





A twenty-six-year-old woman, with arthralgia and crepitation in her hands, feet and knees, and longstanding camptodactyly.1,2Personal history: bilateral myopia, retinal vitreous degeneration and sensorineural hearing loss since childhood. Family history: polyarthralgia, ophthalmological anomalies (retinal vitreous degeneration, retinal detachment, myopia and cataracts), hearing loss, scoliosis and similar phenotype in the paternal line3,4 (Fig. 1). Physical examination revealed marfanoid habitus, standard size, scoliosis, joint hyperlaxity (non-cutaneous),5 particular facial features (mediofacial hypoplasia, ocular proptosis, depressed nasal bridge, macrognathia)6 (Fig. 2A and B) and elongated fingers and toes with camptodactyly7 (Fig. 2D).
Diagnosis/progress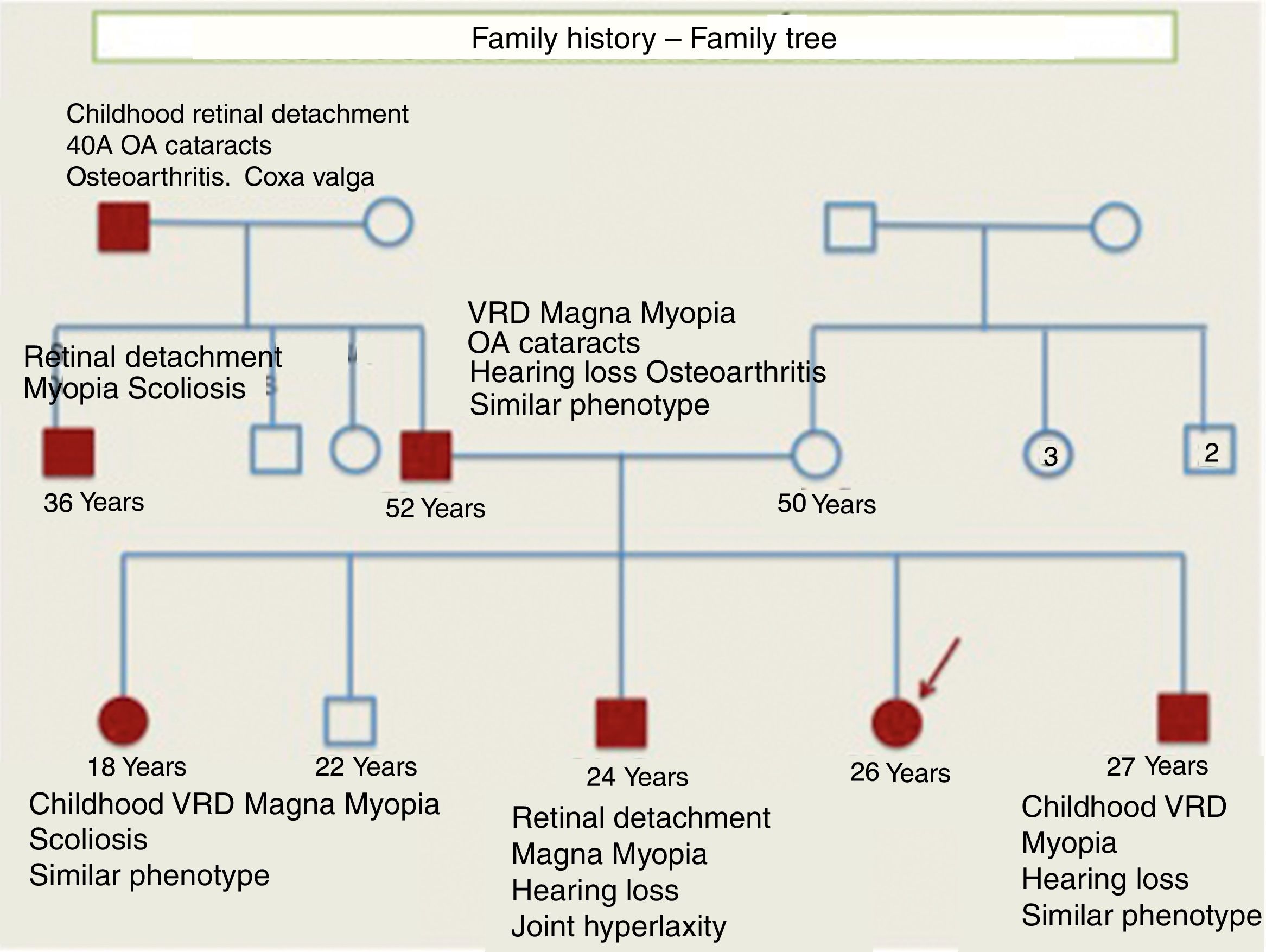

Blood tests: ESR 10mm/1st hour, CRP .3 (<.5mg/dl); normal haemogram and TSH/T4L, RF/negative autoimmunity (ANA, ENA, ANCA, ACPA). Radiology: scoliosis, increased metacarpal length (Fig. 2C). Normal knee MRI and echocardiography.
Given the possibility of hereditary collagenopathy we contacted the medical genetics department, who suspected Stickler syndrome, autosomal disease (AD), dominant and progressive.1,9 A molecular study of implicated genes was requested: COL2A1, COL11A1 and COL11A2,3,4,8–10 by means of next-generation sequencing (NGS) panel with detection of pathogenic heterozygous variant (not described) c.598C>T (p.Gln200) of the COL2A1 gene. Compatible familial segregation analysis (parents/siblings).3,8–10
DiscussionStickler syndrome (OMIM: 108300) is a hereditary and progressive connective tissue disorder characterised by skeletal abnormalities (arthralgia, joint hyperlaxity and scoliosis), ocular abnormalities (early-onset myopia, strabismus, cataract and retinal detachment), craniofacial abnormalities (midface hypoplasia, broad/flattened nasal bridge, cleft palate and macro/retrognathia) and sensorineural hearing loss.2,5–8,10 With an estimated incidence of 1/7500, this is a rare congenital collagenopathy, caused by mutation of the COL2A1 AD gene, of variable expressivity, even within the family.7–10 In spite of the time available in consultations, it is essential to take an adequate history in our routine practice. A personal and family history of ophthalmopathy and deafness, together with close collaboration with medical genetics were determining factors in the correct diagnosis, prognosis and final treatment of the patient and her family.
Conflict of interestsThe authors have no conflict of interests to declare.
The authors would like to express their gratitude for being able to collaborate in your journal and disseminate their article.
Please cite this article as: Gallo Puelles F, Serrano Anton AT, Lopez Gonzalez V, Hurtado Martinez J. Artralgias e hiperlaxitud articular en mujer con oftalmopatía y sordera precoz. Reumatol Clin. 2020;16:423–425.


