,7 was to be applied arbitrarily to determine the extension of the lesions, and it was considered that ≤18% involvement of the body area was mild involvement and >18% was severe involvement. In item 3 (muscle weakness) the Daniels scale of muscle strength was used in which the absence of contraction is 0, contraction without movement is 1, active movement in favour of gravity is 2, active movement which defies gravity and partial resistance is 4 and normal strength is 5. In the index the absence of muscle weakness was considered (grade 5), mild/moderate muscle weakness (grades 3–4) and severe muscle weakness (grades 0–2). The remaining items were maintained without changes (Appendix II).
For statistical analysis, descriptive statistics were used and central tendency and dispersion measures were calculated (standard means and deviation for numerical variables and frequencies for categorical and nominal variables). For comparisons the χ2 or Wilcoxon test was used for the non-parametric variables and the Student’s t-test or ANOVA test for numerical variables. Statistical significance was considered as under .05. For interobserver concordance Kappa was used for the items and intraclass correlation coefficiency for global qualification. The homogeneity between the items was measured with Cronbach’s α. The main components analysis was performed using the Kaiser–Meyer–Olkin statistics and ortogonal (varimax) and oblique (promax) rotations were used to determine the uni or multi-dimensionality of the index.
ResultsThe study involved 32 patients with average ages of 35.72 ± 12.8 years, 29 of whom were women (90.6%). The average level of education was 10.94 ± 3.66 years. The main rheumatologic diagnoses were: systemic lupus erythematosus in 14 patients (43.8%), rheumatoid arthritis in 9 (28.1%), primary vasculitis in 4 (12.5%), gout in 3 (9.4%), human modelants disease in one (3.1 %) and painful shoulder syndrome in one patient (3.1%). The average score on the EuroQoL 5D was .83 ± .21. The global health VAS measured by the patients was 72.4 ± 23.7 mm.
Glucocorticoid usage characteristicsThe main GC used (some more than others) were prednisone in 23 patients (71.9%), dexamatasone in 6 patients (18.8%), betametasone in 5 (15.6%), deflazacort in 2 (6.3%), intravenous methylprednisolone in 6 (18.8%) and parametasone in 3 (9.3%). The main administration route of the GC was oral in 20 patients (62.5%), in 3 it was intramuscular (9.4%) and in 9 patients (28.1%) the GC were administered through combined routes (oral and intramuscular or intravenous). Usage time median of GC was 7.85 (1.50–144 months). The median daily dose was 19 (.23–665) mg/day. The median of accumulated GC dose was 4,962.5 (170−54,000) mg.
Based on the daily dose of prednisone or the equivalent, patients were divided into 3 groups. The low dose group (n = 10) had an average intake of .89 ± 2.11 mg/day. The medium dose group (n = 11), had an average intake of 16.67 ± 6.03 mg/day. Finally, in the high dose group (n = 11), average intake was 184.66 ± 240.9 mg/day (P = .010).
Usage reason shown by the patient was for disease activity based on 20 cases (62.5%) and for pain in the others.
Only 11 patients (34.4%) prescribed with GC by the doctor were informed about possible adverse effects. After evaluation by the doctor, secondary adverse effects from the use of GC in 28 patients (87.5%) were reported, and with a median of 2 (1–7) adverse effects (Fig. 1).
In 12 patients (37.5%) a sudden withdrawal from treatment with GC was reported and, of these patients 8 (67%) reported manifestations of suppression.
The average value of cortisol in the group of low doses was 38.45 ± 123.78 ng/mL and in the medium to high doses it was 9.6 ± 9.6 ng/mL (P < .000). Serum cortisol was correlated with the accumulated GC dose (r = .75; P = .013).
Results of the application of the Cushing’s syndrome severity indexThe average CSI score by the first observer was 3.50 ± 2.02 and by the second observer it was 2.31 ± 1.75 (P = .004).
