





AS is a chronic disease with an inflammatory serum microenvironment characterized by increased oxidative stress (OS). Along with OS, reactive oxygen species (ROS) are elevated in patients with AS. Overexpression of ROS causes active inflammatory processes leading to the secretion of pro-inflammatory factors, including tumor necrosis factor-alpha (TNF-α). Immature granulocytes (IG) are essential to the chronic inflammatory process. This may mean that IG can be a parameter used in the follow-up of chronic inflammatory diseases such as AS.
ObjectiveWe aimed to evaluate the change in IG in patients with AS who were on biologic medication for six months after diagnosis and to assess its relationship with disease activity, remission, and BASDAI score.
MethodsThis single-center, retrospective study was conducted between January 2020 and January 2022. For the study, 68 patients were included in the patient group and 74 patients in the control group. Demographic and laboratory data were recorded and compared in the groups. Then, the patient group was divided into two groups: pre-biologic drug and post-biologic drug. Hemogram data, IG, ESR, CRP, and BASDAI data were recorded for both groups. Correlation analysis was performed between the results of IG data and hemogram and laboratory data.
ConclusionIn our study, WBC, neutrophil, IG, and IG% ratios were significantly higher in AS patients compared to the control group. Neutrophil, IG, and IG% levels were significantly decreased in the AS group compared to pretreatment and post-treatment comparisons. In addition, IG levels were correlated with WBC, neutrophil, CRP, and ESR levels. This study hypothesized that IG values may be a valuable parameter for monitoring AS disease severity, response to treatment, and disease activation after biological drug use.
La espondilitis anquilosante (EA) es una enfermedad crónica con un microambiente sérico inflamatorio caracterizado por un aumento del estrés oxidativo (EO). Junto con el EO, las especies reactivas del oxígeno (ERO) están elevadas en los pacientes con EA. La sobreexpresión de ROS provoca procesos inflamatorios activos que conducen a la secreción de factores proinflamatorios, incluido el factor de necrosis tumoral alfa (TNF-α). Los granulocitos inmaduros (GI) son esenciales para el proceso inflamatorio crónico. Esto puede significar que los GI pueden ser un parámetro utilizado en el seguimiento de enfermedades inflamatorias crónicas como la EA.
ObjetivoNos propusimos evaluar el cambio en los GI en pacientes con EA que recibieron medicación biológica durante seis meses tras el diagnóstico y valorar su relación con la actividad de la enfermedad, la remisión y la puntuación BASDAI.
MétodosEste estudio unicéntrico y retrospectivo se realizó entre enero de 2020 y enero de 2022. Para el estudio, se incluyeron 68 pacientes en el grupo de casos y 74 pacientes en el grupo de control. A continuación, el grupo de casos se dividió en dos grupos: pre-fármaco biológico y post-fármaco biológico. Se registraron los datos del hemograma, la GI, la VSG, la PCR y el BASDAI de ambos grupos. Estos dos grupos se compararon entre sí.
ConclusionesEn nuestro estudio, las proporciones de CMB, neutrófilos, GI y porcentaje de GI fueron significativamente mayores en los pacientes con EA en comparación con el grupo de control. Los niveles de neutrófilos, GI y porcentaje de GI disminuyeron significativamente en el grupo de pacientes con EA en comparación con las comparaciones pretratamiento y postratamiento. La disminución de los niveles de VSG y PCR acompañó a la disminución de los niveles de GI y porcentaje de GI. Además, los niveles de GI se correlacionaron con los de CMB, neutrófilos, PCR y VSG. La hipótesis de este estudio es que los valores de GI pueden ser un parámetro valioso para monitorizar la gravedad de la enfermedad de EA, la respuesta al tratamiento y la activación de la enfermedad tras el uso de fármacos biológicos.
