






The association of depression and chronic pain in knee osteoarthritis is a complex and difficult phenomenon to understand. In fact, establishing the order of appearance of these entities might result in an arduous task.
ObjectiveIn addition to analysing the relationship between preoperative anxiety and depression according to the results of total knee arthroplasty (TKA), we will assess the evolution of anxiety and depression symptoms.
Material and methodsA study of 260 patients with a mean age of 70.8 years. Patients were evaluated preoperatively and one year post-surgery completing the Knee Society Score (KSS), the Visual Analogue Scale (VAS), the Hospital Anxiety and Depression Scale (HADS) for the assessment of anxiety and depression, and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for quality of life.
ResultsThe mean scores of preoperative depression and anxiety decreased postoperatively from 6.55/7.63 to 4.96/5.96, respectively, a reduction that was statistically significant (P<.001). The differences between the preoperative scores and the 1-year scores of the different groups classified by HADS for both anxiety and depression were statistically significant (P<.001). The differences in VAS scores (P=.02) showed a significant improvement in patients with preoperative anxiety, in contrast to depressed patients.
ConclusionsTKA has proved to significantly decrease the preoperative levels of anxiety and depression. In patients with preoperative anxiety, the decrease in pain levels measured by the VAS was greater after TKA. Preoperative anxiety and depression did not influence the functional results of the TKA measured by the KSS.
La asociación de depresión y dolor crónico en la artrosis de rodilla es un fenómeno complejo y de difícil comprensión, en el que puede ser complicado establecer cuál de las dos entidades precedió a la otra.
ObjetivoAdemás de analizar la relación entre ansiedad y depresión preoperatorias y los resultados de la artroplastia total de rodilla (ATR), se valoró la influencia de la ATR en la evolución de la sintomatología de ansiedad y depresión.
Material y métodosUn total de 260 pacientes, con una edad promedio de 70,8 años, fueron evaluados preoperatoriamente y al año de la intervención, completando el Knee Society Score (KSS), la escala visual analógica (EVA), el Hospital Anxiety and Depression Scale (HADS) para valorar ansiedad y depresión, y el Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) para calidad de vida.
ResultadosLas puntuaciones medias de depresión/ansiedad preoperatorias descendieron de 6,55/7,63 a 4,96/5,96, respectivamente tras la cirugía, resultando estadísticamente significativas (p<0,001). Las diferencias entre las puntuaciones preoperatorias y anuales, de los distintos grupos ordenados por el HADS, tanto para la ansiedad como para la depresión, resultaron estadísticamente significativas (p<0,001). Las diferencias en las puntuaciones de la escala EVA fueron estadísticamente significativas (p=0,02) en los pacientes con ansiedad preoperatoria pero no en los deprimidos.
ConclusionesAunque la ansiedad y depresión preoperatorias no influyeron en los resultados funcionales de la ATR, sí se objetivó que la ATR mejoró significativamente los niveles de ansiedad y depresión. En pacientes con ansiedad preoperatoria, el descenso en los niveles de dolor medidos por la EVA fue mayor tras la ATR.
Pain and depression often coexist in medical practice. Sometimes depression occurs as a result of painful symptoms; however, chronic pain can also be a symptom of depression or increased by it.
This association poses a challenge for physicians, because the symptoms of the two entities can be confused, it being difficult to establish which of the two phenomena – depression or chronic pain – preceded the other, making an adequate therapeutic approach impossible or forcing this patient to do the rounds of the different specialists.
These patients whose primary complaint is pain, relatively often also suffer from a baseline depressive disorder, diagnosed or otherwise, and can be unfairly accused of scrounging, demanding and manipulating.
