






Trichorhinophalangeal syndrome (TRPS) is a rare multisystem disorder characterized by abnormalities in the hair (tricho), nose (rhino), and digits (phalangeal). A variety of nonspecific intraoral findings have been reported in the literature, including hypodontia, delayed tooth eruption, malocclusion, a high-arched palate, mandibular retrognathia, midface hypoplasia, and multiple impacted teeth. In addition, supernumerary teeth have been detected in several persons with TRPS, especially type 1. This report describes the clinical manifestations and dental management of a TRPS 1 patient with multiple impacted supernumerary and permanent teeth.
PatientA 15-year-old female patient visited our clinic with a known medical history of TRPS 1 with laceration of the tongue caused by teeth eruption in the palate.
ResultsRadiographic images showed a total of 45 teeth: two deciduous, 32 permanent, and 11 supernumerary teeth. Six permanent teeth and 11 supernumerary teeth in the posterior quadrants were impacted. Four impacted third molars, supernumerary teeth, retained deciduous teeth, and impacted maxillary premolars were removed under general anaesthesia.
Discussion and conclusionsThis case suggests that all patients with TRPS should undergo full clinical and radiographic oral examination and should be informed about the disease and the importance of dental counselling.
El síndrome tricorrinofalángico (TRPS) es un trastorno multisistémico raro caracterizado por anomalías en el pelo (trico), la nariz (rino) y los dedos (falángico). En la literatura se han reportado una variedad de hallazgos intraorales inespecíficos, incluyendo hipodontia, demora de la erupción dental, maloclusión, paladar muy arqueado, retrognatia mandibular, hipoplasia en la sección media del rostro y múltiples dientes impactados. Además, se han detectado dientes supernumerarios en diversas personas con TRPS, en especial de tipo 1. Este informe describe las manifestaciones clínicas y el manejo dental de una paciente con TRPS 1 con múltiples dientes impactados, supernumerarios y permanentes.
PacienteUna paciente de 15 años con historia médica conocida de TRPS 1 se presentó en nuestra clínica quejándose de laceración de la lengua causada por dientes erupcionados.
ResultadosLas imágenes radiográficas mostraron un total de 45 dientes: 2 deciduos, 32 permanentes y 11 supernumerarios. Seis dientes permanentes y 11 dientes supernumerarios de los cuadrantes posteriores resultaron impactados. Se extrajeron 4 terceros molares y dientes supernumerarios impactados, dientes deciduos retenidos y premolares maxilares impactados bajo anestesia general.
Discusión y conclusionesEste caso evidencia que todos los pacientes con TRPS deberían someterse a exámenes orales completos a nivel clínico y radiográfico, y ser informados sobre la enfermedad y la importancia del asesoramiento dental.
Trichorhinophalangeal syndrome (TRPS) was first described in 1966 by Giedion and then classified into three types (TRPS 1-2-3), depending on the severity of the phenotype and cytogenetic/molecular findings.1
TRPS 1 is characterized by slow growing, sparse and thin hair, bulbous and prominent tip of the nose, and peripheral dysostosis (conical epiphysis in the hands and feet). Intraoral findings in patients with TRPS 1 include malocclusion, crowding, microdontia, hypodontia, delayed tooth eruption, high caries index and maxillary/mandibular hypoplasia, multiple impacted teeth,1–3 and supernumerary teeth.1–7
The other type of syndrome is Langer–Giedion syndrome (TRPS 2). Patients with TRPS 2 have additional features, including microcephaly, mental retardation, and multiple bony and cartilaginous exostoses (a hallmark of this variant) seen in early childhood. In addition, shortening of the hands and feet and redundant skin have also been reported in TRPS 2.
TRPS 3 is very rare and is similar to TRPS 1, as defined in 1984 by Sugio and Kajü. TRPS 3 can be considered a severe form of TRPS 1, but not a distinct entity.1,7 It differs from TRPS 1 with severe shortness in all phalanges and metacarpals, and is distinguished from TRPS 2 by not featuring mental deficiency and exostoses.3
The diagnosis of TRPS is primarily based on clinical and radiological findings. Confirmation with genetic analysis is helpful in cases of non-classical clinical presentations. However, genetic analysis cannot be regarded as the diagnostic gold standard.8
This case report is aimed to describe the clinical manifestations and dental management of TRPS 1 patient with multiple supernumerary impacted teeth within the knowledge seen in literature. No ethical approval was required because of the retrospective nature of this case report. Informed consent for publication of this article and its contents (photos) was obtained from the patient at the 4-year follow-up appointment.
Case presentationA 15-year-old female patient with a known medical history of TRPS 1 and a complaint of laceration of the tongue cause of teeth erupted in the palate visited our clinic. The Department of Orthopedics and Traumatology referred the patient at birth to the Department of Medical Genetics with symptoms of hyperlaxity of the joints, deformity of the hand and finger joints, dysmetria, dysdiadochokinesia, and delayed wound healing. The patient prediagnosed with Ehler–Danlos syndrome. The diagnosis of TRPS 1 was established at the age of 11 years based on physical examination findings, including left shoulder joint luxation, brachydactyly, deformity of the fingers, obesity, and craniofacial abnormalities supported by genetic analysis. A detailed family history is not medically relevant. This syndrome can be related to consanguineous marriage.