Ankylosing spondylitis (AS) is a chronic inflammatory disease with genetic predisposition, yet it presents with diverse clinical features. It is primarily associated with human leukocyte antigen (HLA)-B27.1 Clinical features include inflammatory back pain, peripheral arthritis, enthesitis, and specific organ involvement (inflammatory bowel disease, anterior uveitis, etc.).2
AS is a chronic disease characterized by increased oxidative stress (OS) and an inflammatory serum microenvironment. Chronic inflammation is a fundamental feature of AS pathogenesis. Studies have shown that OS is elevated in patients with AS compared to healthy individuals.3 However, the mechanism of OS in AS patients is not well understood. OS is directly related to inflammation. In a study conducted by Solmaz et al., the total OS level was higher in active AS (BASDAI>4) patients compared to inactive ones. This study demonstrated a correlation between OS levels and BASDAI, BASFI, ESR, and CRP levels.4 There is also a positive relationship between OS levels and reactive oxygen species (ROS). Compared to normal controls, ROS levels are elevated in AS patients.5 The overexpression of ROS leads to active inflammatory processes, resulting in the secretion of pro-inflammatory factors, including tumor necrosis factor-alpha (TNF-α). It is also known that TNF-α activates granulocytes and prolongs their lifespan. In summary, the interaction between inflammation, oxidative stress, and ROS is closely related to the pathogenesis of AS.6
It is a known fact that neutrophils contribute to both anti-inflammatory and pro-inflammatory processes.7 Recent studies have demonstrated that, contrary to previous beliefs, neutrophils are a heterogeneous population. In healthy donors, normal density neutrophils are present. In patients with chronic inflammation, a heterogeneous population of mature and immature neutrophils exists. These heterogeneous populations of neutrophils are referred to as low-density neutrophils, low-density granulocytes (LDGs), or granulocytic myeloid-derived suppressor cells.8 LDGs were first identified in systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA).9 Immature granulocytes (IGs) are also a type of LDG. Studies have shown that IGs can be associated with disease activation in rheumatological diseases such as granulomatous polyangiitis and systemic lupus erythematosus.10
IGs develop from myeloid stem cells in the bone marrow. In the early stages of development, IGs have a large nucleus and clear cytoplasm. As they mature, the nucleus fragments, and granules containing enzymes and other proteins form in the cytoplasm.11 Certain cytokines are known to affect the formation and function of IGs. These cytokines include granulocyte colony-stimulating factor (G-CSF), interleukin-6 (IL-6), and TNF-α. G-CSF is a growth factor that stimulates the production of immature granulocytes in the bone marrow. It acts on myeloid stem cells and progenitor cells, promoting their differentiation into granulocytes. IL-6 stimulates the proliferation of myeloid progenitor cells and increases G-CSF production, leading to an increase in IGs. TNF-α has various effects, including the regulation of IG production and function. TNF-α stimulates the proliferation of myeloid progenitor cells and the differentiation of promyelocytes into myelocytes, leading to increased IG production.12
In conclusion, IGs are a significant component of the chronic inflammatory process. Their presence in circulation may indicate ongoing inflammation. In patients with AS, increased OS levels and ROS production may lead to a heterogeneous neutrophil response. This may trigger an increase in pro-inflammatory LDGs. Consequently, IGs may serve as an easily monitorable marker of disease activity in serum. Based on this pathophysiology, we aimed to measure IG levels in AS patients before and after treatment, comparing the outcomes. This study aims to demonstrate the utility of IGs as a valuable parameter in disease monitoring.
Material and methodsThis single-center, retrospective study was conducted at the Department of Rheumatology, Kahramanmaras Sutcu Imam University Faculty of Medicine, between January 2020 and January 2022. We aimed to assess the changes in immature granulocyte (IG) levels in patients diagnosed with ankylosing spondylitis (AS) who used biologic agents for six months post-diagnosis and to evaluate the relationship of these changes with disease activity, remission, and BASDAI score. Patient data were obtained from our hospital's digital data recording module.
Measurement of IGThe IG levels of our patients were measured using the Sysmex XN_3000 hematology analyzer (Sysmex Corp., Kobe, Japan).
Inclusion and exclusion criteriaThe study included 68 AS patients who met the Assessment of SpondyloArthritis International Society (ASAS) criteria for axial spondyloarthritis. In the retrospective screening, all patients with access to Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) records, available laboratory data, and regular follow-up visits were included in the patient group. The indication for starting TNF-α blockers was a BASDAI score>4 despite at least three months of non-steroidal anti-inflammatory drug (NSAID) use. Patients who regularly used TNF-α blockers for six months were selected. These patients were required to refrain from using any steroid-containing medications during the six-month period. Patients who achieved a >2-point decrease in BASDAI score after six months of follow-up were included in the study. The control group comprised 74 patients who agreed to participate in the study.