Cronbach’s α of the 8 CSI items of the first observer was .53 and was .42 for the second observer. The intraclass correlation coefficient of the global score of both observers was .895. Table 1 contains several items which were eliminated and could have improved the global consistency of the index, and therefore could have been redundant.
Consistency of the Cushing’s syndrome severity index.
| CSI items | Cronbach’s alfa if element eliminated | Cronbach’s alfa if element eliminated |
|---|---|---|
| Observer 1 | Observer 2 | |
| Fat distribution | .312 | .297 |
| Skin lesions | .439 | .292 |
| Muscle weakness | .504 | .481 |
| Mood disorders | .456 | .491 |
| Hypertension | .583 | .479 |
| Diabetes | .402 | .337 |
| Hypokalaemia | .550 | .459 |
| Sexual changes | .608 | .499 |
| Total Cronbach’s alpha | .531 | .424 |
CSI: Cushing’s syndrome severity index.
Average scores and interobserver concordance of each of the items from the CSI and statistical significance, are described in Table 2.
Interobserver variability of the CSI.
| CSI | |||||
|---|---|---|---|---|---|
| Item | Observer 1 | Observer 2 | P | Kappa | Kappa with modifications |
| Mean (SD) | Mean (SD) | ||||
| 1 | .84 (.85) | .78 (.87) | .423 | .707 | .54 |