Extraoral examination revealed craniofacial abnormalities, such as sparse and thin hair, broad forehead, laterally 1/3 thin eyebrows, bulbous nose, long flat philtrum, thick vermilion border of the lips and prognathic mandible and some skeletal abnormalities, including short stature and short deformed fingers (clinobrachydactyly) (Fig. 1A, C and D). Radial deviation of the ring and little fingers and ulnar deviation of the second and third fingers were observed in both hands (Fig. 1). The patient's mental abilities were minimally impaired.
 frontal view of the patient; (B) radial and ulnar deviation of the distal phalanges; (C and D) profile views of the patient.")
Anterior open bite and bilateral posterior cross bite with dental crowding, retained maxillary deciduous second molars (55 and 65), high-arched palate, and mandibular prognathism were observed intraorally (Fig. 2).
. (A) Anterior open-bite with dental crowding; (B) high-arched palate; (C and D) bilateral posterior cross-bite with dental crowding.")
Radiographic examination revealed the presence of multiple impacted supernumerary teeth in mandible and maxilla. The number and the correct positions of the supernumerary teeth were determined using cone-beam computed tomography (CBCT). Radiographic images showed a total of 45 teeth: 2 deciduous, 32 permanent, and 11 supernumerary teeth. Six permanent teeth (teeth 18, 15, 25, 28, 38, and 48) and 11 supernumerary teeth in the posterior quadrants were impacted (Fig. 3).
.")
The patient had a history of malignant hyperthermia; therefore, precautions were taken to minimize the risk after consultation with the Department of Anesthesiology and Resuscitation. Four impacted third molar teeth, supernumerary teeth, retained deciduous teeth (55 and 65), and impacted maxillary left premolar (tooth 25) were removed under general anaesthesia (Fig. 4).

However, the impacted maxillary right premolar (tooth 15) was left, according to consultation with the Department of Orthodontics (Fig. 5). After four years, the patient was referred to our clinic again for surgical removal of the impacted maxillary right premolar as it prevented orthodontic tooth movement. The impacted maxillary right premolar (tooth 15) was removed under general anaesthesia. During the maintenance period, the patient was instructed to maintain oral hygiene.
Discussion.")
TRPS is a rare, multisystem disorder. The syndrome was first described by Klingmuller in 1950 and two cases were reported, but the details of the clinical and radiographic features of the disorder were described by Giedion in 1966.1
Individuals with TRPS 1 have slow-growing, fine, and sparse hair ranging from almost normal hair to severe diffuse alopecia, laterally sparse eyebrows, sparse eyelashes, bulbous tip of the nose, long flat philtrum, thin upper vermilion border, protruding ears, cone-shaped epiphyses of phalangeal bones and hip malformations.7 The patient reported in this study had most of the characteristic features of TRPS 1, but differentially thin upper lip and long flat philtrum were not observed.
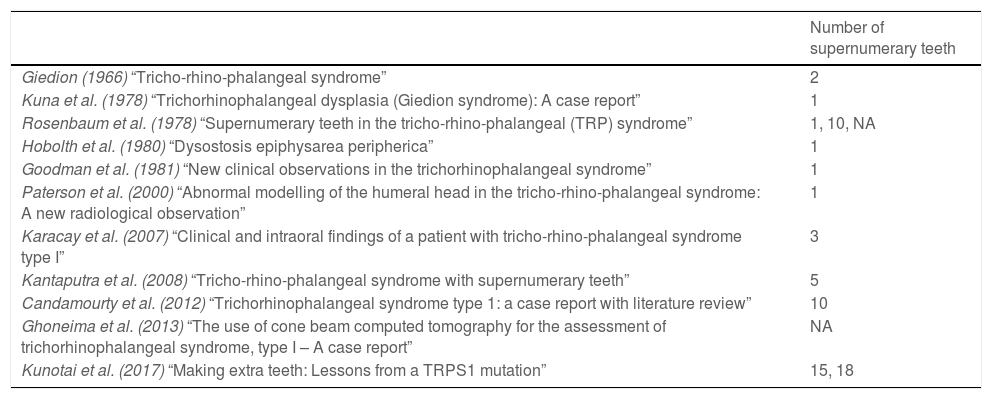
A variety of nonspecific intraoral findings have been reported in the literature, including microdontia, hypodontia, delayed tooth eruption, malocclusion, high caries index, high-arched palate, micrognathia, mandibular retrognathia, midface hypoplasia, and multiple impacted teeth.1–3 In addition, supernumerary teeth have been detected in several patients with TRPS, especially type 1.6,7 Fourteen affected patients with supernumerary teeth from 13 families have been reported. Among these, five patients had a single supernumerary tooth.2,9–12 Gideon reported two supernumerary incisors.4 Furthermore, multiple supernumerary teeth ranged from three in the bilateral premolar regions of the mandible3 to 18 in the premolar and molar regions of the maxilla and mandible, and missing right maxillary and mandibular premolars.5 Kantaputra et al.7 and Candamourty et al.6 reported patients with five and ten supernumerary teeth in the premolar and molar regions of the maxilla and mandible, respectively. Patient 1 in the study by Rosenbaum et al. had ten supernumerary teeth, eight in the anterior maxilla, and two in the premolar region of the mandible.12 Patient 1 in Kunotai et al. had 15 supernumerary teeth in relation to the maxilla and mandible.5 In addition, Rosenbaum et al. (Patient 2)12 and Ghoneima et al.1 reported an unstated number of supernumerary teeth in the posterior maxilla and mandible. Additionally, many cases of multiple supernumerary teeth involved both the maxilla and mandible, and four patients had ten or more teeth. The number of supernumerary teeth of patients with TRPS from literature summerized in Table 1. In our case, the most significant intraoral finding was multiple impacted supernumerary and permanent teeth (11 supernumerary teeth and eight permanent teeth) in both arches, related to TRPS 1. The presence of 14 TRPS 1 patients with supernumerary teeth seems significant. We believe that the existence of supernumerary teeth in patients with TRPS 1 is underreported. This might be related that supernumerary teeth are mostly impacted and impossible to realize without radiographic examination.