Patients with any rheumatologic, oncologic, or metabolic diseases other than AS were excluded from both the patient and control groups. Patients with suggestive findings of infection or a history of medication use, such as glucocorticoids, that could affect IG levels during the measurement period were also excluded from the study. Additionally, patients with incomplete clinical and laboratory data identified during retrospective screening, those who did not attend regular follow-up visits, and those who refused to participate were excluded from the study.
MethodologyA total of 1132 patients were screened for the study, and 68 patients who met the inclusion and exclusion criteria were included. Seventy-four healthy individuals who met the inclusion and exclusion criteria were included in the control group. Demographic data and laboratory parameters (white blood cell (WBC), neutrophil, lymphocyte, hemoglobin (HGB), IG, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)) were recorded for all groups. All clinical and laboratory data were recorded immediately before the initiation of biological therapy and six months after treatment. BASDAI scores were recorded for all patients in the patient group. Patient and control groups were compared in terms of demographic and laboratory data. Subsequently, the patient group was divided into two groups: pre-biologic therapy and post-biologic therapy. Hemogram data, IG, ESR, CRP, and BASDAI data were recorded for both groups and compared with each other. Correlation analysis was performed between the results of IG data and hemogram and laboratory data.
Statistical analysisThe Kolmogorov–Smirnov test was used to assess normality. Continuous variables were presented as mean±standard deviation or median (1st quartile–3rd quartile), depending on the normality of distribution, while categorical variables were expressed as frequency (percentage). Group comparisons for continuous variables were conducted using either Student's t-test or Mann–Whitney U test, contingent upon the distribution normality. Repeated measurements of continuous variables were assessed using paired t-test or Wilcoxon signed ranks test, depending on distribution normality. Categorical variables were analyzed using the Chi-square test or Fisher–Freeman–Halton test. Analysis among different biological drug groups was performed using the Kruskal–Wallis test. Correlations between variables were evaluated using Pearson or Spearman correlation coefficients. All statistical analyses were conducted using IBM SPSS Statistics for Mac, Version 29.0 (IBM Corp., Armonk, NY, USA). Results with p<0.05 were considered statistically significant.
Ethical approvalOur study was approved by the Kahramanmaras Sutcu Imam University Medical Ethics Committee on 13.12.2022 with approval number 2022/37.
ResultsWe enrolled a total of 68 patients diagnosed with ankylosing spondylitis (AS) and 74 healthy individuals as controls, with a mean age of 38.62±10.25 years (range: 18–68) in our study. The age distribution did not show a significant difference between the patient and control groups (p: 0.467). Regarding gender distribution, 44.1% (n: 30/68) of participants in the AS group were female, while a similar proportion of 43.2% (n: 32/74) was observed in the control group (p: 0.916).
The white blood cell (WBC) count, neutrophil count, immature granulocyte (IG) levels, and IG percentile value were significantly higher in AS patients compared to controls (p<0.05). Conversely, hemoglobin levels in AS patients were significantly lower than those in healthy controls (p<0.05). The comparison of age, gender, and laboratory values between AS patients and the healthy control group is summarized in Table 1.
Summary of participants’ characteristics and lab results by groups.
| Groups | |||
|---|---|---|---|
| AS patients (n: 68) | Healthy control (n: 74) | p | |
| Age, years | 39.26±10.20 | 38.03±10.33 | 0.467 |
| Sex | |||
| Male, n (%) | 38 (44.10%) | 32 (43.20%) | 0.916 |
| Female, n (%) | 30 (55.90%) | 42 (56.80%) | |
| WBC (×103) | 8.25 (6.62–9.98) | 6.87 (6.18–7.82) | <0.001 |
| Neutrophil (×103) | 4.82 (3.89–6.48) | 3.92 (3.32–4.81) | <0.001 |
| Lymphocyte (×103) | 2.25 (1.92–2.63) | 2.07 (1.78–2.56) | 0.089 |
| Hemoglobin | 13.06±1.85 | 14.30±1.88 | <0.001 |
| RDW | 41.30 (38.90–43.80) | 41.10 (38.60–43.70) | 0.652 |
| IG | 0.03 (0.02–0.04) | 0.02 (0.01–0.02) | <0.001 |
| IG (%) | 0.3 (0.20–0.40) | 0.25 (0.20–0.30) | <0.001 |
Data are given as mean±standard deviation or median (1st quartile–3rd quartile) for continuous variables according to normality of distribution and as frequency (percentage) for categorical variables.