Joint replacement surgery is a proven procedure to treat pain in osteoarthritis of the knee that includes in its objectives improving quality of life.1–3
On reviewing the results of knee arthroplasty (TKA), a significant proportion of patients are observed – up to 20% in some series – in whom the persistence of chronic pain, disability, low quality of life and dissatisfaction cannot be explained by defects in the surgical technique or the implant.4
Preoperative mental health has been related to the results of TKA.5,6 Specifically, anxiety and depression prior to the surgical intervention have been described as factors associated with poorer outcomes after TKA. On the other hand, the literature also shows a decrease and therefore improvement in anxiety and depression rates in many patients following surgery.7–9
Because TKA is a procedure that can improve quality of like and increase the psychological wellbeing of patients by reducing levels of anxiety and depression, it is surprising that at the same time anxiety and depression have been considered predictors of poorer outcomes following TKA. Our hypothesis is that patients with anxiety and depression can achieve good outcomes after TKA through mental and physical improvement.
The principal aim of this study was to analyse the influence of preoperative anxiety and depression on TKA outcomes. The secondary aim was to evaluate the response that this surgical procedure might have on levels of anxiety and depression.
Material and methodsParticipants and procedureA longitudinal, observational, prospective, follow-up study was performed of a sample of primary TKA patients. An initial cohort of 265 patients was obtained.
The study was approved by the clinical research ethics committee of the General University Hospital of Ciudad Real. All patients signed an informed consent form prior to recruitment.
All the patients were implanted with a Duracon (Stryker) total knee prosthesis. The inclusion criterion for the study was advanced degenerative disease of the knee joint with clinical-radiological indication for prosthetic replacement. The preoperative diagnosis was osteoarthritic genu varus in 203 patients, osteoarthritic genu valgus in 18, gonarthrosis with no alteration of the mechanical axis in 21, gonarthrosis secondary to rheumatoid arthritis (RA), in 8 and condylar osteonecrosis in 10. The exclusion criteria of the study were: death (4 cases); under 50 years of age (one patient aged 37 with RA).
There were 8 patients (3.1%) with bilateral arthroplasty and there had been a period of more than 12 months between the two procedures; they were included as different patients.
All the patients were assessed preoperatively and one year after the intervention. Epidemiological data (age, sex, weight, height, diagnosis and laterality) and comorbidity were recorded in the preoperative assessment.
InstrumentsAt each of the assessments the patients completed the following questionnaires:
- 1.
Hospital Anxiety and Depression Scale10 (HADS), a self-assessment scale that detects states of anxiety and depression in non-psychiatric outpatient hospital departments. It comprises 2 subscales, each with 7 questions. Each item is assessed using a Likert-type response scale of 4 points (range 0–3), setting values from 0 to 21 for each of the subscales. The interpretation criteria are as follows: 0–7 (normal range or Non-case), 8–10 (doubtful case) and 11–21 (case of anxiety or depression).
- 2.
El Western Ontario and McMaster Universities Osteoarthritis Index11–13 (WOMAC) in its Likert-type version, comprising 24 questions, grouped into 3 domains. Five measure pain, 2 joint stiffness, and 17 assess difficulty in carrying out physical functions. It is a specific self-administered questionnaire that assesses quality of life in patients with osteoarthritis of the hip and knee. The total score can range from 0 to 96 points. The lower the score, the higher the quality of life.
- 3.
The visual analogue scale (VAS) was used as a measure of the subjective intensity of pain. It quantifies pain on a straight line of 10cm ranging from 0 to 10, which represents the worst pain imaginable.
- 4.
The Knee Society Score14,15 (KSS) was used to assess the specific results of the TKA, which consists of 2 subscales: own knee and function. Both subscales are assessed separately, with a maximum score of 100 points for each. The higher the score, the better the functional outcome.
- 5.
Degree of satisfaction with the result of the surgery: the patients were asked this during the annual assessment, which was categorised as poor, fair, good and very good.
The statistical analysis was performed using version 21.0 of the SPSS package.16 The normal distribution of the anxiety and depression variables was assessed using the Kolmogorov–Smirnov test. They were found to follow a non-normal distribution in most cases, and therefore in these cases primarily non-parametrical statistics were used. Descriptive analysis of the qualitative variables was defined by frequency distribution tables and bar graphs. The quantitative variables were studied using statistics of central tendency (mean, mode, median), of dispersion (standard deviation) and histogram graphs. The χ2 test was used to determine the association or independence of the variables, and ANOVA was used to compare the average values of the sample divided into various subsets. Variations observed over time were analysed by Friedman's test.
