







The Colegio Mexicano de Reumatología (CMR) is a corporation whose brand has two elements—image and identity—that differentiate it from other corporations. We evaluated aspects of CMR's corporate image and identity.
Subjects and methodsTo assess corporate image, we designed a survey using proof-of-concept and discrete-choice-experiments approaches. It assessed which definition (orthopedist, rheumatologist, or rehabilitator) was most meaningful in four pain scenarios in healthy adults from the country's Western region.
We used discourse analysis and five readability indices of the CMR website to assess corporate identity.
ResultsIn total, 700 respondents were included. For every rheumatologist chosen in the hand scenario, respondents chose 1.13 orthopedists and 0.70 rehabilitators. For every rheumatologist chosen in the knee scenario, respondents chose 2.36 orthopedists and 0.64 rehabilitators, whereas 0.85 orthopedists and 0.58 rehabilitators were chosen in the arthritis scenario. Only 38% of the respondents preferred the CMR's definition of a rheumatologist to describe a rheumatologist.
The younger age group preferred orthopedists to rheumatologists (50% vs. 31%, p<0.001). In the arthritis scenario, the choice of rheumatologist increased from 27% in the elementary school group to 49% in the university group (p<0.001). Mother was the most influential in healthcare seeking.
The discursive analysis revealed that the CMR is positioned as a “we” restricted to “colleagues;” the patient did not have agentive representation. The semiotic structure of the CMR's mission/vision was deemed imprecise and lacking in statements of value and purpose; the readability scores indicated that the text was challenging and dry.
ConclusionsThe CMR's corporate image does not differentiate it from other health providers. CMR's identity seems ambiguous with restricted directionality. It seems pertinent to redefine the CMR.
El Colegio Mexicano de Reumatología (CMR) es una corporación cuya marca tiene dos elementos (imagen e identidad) que la diferencian de otras entidades. El objetivo del estudio es evaluar los aspectos de la imagen e identidad corporativa del CMR.
Sujetos y métodosPara valorar la imagen corporativa, diseñamos una encuesta utilizando enfoques de prueba de concepto y experimentos de elección discreta. Se evaluó cuál definición (ortopedista, reumatólogo o rehabilitador) era más significativa en cuatro escenarios de dolor en adultos sanos de la región occidente del país. Utilizamos análisis del discurso y cinco índices de legibilidad del sitio web de CMR para evaluar la identidad corporativa.
ResultadosSe incluyeron 700 encuestados. Por cada reumatólogo elegido en el escenario de la mano, los participantes escogieron 1,13 ortopedistas y 0,7 rehabilitadores. Por cada reumatólogo en el caso de rodilla, eligieron 2,36 ortopedistas y 0,64 rehabilitadores, mientras que en el de artritis se seleccionaron 0,85 ortopedistas y 0,58 rehabilitadores. Solo 38% de los encuestados prefirió la definición de reumatólogo del CMR para describir a un reumatólogo. El grupo de edad más joven prefirió ortopedistas que reumatólogos (50 vs. 31%, p<0,001). La figura materna fue identificada como la más influyente para las decisiones sanitarias. El análisis del discurso reveló que el CMR se posiciona como un «nosotros» restringido a los «colegas»; el paciente no tuvo representación agente. La estructura semiótica de la misión/visión es imprecisa, faltando declaraciones de valor y propósito. Las puntuaciones de legibilidad indicaron texto difícil y árido.
ConclusionesLa imagen corporativa del CMR no lo diferencia de otros servicios de salud. Su identidad es ambigua con una direccionalidad restringida. Parece pertinente redefinir el CMR.
Rheumatologists and the Colegio Mexicano de Reumatología (Mexican College of Rheumatology-CMR) have significant country-specific social connotations. These terms connote individuals and groups, what they do, why they do it, and where they are headed.
The CMR can be defined as a corporation, and its owners are members who select the board that oversees the organization's activities. A corporate brand describes an organization as a whole and aims to create a consistent corporate image through the interplay of corporate strategy, business activity, and brand stylistics. The corporate brand addresses all influence and target groups, including already-diagnosed rheumatic patients, individuals with musculoskeletal complaints who seek medical attention, policymakers, health institutions, the media, and the pharmaceutical industry.