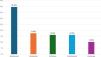
In our study, among the 68 examined AS patients, HLA-B27 was positive in 30 (44.1%) patients and negative in 19 (27.9%) patients. The median duration of the disease was 7.00 years (interquartile range (IQR): 4–11.0, range 1–19). The median duration of biological drug use was 32.5 months (IQR: 14–50, range 4–74). Among the AS patients, 27 (39.7%) received Adalimumab, 12 (17.6%) received Golimumab, 11 (16.2%) received Infliximab, 11 (16.2%) received Certolizumab, and 7 (10.3%) received Etanercept. Supplementary Data: Table 1 summarizes the disease and treatment characteristics of AS patients, and Fig. 1 illustrates the distribution of treatments received.

In the AS group, parameters of AS patients were compared before and after treatment. Following treatment, there was a significant decrease in the BASDAI score from baseline (7.2–3.98) (p<0.001). However, there was no significant difference observed between post-treatment and baseline white blood cell (WBC) levels in the AS group (p: 0.103). Similarly, neutrophil levels significantly decreased from baseline (4.82×10^3 to 4.53×10^3) after treatment (p: 0.023). Conversely, lymphocyte count increased significantly from baseline (2.25×10^3 to 2.48×10^3) following treatment (p: 0.040). Hemoglobin levels also displayed a significant increase after treatment, rising from an average of 13.15mg/dl to 13.7mg/dl (p: 0.002). No significant change in Red Cell Distribution Width (RDW) levels was noted (p: 0.342).
Furthermore, immature granulocyte (IG) levels demonstrated a significant decrease after treatment, with values decreasing from 0.03 to 0.02 (p<0.001), and IG percentile value decreased from 0.30 to 0.26 (p<0.001). There was no significant change in Mean Platelet Volume (MPV) values compared to baseline (p: 0.665). C-reactive protein (CRP) levels significantly decreased after treatment, from 10.7 to 3.22 (p<0.001). Sedimentation levels also exhibited a significant decrease, from 16 to 11 (p<0.001).
The comparison of baseline and post-treatment values in AS patients is presented in Table 2.
Comparison of baseline and after treatment values in AS patients.
| Baseline (n: 68) | After treatment (n: 68) | p value | |
|---|---|---|---|
| BASDAI | 7.2 (6.4–8.3) | 3.98 (2.8–4.7) | <0.001** |
| WBC (×103) | 8.25 (6.62–9.98) | 7.96 (6.7–9.59) | 0.103 |
| Neutrophil (×103) | 4.82 (3.89–6.48) | 4.53 (3.46–5.87) | 0.023** |
| Lymphocyte (×103) | 2.25 (1.92–2.63) | 2.48 (2.11–2.95) | 0.040** |
| Hemoglobin | 13.15 (11.7–14.5) | 13.7 (12.05–15) | 0.002** |
| RDW | 41.25 (38.85–43.75) | 41.1 (39.3–43.7) | 0.342 |
| IG | 0.03 (0.02–0.04) | 0.02 (0.02–0.03) | <0.001** |
| IG (%) | 0.30 (0.2–0.4) | 0.26 (0.2–0.3) | <0.001** |
| CRP | 10.7 (3.7–23) | 3.22 (3.19–12.05) | <0.001** |
| Sedimentation | 16 (7–27) | 11 (4–18) | <0.001** |
The comparison between HLA-B27 positive (n: 30) and negative (n: 19) individuals revealed no statistically significant difference in age distribution (p: 0.405). Similarly, there was no significant discrepancy observed in gender distribution between the two groups (p: 0.204). Regarding treatment characteristics, no significant differences were noted in the distribution of biological drugs (p: 0.483) or the duration of biological drug use (p: 0.309) between the HLA-B27 positive and negative cohorts.