In the inferential analysis, P values <.05 were considered statistically significant differences.
ResultsFrom an initial sample of 265 patients, 5 patients were excluded, as previously mentioned. The final sample comprised 260 patients. Of these, 74.2% (n=193) were female and 25.8% (n=67) were male. The mean age was 70.8 years, and 83% of the patients were over 65 years old. There was no difference in laterality. Of the patients, 9.6% had documented treatment for anxiety and 8.8% for depression. These patients were not excluded from the study. The most relevant clinical characteristics of the sample are shown in Table 1.
Clinical characteristics of the sample (n=260).
| Frequencies | Percentages (%) | |
|---|---|---|
| Sex | ||
| Females | 193 | 74.2 |
| Males | 67 | 25.8 |
| Age | 70.86 (SD: 5.81) | |
| BMI | 32.13 (SD: 4.35) | |
| Laterality | ||
| Right | 130 | 50 |
| Left | 130 | 50 |
| History | ||
| HBP | 102 | 39.2 |
| Diabetes | 35 | 13.4 |
| Heart disease | 37 | 14.2 |
| COPD | 12 | 4.6 |
| Rheumatoid arthritis | 8 | 3.1 |
| Previous osteotomy | 13 | 5 |
| Contralateral TKP | 78 | 30 |
| Social support | ||
| Family | 118 | 45.4 |
| Partner | 104 | 40 |
| Other (alone, residential home, etc.) | 38 | 14.6 |
SD: standard deviation; COPD: chronic obstructive pulmonary disease; HBP: high blood pressure; BMI: body mass index; TKP: total knee prosthesis.
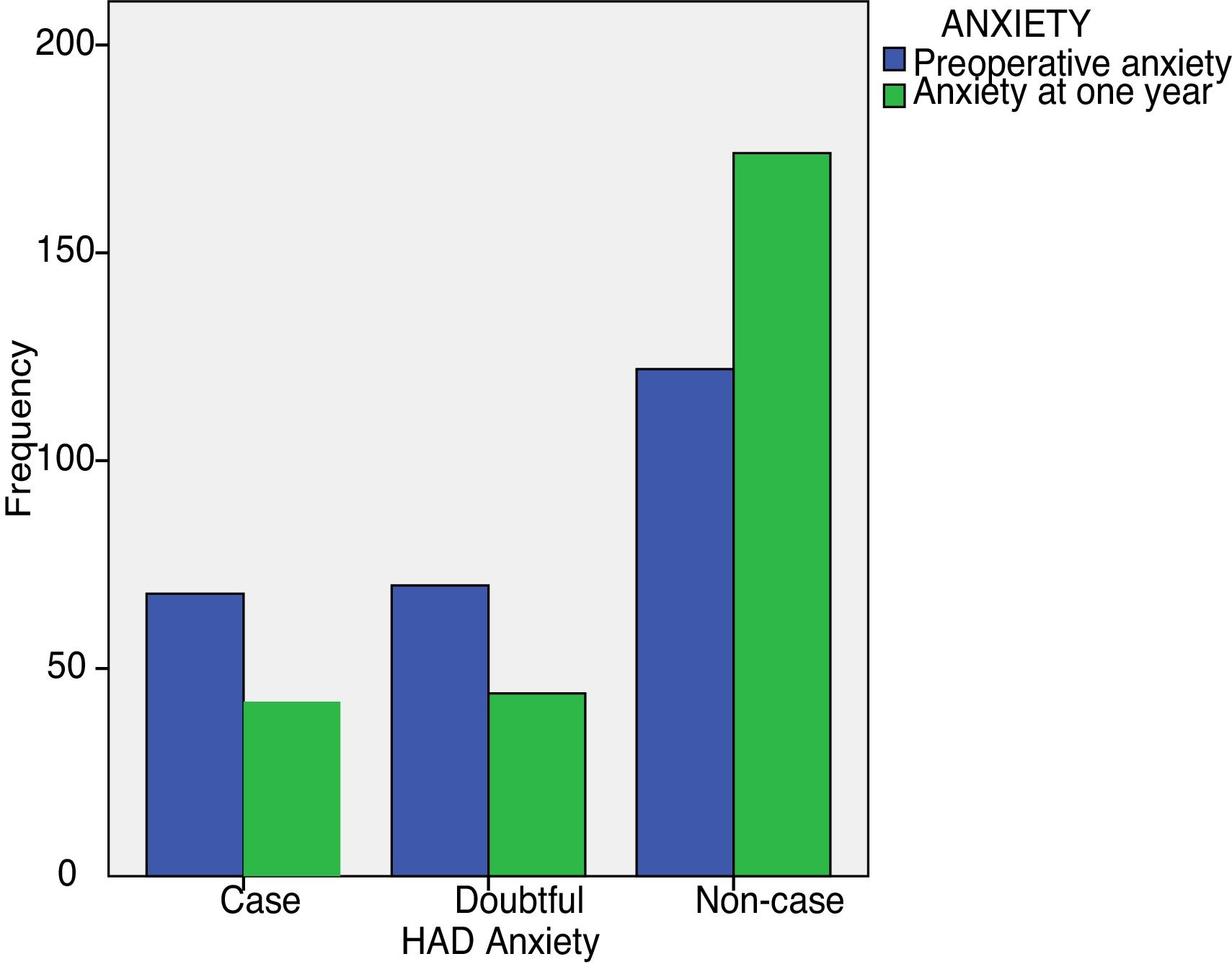
The number of patients with anxiety before the intervention was 68 and dropped to 42 at one year. With regard to depression, the total number of depressed patients was 35, and at one year it had fallen to 18. The mean score for preoperative anxiety was 7.63 and fell to 5.96 following the surgery. The mean preoperative depression score was 6.55 and had decreased at the annual check-up to 4.96.
The differences between preoperative levels of anxiety and depression and those obtained after surgery were statistically significant (P<.001) (Table 2).
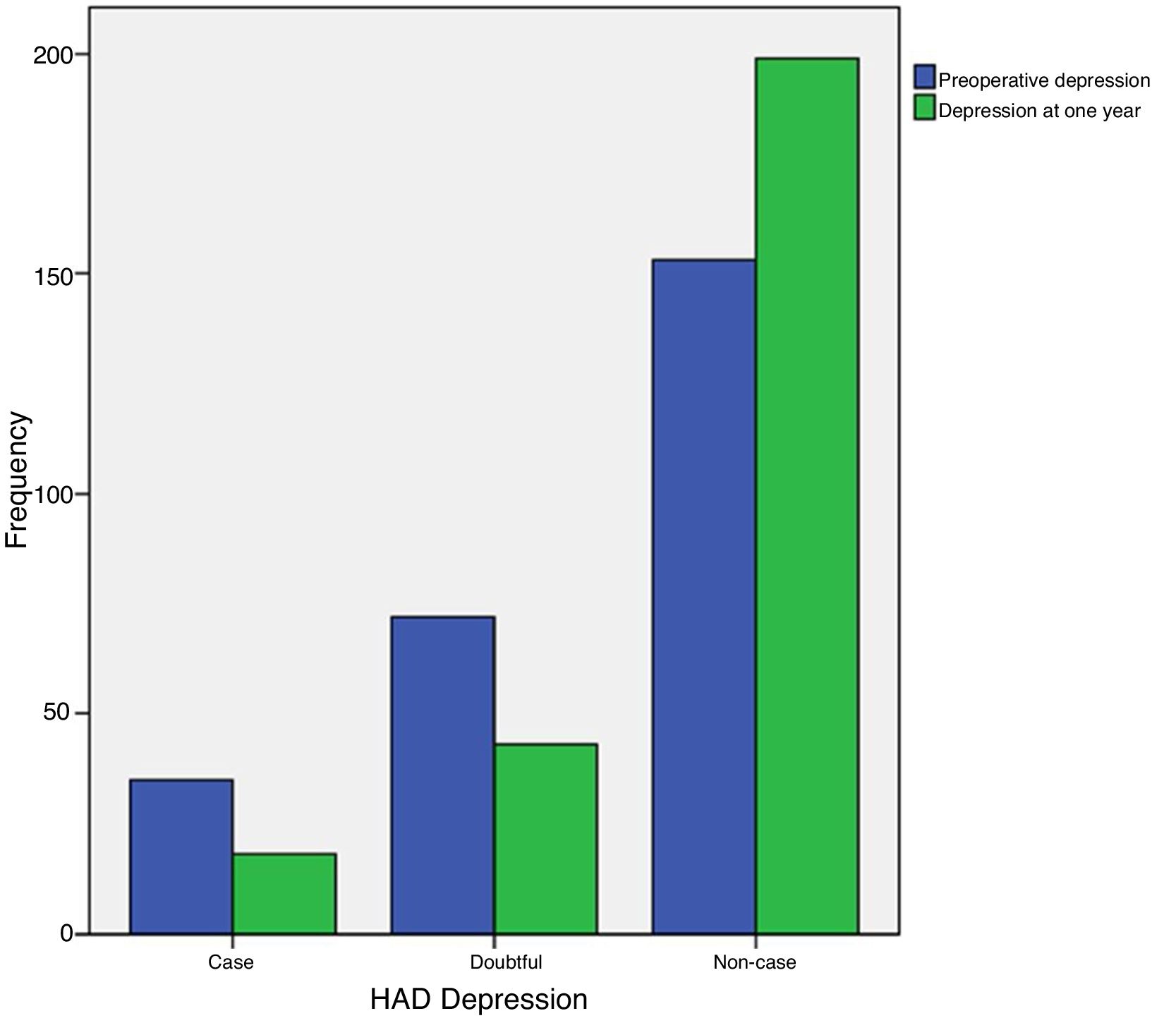
The HADS classifies patients as case (clearly anxious or depressed), doubtful (with some symptoms of anxiety or depression) and non-case (without anxiety or depression).
A total of 51 patients with some symptoms of anxiety improved. Of these, 26 were clearly anxious. The remaining 25 corresponded to the partial anxiety symptomatology group (P<.001) (Fig. 1).
A total of 46 patients with some depressive symptomatology improved. Of these, 17 were clearly depressed. The remaining 29 correspond to the group with partial symptomatology (P<.001) (Fig. 2).
The levels of preoperative anxiety in this sample did not influence quality of life, although statistical significance was close (P=.055) (Table 3). Preoperative depression did not influence quality of life (P=.876).
Anxiety describers/WOMAC. ANOVA.
| n | Mean | Standard deviation | 95% confidence interval | Sum of squares | Sig. | |||
|---|---|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||||
| Total WOMAC dif. | Case | 67 | −41.42 | 14.76 | −45.02 | −37.82 | 1184.89a | .055 |
| Doubtful | 70 | −35.63 | 14.51 | −39.09 | −32.17 | 52,142.51b | ||
| Non-case | 123 | −37.70 | 13.80 | −40.16 | −35.24 | |||
| Total | 260 | −38.10 | 14.35 | −39.85 | −36.35 | |||
| WOMAC dif. pain | Case | 67 | −9.00 | 3.36 | −9.82 | −8.18 | 108.26a | .019 |
| Doubtful | 70 | −7.24 | 3.98 | −8.19 | −6.29 | 3442.74b | ||
| Non-case | 123 | −8.30 | 3.62 | −8.95 | −7.65 | |||
| Total | 260 | −8.20 | 3.70 | −8.65 | −7.74 | |||
| WOMAC dif. stiffness | Case | 67 | −3.80 | 2.25 | −4.34 | −3.24 | 13.09a | .284 |
| Doubtful | 70 | −3.23 | 2.41 | −3.80 | −2.65 | 1328.05b | ||
| Non-case | 123 | −3.32 | 2.20 | −3.71 | −2.92 | |||
| Total | 260 | −3.42 | 2.28 | −3.69 | −3.14 | |||
| WOMAC dif. physical status | Case | 67 | −28.49 | 11.27 | −31.24 | −25.74 | 440.34a | .161 |
| Doubtful | 70 | −25.13 | 11.08 | −27.77 | −22.49 | 30,716.51b | ||
| Non-case | 123 | −25.87 | 10.66 | −27.77 | −23.97 | |||
| Total | 260 | −26.35 | 10.97 | −27.69 | −25.01 | |||
Dif.: differences; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Preoperative anxiety influenced pain levels measured on the VAS. The VAS scores, measure at one year following the intervention, showed a greater reduction in pain levels in the patients with preoperative anxiety than in those without anxiety (P=.02) (Table 4).
Anxiety describers/VAS-KSS. ANOVA.
| n | Mean | Standard deviation | 95% confidence interval | Sum of squares | Sig. | |||
|---|---|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||||
| VAS dif. | Case | 67 | −4.86 | 2.22 | −5.40 | −4.33 | 40.42a | .022 |
| Doubtful | 69 | −3.97 | 2.03 | −4.45 | −3.48 | 1335.07b | ||
| Non-case | 123 | −4.86 | 2.44 | −5.29 | −4.42 | |||
| Total | 260 | −4.62 | 2.30 | 4.90 | −4.34 | |||
| KSS diff. own knee | Case | 67 | 46.03 | 15.95 | 42.14 | 49.92 | 87.42a | .808 |
| Doubtful | 69 | 44.48 | 15.38 | 40.78 | 48.17 | 52,567.74b | ||
| Non-case | 123 | 45.54 | 12.70 | 43.27 | 47.80 | |||
| Total | 260 | 45.38 | 14.29 | 43.63 | 47.13 | |||
| KSS dif. function | Case | 67 | 26.19 | 18.09 | 21.78 | 30.61 | 108.34a | .860 |
| Doubtful | 69 | 24.57 | 20.68 | 19.60 | 29.53 | 91,838.18b | ||
| Non-case | 123 | 24.84 | 18.36 | 21.56 | 28.12 | |||
| Total | 260 | 25.12 | 18.88 | 22.81 | 27.43 | |||
Dif.: differences; VAS: visual analogue scale; KSS: Knee Society Score.
Anxiety in this study did not affect the functional outcomes of TKA measured with the KSS in the own knee subscale (P=.808) and function subscale (P=.860) (Table 4).
Preoperative depression did not influence differences in pain scores assessed by the VAS (P=.723), or the functional results of the own knee subscale (P=.448), or the functional subscale (P=.770).
Regarding degree of satisfaction, 84.2% (n=219) expressed an outcome classified as good or very good, while 15.8% (n=41) expressed a fair or poor result.
DiscussionThe presence of preoperative anxiety and depression is considered, at least by part of the medical literature, a predictor of poor outcomes following orthopaedic surgery. Complementarily, there are also studies that, after prosthetic replacement of a joint, observe an improvement in previous levels of anxiety and depression.
However, there also publications that report negatively on the relationship between psychological problems and surgical outcomes, as well as other studies that do not find mental improvement after surgery.
On analysing the references in an attempt to understand what is happening with such different outcomes, we found that a large number of different scales have been used. This might be why the outcomes are not interchangeable,17,18 and therefore apparently contradictory conclusions could be drawn.
Therefore we consider, in assessing the results of orthopaedic surgery, that the use of validated and specific questionnaires is necessary in any current clinical investigation.19
We used the HADS10 in our study to assess mental health, which allows us to detect anxiety disorders and depression with the advantage of not being contaminated by the symptoms of the patients’ physical disorder, in this specific case osteoarthritis of the knee.
The literature states that patients with chronic pain often feel depressed, anxious and have more physical complaints.20,21 When we focus on patients with osteoarthritis of the knee or hip, the publications22,23 also report a high prevalence of anxiety (43%) and depression (38%). The literature also describes percentages of anxiety and depression higher than those of our series (26.05%) and (13.40%), respectively, although in our case only patients with osteoarthritis of the knee and not the hip were included.
Equally notable are the high rates of anxiety (30.35%) and depression (50%) present postoperatively in TKA or total hip arthroplasty (THA) patients.23
There are studies9,24–27 that relate anxiety and/or depressive disorders with a lower degree of satisfaction after surgery, higher likelihood of developing complications of the surgical wound and/or higher costs in TKA implantation. Costs were not higher in patients with anxiety and depression when a TKA was implanted.
Unlike anxiety, preoperative depression appears to be related to poor results on functional knee scores,6,22 it being difficult to establish whether it is the severity of the osteoarthritis that is causing an increase in the level of depression or, by contrast, it is depression that is affecting the perception of symptoms, which would make patients feel the effects of their disease and end up scoring higher in the test.
Although the presence of pain and poor subjective function in patients who are to undergo TKA are considered predictors of preoperative anxiety and depression,28 the associations of these preoperative depressive symptoms with subsequent poor outcomes in pain and function is not clear in the literature.
In our series the patients with preoperative anxiety showed a significantly greater reduction in pain levels after TKA than those who did not.
By contrast, preoperative anxiety and depression did not influence the functional outcomes of TKA assessed using the KSS and, although close to statistical significance in the group of patients with anxiety, did not affect quality of life either (P=.055).
In the analysis of quality of life scores measured by WOMAC, it is surprising that the patients with preoperative anxiety did achieve significantly better results in the dimension of pain (P=.019), which indicates that studies with a greater number of cases could, hypothetically, reach statistical significance in this section on quality of life. These results could be explained by the fact that the perception of pain, both with the VAS scale and with the WOMAC pain dimension, was higher in the patients with anxiety.
In our study, TKA managed to improve the psychological status of the patients, statistically significantly reducing preoperative levels of anxiety (preoperative HADS-A 26.05% and 16.1% at one year) and depression (preoperative HADS-D 13.40% and 6.9% at one year). These results are similar to those obtained by Cho et al.7 in a study of shoulder arthroplasties, Pietrzak et al.8 following arthroplasty in patients with RA and Duivenvoorden et al.9 in a combined study on TKA and THA. In all these studies the number of patients with preoperative anxiety and depression reduced after the intervention. Unlike our results, the paper by Riddle et al.29 found no reduction in depressive symptoms after a procedure like TKA.29
The literature includes papers like that of Blackburn et al.30 who, confirming our results in the reduction of post-operative anxiety and depression, observed – unlike our series – an improvement in the functional outcomes of the knee at 3 and 6 months following the intervention. However, this was a sample of only 40 TKAs and used a different assessment questionnaire used, the Oxford Knee score.30
Our study, like that of the abovementioned authors,7–9,30 shows that joint pain in the knee, hip and shoulder would contribute to the onset of psychological symptoms. We could infer from our results that a successful TKA would offer an excellent opportunity to improve both the soma and the psyche It would confirm the hypothesis that patients with anxiety and depression in this study would achieve the same good outcomes following TKA as the rest of the patients in the sample, and that mental health would be improved through physical improvement.
We agree, therefore, that the difficulty in interpreting preoperative anxiety and depression and the outcome of TKA lies in establishing whether they are the cause or effect of knee pain, and that the different methods for assessing results are not necessarily interchangeable. The eminently mechanistic nature of our specialty could imply a limitation of the study, and undoubtedly, new trials that include the implementation of pre- and postoperative psychological therapies31 by mental health professionals could contribute to better control that would prevent possible biases during follow-up.
ConclusionsPreoperative anxiety and depression in this study did not influence the functional outcomes of TKA as measured by the KSS or the quality of life as assessed by the WOMAC questionnaire.
TKA reduced preoperative levels of anxiety and depression.
The differences between the preoperative and the annual scores of the different groups – case, non-case and doubtful case – classified by the HADS, both for anxiety and depression, were statistically significant (P<.001) (Figs. 1 and 2).
The patients with preoperative anxiety showed a greater, statistically significant reduction in pain levels assessed with the VAS scale after arthroplasty.
Conflict of interestsThe authors have no conflict of interests to declare.
To Mrs María de los Ángeles Toro López and Dr Antonio López Alonso, for their invaluable encouragement and support in undertaking this study.
Please cite this article as: Jiménez Ortiz M, Espinosa Ruiz A, Martínez Delgado C, Barrena Sánchez P, Salido Valle JA. ¿Influye la ansiedad y depresión preoperatorias en los resultados de la artroplastia de rodilla? Reumatol Clin. 2019. https://doi.org/10.1016/j.reuma.2018.06.008