Internally, the corporate brand embodies a set of values and takes on an orientation function for affiliates (rheumatologists). Rheumatologists’ strong identification with brand values and brand-consistent actions make them important brand ambassadors who convey the idea of the corporation to potential and existing customers. Externally, a corporate identity and image represent how a corporation—in this case, the CMR—presents itself to the public (i.e., patients, family members, decision-makers, the industry, and the rheumatologists themselves). The essential difference between corporate image and corporate identity is perspective: whereas the image describes the subjective perception from the outside, the corporate board specifically controls the identity, which defines how corporate management wants the corporation to be perceived.1
Corporate branding, including its identity and image, has gained more relevance in times of social uncertainty and overabundance.1 It creates added value that is fundamental for competing in markets that offer many products and services that many in society consider interchangeable (e.g., rheumatologist consultation versus charlatanism and “magic” remedies or lay prescriptions).2,3 Despite the need for a corporation to periodically investigate its identity and image to identify opportunities and gaps for improvement,4,5 we did not identify any such approach taken by the CMR.
This study evaluated aspects of the CMR's image and corporate identity. We evaluated corporate image by surveying healthy individuals about which definition (rheumatology, orthopedics, or rehabilitation) has the greatest resonance when seeking adequate care for arthritis or chronic pain in the hands or knees. We evaluated corporate identity by analyzing the CMR's website using a discourse analysis approach and commonly used readability indexes.
Subjects and methodsThis study adopts a cross-sectional, proof-of-concept design and was conducted in Guadalajara, Mexico, during the period from May to July 2023.
Evaluation of the corporate imageThe assessment of a specific aspect of the corporate image was through a survey in Spanish (Table 1) that aimed to determine which definition – that of the orthopedist, the rheumatologist, or the rehabilitator – is most meaningful to respondents in the context of four different scenarios. We used the orthopedist definition in Spanish provided by the American Academy Orthopaedic Surgeons.6 The rheumatologist's definition was provided by the CMR,7 and the definition of a rehabilitator was provided in Spanish by the Mayo Clinic.8 The first posed scenario was chronic hand pain, the second was about chronic knee pain, and the third was about arthritis in the hands. In a fourth question, they were asked to choose one of the three definitions that best define the rheumatology specialist (Table 1).
The questions that were asked to the respondents.
| Hola ¿me ayudas a contestar estas preguntas? Queremos conocer tu opinión sobre qué especialista sería mejor que te atendiera. Tu opinión nos ayuda para saber qué definiciones te hacen más sentido. No hay respuestas correctas, nos interesa tu opinión. Tus respuestas son anónimas y confidenciales. |
| 1. Te anoto 3 definiciones de doctores. Si tuvieras dolor en las coyunturas de las manos por más de 2 meses, ¿con cuál de ellos te atenderías? (selecciona solo una respuesta) |
| • Especialista que se encarga de diagnosticar y tratar las enfermedades musculoesqueléticas y autoinmunes sistémicas. |
| • Especialista dedicado al diagnóstico, tratamiento, rehabilitación y prevención de lesiones y enfermedades que afectan al sistema músculo-esquelético de su cuerpo. |
| • Especialista que diagnostica y trata una variedad de enfermedades que afectan al cerebro, la médula espinal, los nervios y el sistema musculoesquelético. |
| 2. Te anoto 3 definiciones de doctores. Si tuvieras dolor en las rodillas por más de 2 meses, ¿con cuál de ellos te atenderías? (selecciona solo una respuesta) |
| • Especialista que diagnostica y trata una variedad de enfermedades que afectan al cerebro, la médula espinal, los nervios y el sistema musculoesquelético. |
| • Especialista dedicado al diagnóstico, tratamiento, rehabilitación y prevención de lesiones y enfermedades que afectan al sistema músculo-esquelético de su cuerpo. |
| • Especialista que se encarga de diagnosticar y tratar las enfermedades musculoesqueléticas y autoinmunes sistémicas. |
| 3. Si tuvieras artritis en las manos ¿con quién irías? |
| • Especialista que se encarga de diagnosticar y tratar las enfermedades musculoesqueléticas y autoinmunes sistémicas. |