| 2 | .84 (.57) | .59 (.67) | .018 | .375 | .81 |
| 3 | .06 (.25) | .13 (.34) | .325 | .273 | .80 |
| 4 | .75 (.44) | .19 (.40) | .000 | .048 | 1.00 |
| 5 | .16 (.52) | .16 (.52) | 1.0 | 1.0 | 1.00 |
| 6 | .16 (.37) | .16 (.37) | 1.0 | 1.0 | 1.00 |
| 7 | .03 (.18) | .03 (.18) | 1.0 | 1.0 | 1.00 |
| 8 | .59 (.67) | .44 (.56) | .057 | .772 | .82 |
| Total | 3.50 (2.02) | 2.31 (1.75) | .000 | .132 | .55 |
CSI: Cushing’s syndrome severity index.
Items 2 and 4 were those with the lowest concordance.
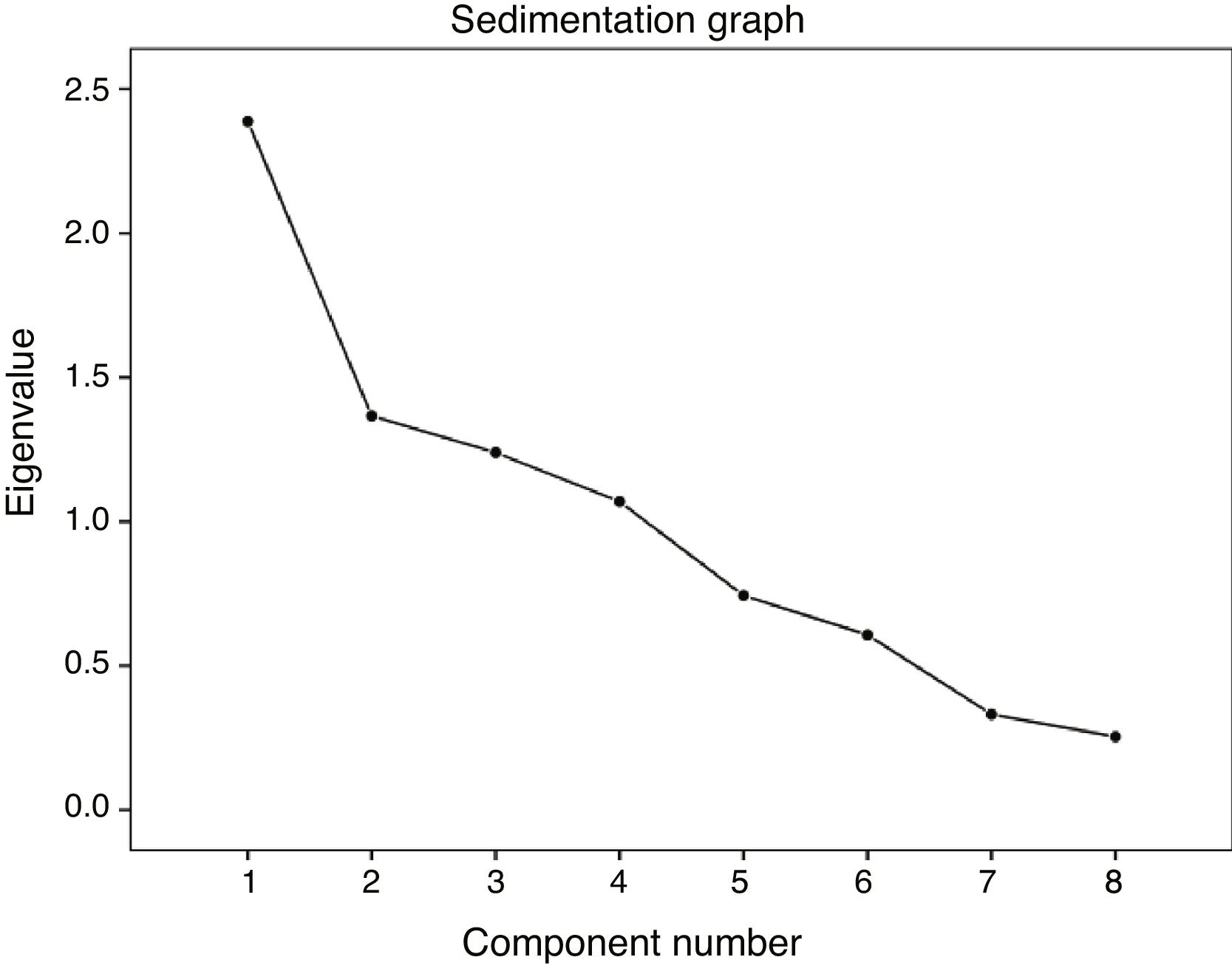
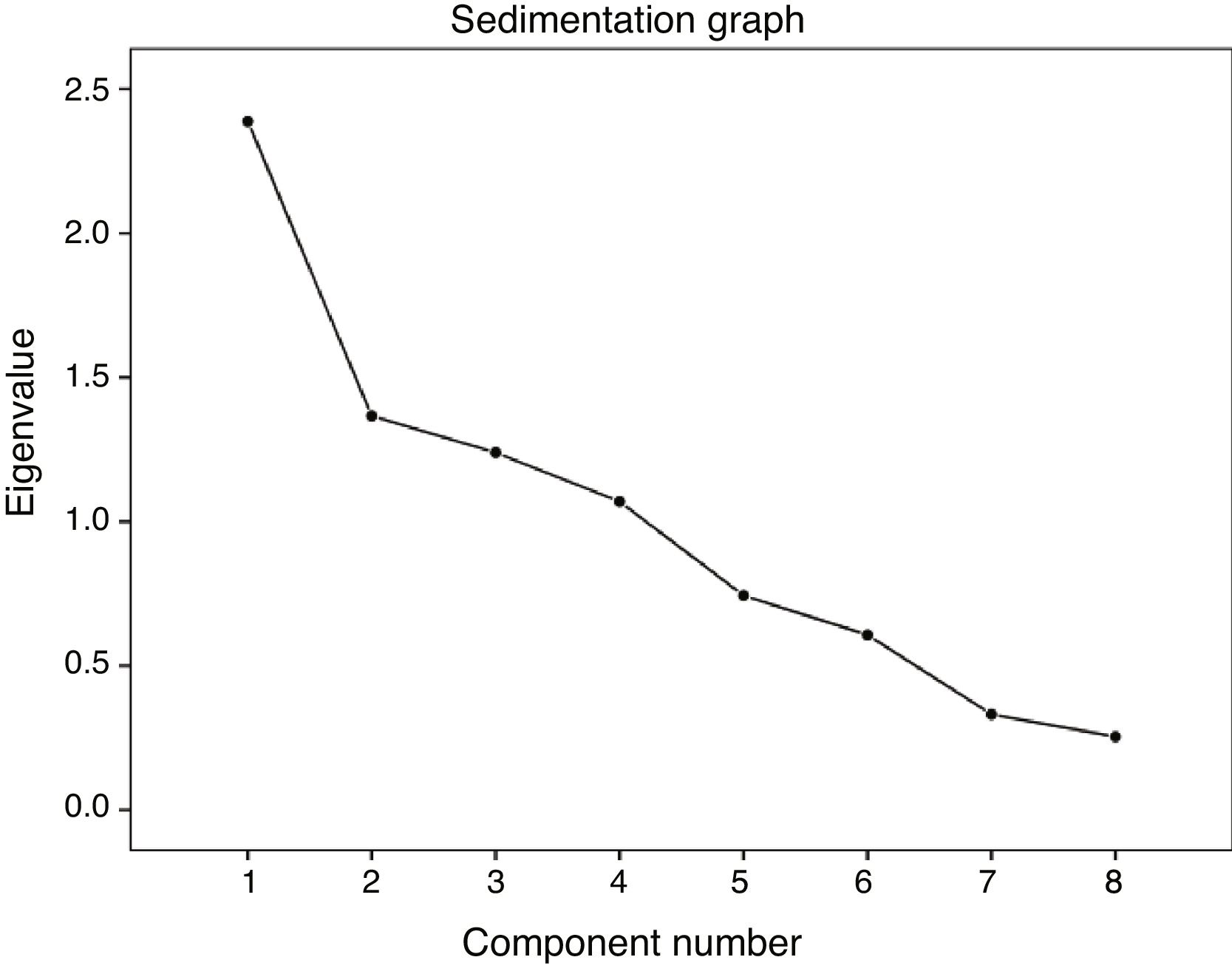
In the analysis of the main components we found 4 components which explained the 75.8% variability (Fig. 2). The matrix of components and rotations positioned items 1, 2 and 6 in the first component; items 3 and 5 in component 2; items 4 and 7 in component 3 and item 8 in component 4.
On stratifying patients by GC dose used, we observed that patients who used higher doses had higher CSI scores than those on low or medium doses. We also observes there to be a tendency for significantly higher scores from the first researcher compared with the second (Table 3).
The CSI scores correlated inversely with the EuroQoL5D with r = −.50 (P = .015), but did not correlate with the global health VAS of the patient nor with cortisol levels, daily dose, accumulated dose or usage time. They did correlate with the presence of adverse effects and the type of dose used (Table 4).
Correlation of the CSI with variables related to the use of glucocorticoids and the presence of adverse effects.
| Characteristic | CSI observatory 1 r(p) | CSI observatory 2 r (p) |
|---|---|---|
| Daily dose | .30 (.10) | .30 (.11) |
| Accumulated dose | .22 (.25) | .32 (.08) |
| Usage time | .16 (.40) | .13 (.49) |
| Type of dose | .49 (.006) | .55 (.002) |
| Number of adverse effects | .70 (.000) | .61 (.000) |
| Presence of adverse effects | .44 (.000) | .32 (.088) |
CSI: Cushing’s syndrome severity index.
Effects of the modifications: the modified CSI had average scores of 3.30 ± 2.5. Cronbach’s α improved to .68 and the interobserver concordance also improved considerably (Table 2). With these modifications, main component analysis was reduced to 3 components which explains the variance of 69.36%. The first component contained items 3, 5, 6 and 7; component 2 contained items 1, 2 and 8 and finally component 3 only contained item 4.
DiscussionPatients with rheumatologic diseases frequently use GC due to its anti-inflammatory and immunomodulatory effect. It has been estimated that GC are used chronically in .5%–1% of the general population and in 2.5% of older adults8 and that it is prescribed in over 50% of patients with rheumatoid arthritis or systemic lupus erythematosus. The undesirable effects of GC use are related to dose; treatment duration; changes in metabolism and speed of drug excretion; hypoalbuminaemia and possibly idiosyncratic factors, although few studies exist in this regard.9–11 One of the adverse effects associated with GC use is the ICS, which presents in a high percentage of patients in treatment with these drugs. Despite frequency there are no clinimetric tools for its evaluation.
The CSI was created to assess response to treatment in patients with endogenous Cushing’s syndrome, and its usefulness in this patient group has been demonstrated,4 although it had not been applied in patients with ICS.
On applying this index in patients with chronic GC usage (without demonstrating the inhibition of the hypothalamus-pituitary-adrenal gland axis, since only the serum cortisol could be measured but not ACTH) an average score of 3.50 ± 2.02 was found in the first observer and of 2.3 ± 1.75 in the second observer, lower figures than those reported by Sonino et al.,4 the average scores of which were 8.5 ± 2.7 and 8.4 ± 2.8 for the first and second observer, respectively, which could be justified by the fact that these patients had rampant Cushing’s syndrome and in our case not all patients had characteristic facies and they were only included based on their background of GC usage.
Similarly to the initial evaluation of this tool by its authors, we determined a prefect interobserver concordance (kappa 1) in the laboratory variables, including hyperglycaemia and hypercalcaemia as well as in the determination of high blood pressure, although in our study the interobserver concordance in more subjective variables such as skin lesion, fat distribution, changes to behaviour or sexual changes was lower (.048–.375) than that reported by Sonino et al. (.45–.61). The possible explanation for this phenomenon is that these variables do not have a strict definition and are objectively classified by the physician. When definitions change, the kappas of these items improve significantly, as does global Cronbach’s α. The main component analysis demonstrated that this was not a one-dimensional index since it was formed by 4 components in its original version and by 3 components in its modified version.
Adequate correlation was not found between the CSI score with cortisol levels, daily dose, accumulated dose and GC usage time, but it was found in the type of dose used (high, medium or low) and significant differences were even found in the CSI score between those who used high doses and those who used low and medium doses. There was also adequate correlation between CSI and the presence and number of adverse effects, although this was expected, since CSI items were stratified adverse effects based on their severity.
With regard to the presence of adverse effects, these were reported in 93.3% of our sample, a similar figure to that reported in a population study with GC use at low doses for ≥60 days which included 2446 people, with an average daily dose of prednisone or equivalent of 16 ± 14 mg and they reported that 90% of patients had at least one associated adverse effect.8
Some of the limitations of our study are the fact that the ACTH levels in our patients were not measured to demonstrate inhibition of the hypothalamus-pituitary-adrenal gland axis and no correlation of the CSI score with this variable was therefore possible. Also no purposeful search was made of adverse effects such as the use of bone densitrometry or ophthalmological review. The heterogeneity of the diseases studied and the use of different glucocorticoids and administration routes may also have weighted study results. The main objective was to validate the tool to be able to use it on a larger population to obtain better outcomes and even use it prospectively to assess sensitivity to the change of the CSI.
ConclusionsCSI has an adequate correlation with clinical manifestations in patients with chronic GC use. The questionnaire improved when the definitions of subjective clinical variables were standardised, and this version is therefore recommended. It is a simple index with good reproducibility which may be useful in the assessment of patients with ICS.
FinancingNone of the authors received financial support or other benefits from commercial sources for the study documented in this manuscript.
The following is Supplementary data to this article:

Please cite this article as: Álvarez-Hernández E, Mercado-Molina G, Barrera-Guerra RC, Validación del índice de gravedad del síndrome de Cushing en pacientes con síndrome de Cushing iatrógénico. Reumatol Clin. 2021;17:313–317.