Number of supernumerary teeth of patients with TRPS from literature.
| Number of supernumerary teeth | |
|---|---|
| Giedion (1966) “Tricho-rhino-phalangeal syndrome” | 2 |
| Kuna et al. (1978) “Trichorhinophalangeal dysplasia (Giedion syndrome): A case report” | 1 |
| Rosenbaum et al. (1978) “Supernumerary teeth in the tricho-rhino-phalangeal (TRP) syndrome” | 1, 10, NA |
| Hobolth et al. (1980) “Dysostosis epiphysarea peripherica” | 1 |
| Goodman et al. (1981) “New clinical observations in the trichorhinophalangeal syndrome” | 1 |
| Paterson et al. (2000) “Abnormal modelling of the humeral head in the tricho-rhino-phalangeal syndrome: A new radiological observation” | 1 |
| Karacay et al. (2007) “Clinical and intraoral findings of a patient with tricho-rhino-phalangeal syndrome type I” | 3 |
| Kantaputra et al. (2008) “Tricho-rhino-phalangeal syndrome with supernumerary teeth” | 5 |
| Candamourty et al. (2012) “Trichorhinophalangeal syndrome type 1: a case report with literature review” | 10 |
| Ghoneima et al. (2013) “The use of cone beam computed tomography for the assessment of trichorhinophalangeal syndrome, type I – A case report” | NA |
| Kunotai et al. (2017) “Making extra teeth: Lessons from a TRPS1 mutation” | 15, 18 |
N/A: not available.
In the oral and maxillofacial region, mandibular retrognathism is a common finding in patients with TRPS 1.13 But there are a few studies reported that mandibular prognathism in patients with TRPS 1 in the literature.7,14 An anterior open bite with crowding, high-arched palate, and mandibular prognathism, which is a very rare finding in TRPS, was observed in this case. Orthognathic surgery was planned for this patient according to the consultation of the Department of Orthodontics, but the department of orthopedics did not allow for the operation because of recurrent dislocation of the joints. Therefore, only orthodontic treatment was performed to meet the aesthetic expectations of the patient.
Multiple supernumerary teeth are commonly associated with diseases or syndromes, such as cleft lip and palate, Gardner's syndrome, cleidocranial dysplasia, and Ehler Danlos. Therefore, establishing a differential diagnosis is important in such patients.15 The patient reported in this study was prediagnosed with Ehler–Danlos syndrome. After 11 years, the diagnosis of TRPS 1 was established based on physical examination and genetic analysis.
Dental management of patients with genetic disorders has become important in recent years. Treatment goals should be established by a multidisciplinary team that may include oral and maxillofacial surgeons, orthodontists, periodontists and prosthodontists. Treatment choices for these patients might include removal of supernumerary teeth, surgical exposure of impacted teeth, and orthodontic treatment to obtain an occlusion, and thus providing the patient with normal physiologic conditions and aesthetic satisfaction.15
ConclusionIn conclusion, we suggest that all patients with TRPS should undergo full clinical and radiographic oral examination and should be informed about the disease and the importance of dental counselling. From this viewpoint, we have reported our experience. We believe that our report may serve as a contribution to the literature because there are few studies about supernumerary teeth and long-term dental follow-up of patients with TRPS 1, while most of the cases in the literature have emphasized extraoral findings or chromosomal analysis of these patients.
Authors’ contributionsAll authors have made substantial contributions to the conceptions an design of the paper, acquisition of data or analysis and interpretation of data. CA drafted the article, and revised it critically for important intellectual content. SA and MA helped to draft the manuscript. All authors read and approved the final manuscript.
FundingThis research did not receive any specific grant from funding agencies in the public commercial, or not-for-profit sectors.
Conflicts of interestNone.