| • Especialista que diagnostica y trata una variedad de enfermedades que afectan al cerebro, la médula espinal, los nervios y el sistema musculoesquelético. |
| • Especialista dedicado al diagnóstico, tratamiento, rehabilitación y prevención de lesiones y enfermedades que afectan al sistema músculo-esquelético de su cuerpo. |
| 4. ¿Cuál de estas definiciones queda mejor para un especialista en reumatología? |
| • Especialista dedicado al diagnóstico, tratamiento, rehabilitación y prevención de lesiones y enfermedades que afectan al sistema músculo-esquelético de su cuerpo. |
| • Especialista que se encarga de diagnosticar y tratar las enfermedades musculoesqueléticas y autoinmunes sistémicas. |
| • Especialista que diagnostica y trata una variedad de enfermedades que afectan al cerebro, la médula espinal, los nervios y el sistema musculoesquelético. |
| 5. Si tuvieras artritis ¿a quién le preguntarías con quién ir? |
| • Madre |
| • Padre |
| • Hermano/a |
| • Hijo/a |
| • Amigo |
| • Otra |
| 6. Sexo |
| • Hombre |
| • Mujer |
| • Prefiero no contestar |
| 7. ¿En qué grupo de edad estás? |
| • <18 años |
| • 18–30 |
| • 31–40 |
| • 41–50 |
| • 51–60 |
| • >60 |
| 8. ¿Hasta qué nivel de escuela terminaste o qué nivel estudias actualmente? |
| • Primaria |
| • Secundaria |
| • Preparatoria |
| • Carretera universitaria |
| 9. ¿Padeces algún problema reumático? |
| • Si |
| • No |
| ¡Muchas gracias por contestar la encuesta! |
The order of options for each studied question was randomized to reduce order bias, including primacy and recency biases.9 All responses were treated as nominal variables. Additionally, to minimize survey fatigue, the structured survey comprised only nine questions: four studied questions, one exploratory question, and four demographic inquiries. The exploratory question was about the perceived influencers or mavens when about to seek medical consultation by asking respondents: If you had arthritis, who would you ask who to go to?
Sample characteristicsWe surveyed four independent samples to optimize resources and compensate for the absence of reference data in our proof-of-concept study. The first three were non-random samples drawn from the family and friends of three medical students during the same week. Invitations were extended to individuals 18 or older and with at least elementary-level schooling. The invited individuals resided in the metropolitan area of Guadalajara and the surrounding small towns. The invitations were delivered through WhatsApp and were accompanied by a link to Google Forms. A response window of 11 days was provided. Using the Central Limit Theorem for proportions, we determined that gathering 100 cases for each sample would yield information with a normal distribution. The fourth sample was assessed two months later utilizing the services of a polling firm. This sample was gathered through simple, on-street, random interviews conducted in the metropolitan area of Guadalajara from 7 to 11 July 2023. The participants were 18 or older, and we ensured that half of the respondents were women. A minimum of 350 respondents were included in the sample to achieve a reliability level greater than 90% and an error margin of 5%.
Evaluating the corporate identityWe assess the CMR's corporate identity using discourse analysis and a readability assessment from the CMR website.10 Discourse analysis is a qualitative research method used to study written (or spoken) language in the context of its social surroundings.11 By analyzing the CMR website's written content, linguistic patterns, and the framing of information, we aimed to have insights into the CMR's identity projection and its engagement with its target audience. This approach offers a comprehensive perspective on how the CMR shapes its image and message, contributing to a better understanding of its overall corporate communication strategy. This analysis was performed by a trained expert (A V-A) unaware at the time of the aims and results of the surveys. The detailed methods and results are in Supplementary file 1.
For the readability assessment, we used five readability indices for Spanish text: Lecturabilidad de Fernández Huerta, Comprensibilidad de Gutiérrez de Polini, Índice de perspicuidad de Szigriszt-Pazos, Escala INFLESZ, and Legibilidad μ de Muñoz y Muñoz. Each index provides an approximation for the difficulty of the text and has been used to evaluate and improve the clarity of a written communication [reviewed in 11]. The analysis used a devoted website12 with algorithms written in Python for each of the six indices. Each index scores from 0 to 100, where 100 is a very easy-to-read text.
Ethical considerationsThis work did not include any experimentation with humans or animals. The first three samples were made through WhatsApp from each student's contacts. There was no addition of any new contacts for this study, and each student invited only their own contact list. The invitation to answer a questionnaire was generic and included a link to Google Forms. The questionnaire did not record the respondent's telephone number or any other sensitive information. The fourth survey was anonymized to the general population. The information collected did not contain sensitive data and did not allow the identification of any particular individual. Therefore, the study did not require evaluation by an ethics committee.
Statistical analysisWe hypothesized that at least 60% of respondents would select the rheumatology definition for each scenario. The analysis relied on four underlying assumptions. First, each of the four samples was considered independent, and no effort was made to control for potential confounders or biases, thus limiting the ability to determine the validity, reliability, and generalizability of the findings. Second, each convenience sample complements the others. We further reported frequency distribution tables for the total surveyed population. Third, as all variables were nominal, the differences were assessed using the Pearson Chi-square test (χ2) to evaluate independence. We use Phi or Cramér's V to determine association strength. Confidence intervals for proportions were calculated at a 95% level, and the two-tailed significance level was set at p≤0.05. Fourth, we added an estimate of the distance between specialties by dividing the rheumatology proportion for each scenario by the corresponding proportion for orthopedics and rehabilitation. Therefore, for every rheumatologist chosen, an estimated n number of orthopedists and an n number of rehabilitators were chosen.
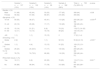
ResultsAll of the invited individuals agreed to participate, resulting in 712 respondents. However, 12 were further (six respondents were under 18 years old, and six did not report their schooling status). Therefore, our analysis included 700 completed surveys. Table 2 presents the respondents’ demographics overall and by sample. The proportions of men and women were similar in all of the samples. Although the samples significantly differed in age distribution and education, the cumulative data across the four samples indicated that most respondents were under 40 years of age and had more than 12 years of schooling. Seventeen percent of respondents reported having a “rheumatic issue,” although the survey's characteristics prevented a specific diagnosis.
Demographics of the 700 surveyed individuals, by sample and overall.a
| Sample 1, n=107 (15%) | Sample 2, n=102 (15%) | Sample 3, n=99 (14%) | Sample 4, n=392 (56%) | Total, n=700 (%) (95% CI) | p value | |
|---|---|---|---|---|---|---|
| Gender, n (%) | ||||||
| Male | 51 (48) | 45 (44) | 33 (33) | 177 (45) | 306 (44) | >0.09 |
| Female | 56 (52) | 57 (56) | 66 (67) | 215 (55) | 394 (56) | |
| Age group, n (%) | ||||||
| 18–30 | 59 (55) | 38 (37) | 40 (41) | 113 (29) | 250 (36) (32–39) | <0.001@ |
| 31–40 | 20 (19) | 29 (28) | 17 (17) | 116 (29) | 182 (26) (23–29) | |
| 41–50 | 15 (14) | 21 (21) | 8 (8) | 74 (19) | 118(17) (14–20) | |
| 51–60 | 12 (11) | 13 (13) | 19 (19) | 89 (23) | 133 (19) (16–22) | |
| >60 | 1 (1) | 1 (1) | 15 (15) | 0 | 17 (2) (1–4) | |
| Schooling, n (%) | ||||||
| Grade 6 | 2 (2) | 0 | 1 (1) | 52 (13) | 55 (8) (6–10) | <0.001* |
| Grades 7–9 | 1 (1) | 4 (4) | 13 (13) | 91 (23) | 109 (15) (13–18) | |
| Grades 10–12 | 26 (24) | 24 (23.5) | 17 (17) | 133 (34) | 200 (29) (25–32) | |
| >12 | 78 (73) | 74 (72.5) | 68 (69) | 116 (30) | 336 (48) (44–51) | |
| Rheumatic issues, n (%) | ||||||
| Yes | 12 (11) | 6 (6) | 22 (22) | 79 (20) | 119 (17) (14–20) | 0.001** |
| No | 95 (89) | 96 (94) | 77 (78) | 313 (80) | 581 (83) (80–85) | |
Table 3 and Fig. 1 show the frequency distribution of responses across scenarios and samples. In the hand scenario, the frequencies were similar among the four samples, with a slight preference for orthopedics. However, orthopedics emerged as the most preferred choice in the knee scenario despite significant differences among samples. The arthritis scenario displayed significant preference differences among samples, with a slightly higher selection frequency for rheumatology. When defining a rheumatologist, the differences among samples were also significant, with orthopedics and rheumatology preferences nearly equal.
Frequency distribution of the responses by scenarios and samples.a
| Questions | Sample 1, n=107 (15%) | Sample 2, n=102 (15%) | Sample 3, n=99 (14%) | Sample 4, n=392 (56%) | Total, n=700 (%) (95%CI) | p value |
|---|---|---|---|---|---|---|
| Hand scenario, n (%) | ||||||
| Orthopedics | 52 (49) | 45 (44) | 48 (48) | 150 (38) | 295 (42) (38–46) | >0.09 |
| Rehabilitation | 18 (17) | 24 (23.5) | 19 (19) | 83 (21) | 144 (21) (18–24) | |
| Rheumatology | 37 (35) | 33 (33) | 32 (33) | 159 (41) | 261 (37) (34–41) | |
| Knee scenario, n (%) | ||||||
| Orthopedics | 71 (67) | 65 (64) | 71 (72) | 207 (52) | 414 (59) (55–63) | <0.001@ |
| Rehabilitation | 13 (12) | 27 (26) | 8 (8) | 65 (17) | 113 (16) (13–19) | |
| Rheumatology | 23 (21) | 10 (10) | 20 (20) | 120 (31) | 173 (25) (21–28) | |
| Arthritis scenario, n (%) | ||||||
| Orthopedics | 29 (27) | 22 (22) | 34 (34) | 159 (41) | 244 (35) (31–38) | 0.004* |
| Rehabilitation | 23 (22) | 32 (31) | 23 (23) | 88 (22) | 166 (24) (21–27) | |
| Rheumatology | 55 (51) | 48 (47) | 42 (43) | 145 (37) | 290 (41) (38–45) | |
| Defining rheumatologists, n (%) | ||||||
| Orthopedics | 40 (37) | 24 (23.5) | 44 (44) | 158 (40) | 266 (38) (34–41) | 0.004# |
| Rehabilitation | 27 (26) | 25 (24.5) | 16 (17) | 106 (27) | 174 (25) (22–28) | |
| Rheumatology | 40 (37) | 53 (52) | 39 (39) | 128 (33) | 260 (37) (33–41) | |
95% CI=95% confidence intervals for proportions.

Fig. 2 provides a visual representation of the distances between specialties. On average, respondents opted for 1.13 orthopedists and 0.70 rehabilitators in the hand scenario for each rheumatologist chosen. In the knee scenario, respondents chose 2.36 orthopedists and 0.64 rehabilitation specialists, whereas a preference for 0.85 orthopedists and 0.58 rehabilitators was observed in the arthritis scenario. Finally, 1.0 orthopedists and 0.67 rehabilitators were selected for each rheumatologist when defining a rheumatologist.

Age was associated with the choice of a specialist in the hand scenario. The youngest age group (i.e., ages 18–30 years) preferred orthopedists over rheumatologists (50.0% vs. 31.2%), and the 41–50-year age group more frequently chose the rheumatologist over the orthopedist (45.8% vs. 34.7%, χ2=17, DF=6, p=0.009; Phi=0.156). Age was also associated with the choice of definition of rheumatology. The 31–40-year age group preferred rheumatology (45.1%) or orthopedics (40.7%) rather than rehabilitation (14.3%; χ2=18.6, DF=6, p=0.005). Age was not associated with specialty in the knee (p=0.263) or arthritis (p=0.769) scenarios.
Schooling was significantly associated with a preference for a specialist in the arthritis scenario. As schooling progressed, the choice of rheumatology increased from 27.3% for those in primary school to 29.4%, 38.5%, and 49.4% for those in secondary school, high school, and university, respectively (χ2=27, DF=6, p<0.001, Cremér's V=0.13). Schooling was also significantly associated with the choice of definition of rheumatology. Respondents with middle (28.4%) and high schooling (27.0%) chose the CMR's definition less frequently than individuals with elementary (34.5%) and university (46.4%) (χ2=26.9, DF=9, p<0.001, Cremér's V=13).
Sex was not significantly associated with the specialist selection in the hand (p=0.4), knee (p=0.6), arthritis (p=0.4), and rheumatologist definition (p=0.1) scenarios. We observed no association between education and preference for a specialist in the hand (p=0.2) or knee (p=0.6) scenarios. Self-reported rheumatic issues were not associated with the chosen specialist in any of the scenarios: hand (p=0.6), knee (p=0.2), arthritis (p=0.8), or rheumatologist definition (p=0.5).
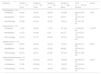
InfluencersTable 4 shows the results of the exploratory question about who would be asked which doctor to go to. Although responses differed significantly among samples, the mother figure was the most frequently mentioned in each sample. Men preferred mother, father, and doctor (37%, 15%, and 15%, respectively), while women preferred mother (41.1%), doctor (15.5%), and friend (10.4%) (χ2=28.7, DF=8, p<0.001). Age was associated, as expected, since 52% of the young group mentioned their mother (52%), but just 14.7% of the older group did it. On the contrary, the older group preferred son/daughter (76.5%) (χ2=158.7, DF=24, p<0.001). The influencer was not associated with the scenarios.
Frequency distribution of influencers as reported by the 700 surveyed individuals.a
| Influencer, n (%) | Sample 1, n=107 (15%) | Sample 2, n=102 (15%) | Sample 3, n=99 (14%) | Sample 4, n=392 (56%) | Total, n=700 (100%) | p value |
|---|---|---|---|---|---|---|
| Mother | 48 (45) | 40 (39) | 36 (37) | 152 (39) | 276 (40) | 0.001** |
| Father | 8 (8) | 12 (12) | 11 (11) | 38 (10) | 69 (10) | |
| Siblings | 13 (12) | 11 (11) | 8 (8) | 34 (9) | 66 (9) | |
| Children | 2 (2) | 4 (4) | 3 (3) | 25 (6) | 34 (5) | |
| Friend | 13 (12) | 16 (16) | 15 (15) | 20 (5) | 64 (9) | |
| Physician | 11 (10) | 13 (13) | 16 (16) | 66 (17) | 106 (15) | |
| Spouse | 1 (1) | 0 () | 2 (2) | 33 (8) | 36 (5) | |
| Internet | 2 (2) | 1 (1) | 1 (1) | 8 (2) | 12 (2) | |
| Others | 9 (8) | 5 (4) | 7 (7) | 16 (4) | 37 (5) |
The full results of the discourse analysis are included in Supplementary file 1. The analysis showed that the enunciation of the CMR website was discursively positioned as a collective “we” that referred to rheumatology specialists and particularly to “colleagues,” and the patient appears as a “necessary actor” within the medical social practice. Although the patient is presented as a potential recipient (addressee), they are never treated as interlocutor. Still, the patient has no agentive representation (i.e., no possibility of intervention in their diagnosis and healing process). Specifically, the physical “patient” was also discursive: they talk about the patient, but the patient is not allowed to act.13 The semiotic structure of the CMR's mission and vision is imprecise and lacks a statement of values and purpose. The overall readability scores corresponded to very difficult and arid text. Specifically, the scores for the Lecturabilidad de Fernández Huerta, the Comprensibilidad de Gutiérrez de Polini, the Índice de perspicuidad de Szigriszt-Pazos, the Escala INFLESZ, and the Legibilidad μ de Muñoz y Muñoz were 26, 29, 21, 21, and 42, respectively.
DiscussionThe significance of rheumatologists and the CMR cannot be understated, given the substantial market value at stake. To illustrate, roughly 900 rheumatologists, along with the CMR, play a pivotal role in serving a population exceeding 15 million individuals with musculoskeletal disorders in Mexico.14 Furthermore, in 2020, the Mexican market for antirheumatic drugs was valued at US$6.3 billion, with a compound annual growth rate of 2.2%.15
Rheumatologists have united under the banner of the CMR to represent their profession. Therefore, what it is in a name must be considered in fostering cohesion, achieving desired outcomes, and forging a reputation.16 It is advised that corporations periodically investigate their brand's identity and image, especially in rapidly changing and evolving times, to identify opportunities and gaps for improvement.4,5 We did not find any publication on it, so we carried out this study.
We identified that CMR's corporate image did not effectively distinguish rheumatologists from orthopedists or rehabilitation specialists, even when the term “arthritis” was employed. Regardless of the scenario presented, six out of 10 respondents did not select a rheumatologist for chronic pain assessment. Although we provided definitions for only orthopedists and rehabilitators, these findings have substantial implications in a growing youth-driven country in which multiple health services are disconnected from one another. In such settings, the onus of choosing a healthcare provider falls squarely on the patients, whose options range from charlatans and those dispensing non-conventional remedies to generalists to laypeople and rheumatologists, with little distinction among them.2,3,17,18
Notably, as many respondents perceived mothers as the first to ask for advice on which doctor to see if they had arthritis-related problems, targeting the “mother figure” warrants further consideration when planning awareness campaigns.
Our findings about CMR's corporate identity also revealed areas for reflection. The CMR website appears to be oriented toward peers (“compañeros”), positioning patients as discursive actors but seemingly disconnected from the core construct of CMR. The readability scores indicated that the text was highly challenging and dense.
Assigning value judgments—from correct to discordant—regarding CMR's identity and image relies on its brand characteristics and the role that CMR aims to play vis-a-vis its diverse stakeholders. This role should be explicitly articulated on its website. For instance, the British Society for Rheumatology places a strong emphasis on patient-centered care,19 EULAR fosters the Emerging EULAR Network (EMEUNET), which caters to young rheumatologists,20 and the American College of Rheumatology centers its focus on rheumatology professionals.21 Contrarily, the semiotic structure of CMR's declared mission and vision is imprecise and lacks statements regarding core values and purposes. Readers may benefit from reviewing the several exemplary mission statements of Fortune 500 companies.22
This study has several limitations. First, the study suffers from the inherent constraints of a proof-of-concept approach, which assesses the presence but not the frequency or magnitude of a phenomenon in the absence of factual information. annoSecond, our study reports only on some functional aspects of corporate image and identity, but not others. A comprehensive evaluation is crucial and would necessitate the corporation's active involvement.4,5 Third, we in no way evaluate any of the academic activities or performance of actual or past CMR boards. Fourth, given the proof-of-concept nature of our study, the generalizability of our results is confined to our specific sample of non-random respondents from the country's Western region; we do not claim representativeness. Nonetheless, the consistency of results across diverse samples could be considered a strength as it indicates a trend. Fifth, we selected orthopedics and rehabilitation as comparators given their perceived similarity to rheumatology, allowing us to assess whether individuals differentiate between these “services” or “products”. Although the consideration was intriguing, we chose to exclude providers of unconventional remedies as it would have introduced cultural and belief-related factors as confounders. Sixth, our study did not ascertain whether the features assessed represent the core of the CMR or are merely aspects of its communication approach. Seventh, although the discourse analysis was performed by a researcher external to rheumatology and experienced in this type of analysis (AV-A), this approach is qualitative and based on a single text (the website).
ConclusionsDespite the limited available evidence,23–25 we assert that rheumatologists are better at caring for rheumatic patients than other providers. Indeed, the significance of rheumatologists to a nation is evident when considering the prevalence of rheumatic conditions, the indirect costs associated with these diseases, and the potential and ever-present possibility of preventable disability.
Therefore, to serve well, national corporations representing rheumatologists, such as the CMR, must have clear and consistent manifestos about who they are, what they represent, what they are for, their ethical principles, and where they are heading. These manifestos are mission, vision, purpose, core values, and social responsibility statements. These statements govern the corporation within (identity) and for society (image) and allow the differentiation of other services and products. However, the CMR website lacks some of these statements, and the existing ones require refinement. CMR's owners are responsible for determining the relevance of our results and, in turn, calling for a consensus that would define whether CMR's objectives and statements are according to contemporary times or need to evolve. After all, the CMR operates in a country that boasts the largest population of Spanish speakers, ranks fourteen in geographical size, tenth in population size, fifteenth in nominal gross domestic product, and eleventh in purchasing power parity globally.
Authors’ contributionsEach author participates in the study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
Availability of data and material (data transparency)Data available upon request.
Statement of generative AI and AI-assisted technologies in the writing processWe used a large language model (Grammarly. https://app.grammarly.com/) solely to check spelling and grammar.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or non-for-profit sectors.
Conflict of interestNone.
None.
The following are the supplementary data to this article:



