




We read the publication by Ly-Pen and Andreu1 in Reumatología Clínica with great attention. They reported the case of a 39-year-old woman who had been diagnosed with bilateral carpal tunnel syndrome secondary to Madelung's deformity. She received a local injection of triamcinolone, which improved the symptoms. We would like to express our experience in the pediatric rheumatology unit of our hospital.
Madelung's deformity is a dysplasia of the distal radial physis. Its early closure is accompanied by a progressive deformity with dorsal dislocation of the ulna and palmar carpal displacement and, thus, supination and rotation are limited. It affects girls between the ages of 8 and 12 years, and is generally bilateral. This disorder is associated with a number of syndromes such as Leri–Weill dyschondrosteosis, Hurler syndrome, Turner syndrome, chondrodysplasia and Ollier disease.
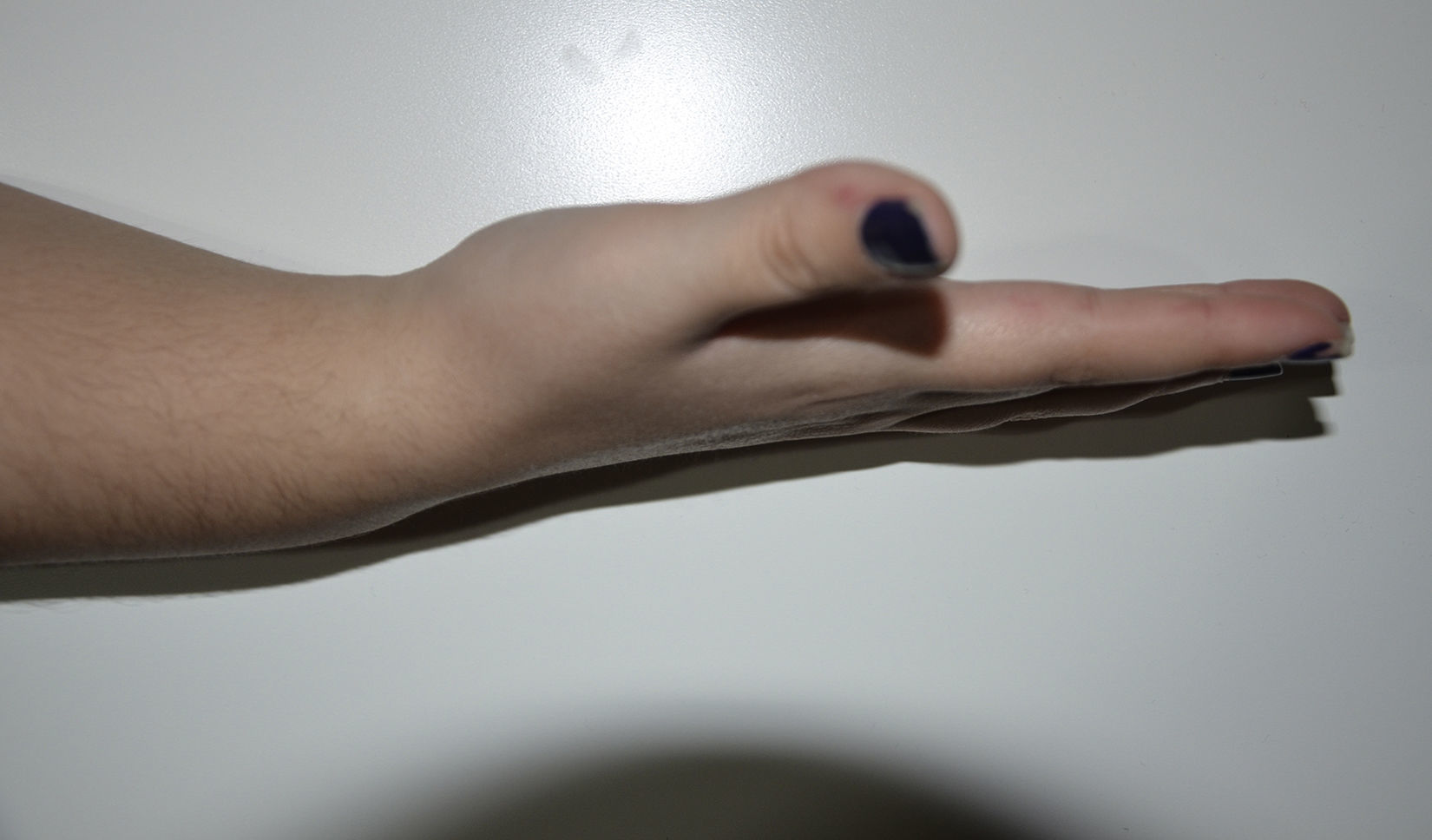
We report the case of a 14-year-old girl who in October 2015 had been diagnosed with Leri–Weill syndrome. The disease was detected incidentally in a radiograph carried out due to a traumatic injury. She had mutations in the Short Stature Homeobox-containing (SHOX) gene and in pseudoautosomal region 1 (PAR1) in 5′. She was referred to pediatric rheumatology by her endocrinologist as she complained of mechanical pain in both carpi that had increased progressively in the preceding months and had a poor response to ibuprofen. The results of physical examination were consistent with bilateral Madelung's deformity, with pain on dorsal flexion of both carpi, with no limitation (Figs. 1–3). There was no evidence of paresthesias or other neurological symptoms. Under sedation, the patient received the injection of 20mg of triamcinolone in each carpi. In a check-up 1 month later, she reported a clear improvement, mentioning the nearly complete disappearance of the pain within 24–48h after the injection, and an improvement in mobility.


We consider that, like the authors of the letter we comment here, local corticosteroid injection is a valid option in cases of carpal pain secondary to Madelung's deformity during the pediatric age, even in the absence of symptoms of carpal tunnel syndrome. Moreover, as the skeleton of the child is still growing, it is necessary to postpone surgical treatment. Thus, in our opinion, local injection is an interesting conservative option given the potential relief of the symptoms, with a low probability of complications. Nevertheless, we have not found publications dealing with this therapeutic approach, nor of its medium- and long-term efficacy.
Please cite this article as: Muñoz Calonge MA, Murias Loza SM, Itza N. En respuesta a: Deformidad de Madelung. Reumatol Clin. 2018;14:60–61.