Analysis of disease activity measured by BASDAI score demonstrated a significant reduction post-treatment within both HLA-B27 positive and negative groups (p<0.001). However, the change in BASDAI score did not significantly differ between the groups (p: 0.100).
Hematological parameters, including white blood cell (WBC) count, neutrophil count, and hemoglobin levels, were also evaluated. There was a significant difference in baseline WBC count between HLA-B27 positive and negative groups (p: 0.016). After treatment, this difference persisted, with the HLA-B27 positive group showing a lower WBC count compared to the negative group (p: 0.022). A significant difference in neutrophil count was observed both at baseline (p: 0.026) and after treatment (p: 0.036) between HLA-B27 positive and negative groups, indicating a lower count in the HLA-B27 positive group in both instances. However, there were no significant differences in lymphocyte count, hemoglobin levels, Red Cell Distribution Width (RDW), immature granulocyte (IG), and IG percentile levels between HLA-B27 positive and negative groups at both baseline and after treatment. These findings suggest that these parameters are not influenced by HLA-B27 status in patients with ankylosing spondylitis undergoing biological therapy.
Inflammatory markers, such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), displayed significant reductions post-treatment within both HLA-B27 positive and negative groups (p=0.014, p=0.006, respectively). However, the change in these markers did not significantly differ between the two groups. Analysis of demographic, laboratory, and inflammatory data is given in Supplementary Data, Table 2.
In our correlation analysis, we examined the relationship among immature granulocytes (IG), immature granulocyte percentile (IG%), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), complete blood count parameters, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) in 68 patients diagnosed with ankylosing spondylitis (AS).
The table displays correlations (represented by ‘r’) and corresponding p-values for various parameters: A positive, strong, and significant correlation was observed between changes in IG and changes in IG% (r: 0.955, p<0.001). Similarly, there was a positive, moderate, and significant correlation between changes in IG and changes in BASDAI (r: 0.262, p: 0.031). Positive, moderate, and significant correlations were also found between changes in IG and certain complete blood count parameters: white blood cell count (WBC) (r: 0.481, p<0.001), neutrophil count (r: 0.455, p<0.001), lymphocyte count (r: 0.261, p: 0.031), and mean platelet volume (MPV) (r: 0.273, p: 0.024). However, negative, moderate, and significant correlations were observed between changes in IG and changes in hemoglobin (r: −0.278, p: 0.022) and platelet count (r: −0.289, p: 0.017). Additionally, a positive, moderate, and significant correlation was found between changes in IG and CRP levels (r: 0.374, p: 0.002). Similarly, positive, moderate, and significant correlations were observed between changes in IG% and WBC (r: 0.264, p: 0.029), lymphocyte (r: 0.239, p: 0.049), and MPV (r: 0.250, p: 0.04).
The correlation analysis of IG, IG%, BASDAI, complete blood count parameters, and infection markers is presented in Supplementary Data, Table 3 for AS patients.
DiscussionAS is a chronic inflammatory disease. In the pathogenesis of AS, oxidative stress (OS) is increased, and in response, pro-inflammatory cytokines in the serum microenvironment have been shown to rise.4,5 Chronic inflammation is a hallmark of AS. The levels of OS and its interaction with reactive oxygen species (ROS) are critical in triggering the pro-inflammatory response, including TNF-α.12,13 This pro-inflammatory microenvironment can enhance granulocyte production and activation, contributing to chronic inflammation.
ROS can affect the survival of adaptive immune cells in the bone marrow. As explained in the introduction, ROS can cause heterogeneity in immune cells.14 Pro-inflammatory cytokines have been shown to regulate ROS levels by increasing OS.15,16 Increased levels of IFN-γ and TNF-α in the bone marrow (BM) have been found to correlate with higher ROS levels in the BM.17 It is also known that an age-related pro-inflammatory process starts in the BM. Studies have shown that with aging, the level of IL-15, which preserves pro-inflammatory CD8+, CD25− T cells, increases. IL-6 works synergistically with IL-15. The expression of IL-15 and IL-6 is stimulated by IFN-γ and TNF. IFN-γ levels have been shown to be associated with ROS levels in the BM.18 In summary, in an inflammatory BM, the heterogeneity of pro-inflammatory cells, such as CD8+, CD25− T cells, is enhanced. In chronic inflammatory diseases like AS, where increased OS and ROS in the serum microenvironment are documented, effects similar to age-related BM changes may occur. This can indirectly reflect on hemogram parameters.
In our study, WBC, neutrophil, IG, and IG% levels were found to be significantly higher in AS patients compared to the control group. This result is considered a consequence of the chronic inflammatory response in AS. It indirectly supports the positive correlation between increased serum OS levels and IG levels in AS. Studies have demonstrated a reduction in total OS and associated ROS levels following treatment in AS. Moreover, the decrease in OS levels correlated with BASDAI, ESR, and CRP levels.4 One study showed a significant reduction in OS levels following infliximab treatment.3 There are also studies where no correlation was found between OS levels and activity indices.19 However, this study was conducted with a small number of patients (n=30). In our study, IG levels decreased in response to the reduction in BASDAI, CRP, and ESR in AS patients who achieved remission under anti-TNF therapy, showing a correlation. The elimination of pro-inflammatory cytokines and the reduction of the inflammatory burden in the microenvironment were reflected in the hematological parameters. In these patients, IG levels may serve as an indirect indicator of the serum inflammatory burden (OS, ROS, and TNF). Our study's results support this hypothesis.
BASDAI includes six items measuring fatigue, back, neck or hip pain, peripheral joint pain and swelling, localized tenderness, and the duration and severity of morning stiffness. However, BASDAI is entirely subjective and lacks an objective measure of inflammation.20 New measurements incorporating ESR and CRP have been developed to provide a more objective basis for BASDAI scores.21 Objective parameters are needed to reinforce clinical remission and establish a more objective basis for patient follow-up in AS patients. In our study, IG levels correlated with BASDAI levels. This result indicates that IG is an easily accessible and trackable parameter for monitoring disease, deciding on remission, and evaluating treatment effectiveness.
Another consequence of chronic inflammation is the decrease in HGB due to altered responses in HGB production and destruction related to increased cytokines. Studies have shown that cytokines like TNF-α, IL-1, and IL-6 inhibit erythroid series production in the bone marrow. Moreover, the inflammatory microenvironment interferes with iron metabolism by increasing hepcidin from the liver via cytokines, slowing down erythrocyte production by reducing iron utilization.20,21 In our study, HGB levels in the AS group were significantly lower before treatment, while post-treatment HGB levels were significantly higher in both AS and control groups. Furthermore, there was no difference in post-treatment HGB levels between the control and AS groups. When the inflammatory process subsided, HGB levels rose to levels similar to the healthy control group. This increase in HGB levels inversely correlated with the reduction in IG levels. As IG levels decreased, HGB increased, supporting the accuracy of IG in indicating inflammation.
The limitations of our study include the small number of patients. Additionally, the relationship between OS levels and IG levels was inferred from other studies and our own study results. Further research comparing OS levels and serum IG levels is needed to clarify this relationship.
Finally, IG levels showed a correlation with WBC, neutrophil, CRP, and ESR levels. This result demonstrates that IG is a reliable parameter for monitoring the inflammatory response in AS patients.
AS is an inflammatory disease that can be chronic and systemic. In this study, we hypothesized that IG values could be a valuable parameter for monitoring disease severity, treatment response, and disease activity post-biologic therapy in AS patients. The fact that it is a cheap and easily accessible parameter enhances its value.
Ethical approval and informed consentEthical approval was obtained from the Ethics Committee of Kahramanmaraş Sütçü İmam University.
FundingThe author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributionsScientific design of the study: Gözde Yıldırım Çetin, Burak Okyar.
Data collection and interpretation: Burak Okyar, Servet Yüce, Bekir Torun.
Manuscript writing: Burak Okyar, Servet Yüce, İlyas Öztürk.
Manuscript revision: Burak Okyar, Servet Yüce, Gözde Yıldırım Çetin.
Consent for publicationWritten informed consent was obtained from all patients for publication of this report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Conflict of interestThe authors declare no conflict of interest.
Availability of supporting dataAll data are kept at the data center of Kahramanmaraş Sütçü İmam University Medical Faculty Hospital.
Artificial intelligenceArtificial intelligence tools were not used at any stage of the preparation of this paper.
The followings are the supplementary data to this article:



