


Juvenile idiopathic arthritis (JIA) is a chronic autoimmune disease characterised by the presence of arthritis in children under 16 years of age for more than 6 weeks in the absence of any other known cause.
The extra-articular manifestations, especially in the audiovestibular system, are related to the involvement of the joints of the ossicular chain as a result of the inflammatory process in the synovium. Previous clinical studies in paediatric patients have shown conductive or sensorineural hearing loss.
ObjectiveThe aim of this study was to assess the frequency of hearing impairment and of associated factors in patients with JIA.
MethodologyA prospective, analytical study was conducted from January 2013 to August 2014 in 62 patients with JIA aged between 5 and 15 years. The study was approved by the local ethics committee and parents signed their informed consent. All subjects underwent audiological examination involving otomicroscopy, audiometry, tympanometry, stapedius reflex and test for transient otoacoustic emissions (TOAE); rheumatologic evaluation included joint examination and the application of a measure of functional ability (disability) using the Childhood Health Assessment Questionnaire (CHAQ).
Measures of central tendency and of dispersion were used (chi-square for associations and P<.05 for statistical significance).
ResultsSixty-two patients were included: 56 girls and 6 boys, mean age 11.9 years and mean disease duration of 3.4 years; 46% had rheumatoid factor (RF)-positive polyarticular JIA, 40% had RF-negative polyarticular JIA, 15% had disease of systemic onset and 3% had oligoarthritis. Active disease was found in 29 patients and 33 were in remission with medication.
Of the total of 124 ears evaluated according to the Jerger classification for tympanometry, abnormal findings were observed in 78 that were type As and in 1 that was type Ad, whereas there were 45 type A ears. Hearing loss was disclosed by speech audiometry, rather than by pure tone audiometry. The TOAE were absent in 4% of those assessed and the stapedius reflex was absent in less than 10%.
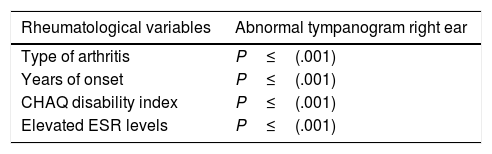
Factors that had a positive correlation with hearing impairment were RF-positive polyarticular JIA, disease duration, degree of disability and the erythrocyte sedimentation rate level (P<.000).
ConclusionThe presence of an abnormal tympanogram suggested early involvement in the structure of the tympanic-ossicular complex; however, 3.4 years later, no hearing loss had been reported.
La artritis idiopática juvenil (AIJ) es una enfermedad autoinmune de curso crónico, caracterizada por la presencia de artritis en menores de 16 años, por más de 6 semanas en ausencia de otra causa conocida.
La expresión extra articular en el sistema audiovestibular se relaciona con la afección de las articulaciones de la cadena oscicular, como consecuencia del proceso inflamatorio de la membrana sinovial. Estudios previos realizados en población infantil han reportado que la pérdida auditiva puede ser de tipo neurosensorial y/o conductiva.
ObjetivoDeterminar la frecuencia de la afección auditiva y los factores asociados en los pacientes con AIJ.
MetodologíaEstudio prospectivo y analítico. Se incluyó a 62 pacientes con AIJ con edades comprendidas entre 5 y 15 años, a partir de agosto del 2013 a enero del 2014. El estudio fue aprobado por el comité de ética local y los padres firmaron el consentimiento bajo información.
Se realizó otoscopia microscópica, audiometría tonal, timpanometría, reflejo estapedial y emisiones otoacústicas transitorias (EOT); la evaluación reumatológica incluyó exploración articular y aplicación de cuestionario para la evaluación del estado de salud en la infancia (CHAQ).
Se utilizaron medidas de tendencia y de dispersión; asociación χ2 con una p<0,05 para la significación estadística.
ResultadosSe incluyó a 62 pacientes; 56 niñas y 6 niños, edad media 11,9 años, duración media de la enfermedad de 3,4 años; el 46% presentó AIJ poliarticular factor reumatoide (FR) positivo; el 40%, AIJ poliarticular FR negativo; el 15% AIJ sistémica y el 3% oligoarticular. Se encontró enfermedad activa en 29 pacientes y 33 en remisión con medicamentos.
Se evaluaron en total 124 oídos; en 78 se encontró curva tipo As de la clasificación de Jerger, curva tipo A en 45 y en uno se reportó curva tipo AD. En la audiometría tonal no se encontró hipoacusia en ningún paciente y esta estuvo acorde con la logoaudiometría. Las EOT se encontraron ausentes en el 4% de los evaluados y sin reflejo estapedial en menos del 10%.
Los factores que presentaron una asociación con la afección auditiva fueron la variedad poliarticular FR positivo, el tiempo de evolución, el índice de discapacidad y los niveles de VSG (p<0,001).
ConclusiónSe encontró en más de la mitad de los pacientes estudiados alteraciones auditivas presentes en el timpanograma, asociadas con la variedad poliarticular FR positivo, tiempo de evolución, actividad de la enfermedad y la elevación de la VSG.
Juvenile idiopathic arthritis (JIA) is one of the most common autoimmune diseases in children involving major short and long-term disability.
Involvement of the temporomandibular joint and audiovestibular system (incudomalleolar and incudostapedial joints) is reported of between 31% and 55% in studies performed on children with JIA.1,2 This involvement can be related to vasculitis, neuritis, drug ototoxicity, or immune deposit accumulation.3–5 Tympanometry is a sensitive tool, of great diagnostic value in detecting anomalies of the middle ear especially in children and young people.6 Clinically it manifests as hearing loss, which can be sensorineural and/or conductive, with type As and C curves according to Jerger's classification, and high air conduction thresholds.1,2
The ear is most affected by systemic onset.
The objective of this study was to establish the frequency of hearing involvement and associated factors in patients with JIA.
Material and MethodsA prospective study was undertaken of a case series of patients aged between 6 and 16, diagnosed with JIA based on the criteria of the International League against Rheumatism (ILAR) of the Paediatric Rheumatology Department of the UMAE Hospital General, Dr. Gaudencio González Garza, of the La Raza National Medical Centre between August 2013 and January 2014, after approval by the local ethics committee.
A paediatric ENT specialist and an audiologist performed the audiological assessment, which included: microscopic Otoscopy, tonal audiometry, tympanometry, stapedius reflex, and transient otoacoustic emissions (TOAE).
The audiological equipment was: optical light microscope; Interacoustics Audiometer AD229E; for the tympanometry: GSI TYMPSTAR, Middle ear Analyzer; for measurement of auditory evoked potentials: ICS chartr EP 200 optometrics; to measure otoacoustic emissions: Otometrics CAPELLA.
Paediatric rheumatologists performed the rheumatological assessment, which included a joint examination, using the Childhood Health Assessment Questionnaire (CHAQ); mild .13, moderate .63 and severe disability ≥1.75. Disease activity and remission were assessed based on clinical and laboratory parameters (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]). Patients with arthritis and/or effusion with limited movement, and elevated ESR and/or CRP were defined as having active disease. For systemic onset, the presence of fever, hepatosplenomegaly and adenomegalies was considered. The absence of active arthritis for more than 6 months with medication was considered remission of the disease with medication, and remission of the disease without medication when the patient had had no active arthritis for a minimum of one year after discontinuing treatment.
The demographic data and treatment used at the time of the study were taken from the clinical records.
Patients with a history of acute otitis media, at least 2 months prior to the audiological assessment, and those using ventilation and/or drainage systems for at least 6 months prior to the study were excluded.
Statistical AnalysisSPSS version 15.0 was used to analyse the results, obtaining the frequency distribution, mean and standard deviation. Ranges (minimum–maximum) and χ2 test were used for associations in nonparametric variables.
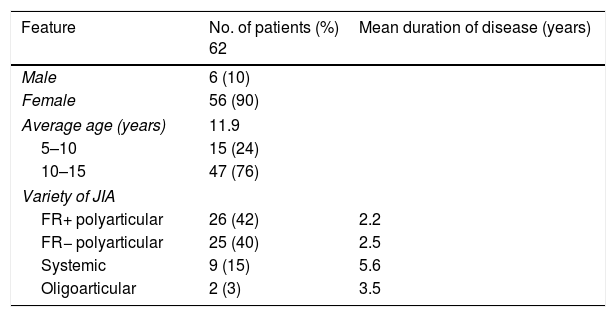
ResultsSixty-two patients were included in the study, 56 girls and 6 boys, mean age of 11.9 years, with mean disease duration of 3.4 years. In terms of disease onset, 26 patients (42%) were rheumatoid factor (RF)-positive polyarticular, 25 (40%) RF-negative polyarticular, 9 (15%) systemic, and 2 (3%) oligoarticular (Table 1).
Demographic Features of the Patients With JIA.
| Feature | No. of patients (%) 62 | Mean duration of disease (years) |
|---|---|---|
| Male | 6 (10) | |
| Female | 56 (90) | |
| Average age (years) | 11.9 | |
| 5–10 | 15 (24) | |
| 10–15 | 47 (76) | |
| Variety of JIA | ||
| FR+ polyarticular | 26 (42) | 2.2 |
| FR− polyarticular | 25 (40) | 2.5 |
| Systemic | 9 (15) | 5.6 |
| Oligoarticular | 2 (3) | 3.5 |
Ninety-five percent of the patients were being treated with methotrexate, 20 (32%) biological therapy, 11 (18%) cyclosporine, 7 (11%) chloroquine, and 7 (11%) prednisone.
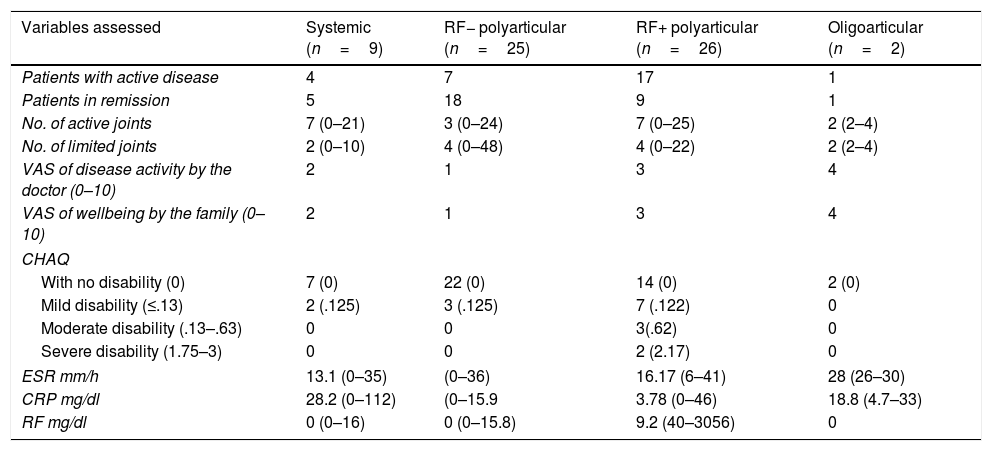
The degree of disability was mild for 12 patients, moderate for 4, and severe for 2 (Table 2).
Clinical and Laboratory Features of the Patients With JIA.
| Variables assessed | Systemic (n=9) | RF− polyarticular (n=25) | RF+ polyarticular (n=26) | Oligoarticular (n=2) |
|---|---|---|---|---|
| Patients with active disease | 4 | 7 | 17 | 1 |
| Patients in remission | 5 | 18 | 9 | 1 |
| No. of active joints | 7 (0–21) | 3 (0–24) | 7 (0–25) | 2 (2–4) |
| No. of limited joints | 2 (0–10) | 4 (0–48) | 4 (0–22) | 2 (2–4) |
| VAS of disease activity by the doctor (0–10) | 2 | 1 | 3 | 4 |
| VAS of wellbeing by the family (0–10) | 2 | 1 | 3 | 4 |
| CHAQ | ||||
| With no disability (0) | 7 (0) | 22 (0) | 14 (0) | 2 (0) |
| Mild disability (≤.13) | 2 (.125) | 3 (.125) | 7 (.122) | 0 |
| Moderate disability (.13–.63) | 0 | 0 | 3(.62) | 0 |
| Severe disability (1.75–3) | 0 | 0 | 2 (2.17) | 0 |
| ESR mm/h | 13.1 (0–35) | (0–36) | 16.17 (6–41) | 28 (26–30) |
| CRP mg/dl | 28.2 (0–112) | (0–15.9 | 3.78 (0–46) | 18.8 (4.7–33) |
| RF mg/dl | 0 (0–16) | 0 (0–15.8) | 9.2 (40–3056) | 0 |
CHAQ: Childhood Health Assessment Questionnaire; VAS: visual analogue scale; RF: rheumatoid factor; CPR: C-reactive protein; ESR: erythrocyte sedimentation rate.
The disease was active in 29 patients, and 33 were in remission with treatment.
Audiological TestsA total of 124 ears were assessed; no hearing symptoms were reported for any of the patients. Impacted ear wax was found in 17 ears on otoscopy. Type As curves were found in 78 ears, type A in 45, and type AD in one, no conductive and/or sensorineural hearing loss was recorded in any of the patients. Seventeen patients with abnormal tympanograms (type As curve) were found to have active joint disease. Speech audiometry revealed up to 100% phonemic discrimination at 40 and 60dB HL, which is in line with the pure-tone threshold obtained in the audiological study.
The transient evoked otoacoustic emissions test resulted as absent unilaterally in 2 patients, and bilateral in 3.
The stapedius reflex was unilaterally absent in 5 patients, 2 with systemic onset, 2 with RF-positive polyarticular, and one with RF-negative polyarticular JIA. It was found to be absent bilaterally in 6 patients, 2 of these patients had RF-positive polyarticular, and 4 had RF-negative polyarticular JIA. These patients had Eustachian tube dysfunction on active manoeuvres only (Williams test). The audiological tests are shown in Fig. 1.

The association between the audiological tests, the clinical and laboratory features of the disease reported statistical significance between the type As tympanogram curves and the variety of arthritis, years of progression, degree of disability, and ESR levels for the right ear only (P=.001) (Table 3).
DiscussionThere are few studies worldwide on hearing loss, and the participation of the middle ear in children with JIA.1,2 The nature of hearing disability, and impaired middle ear function in patients with RA is controversial, and its scope has not yet been fully clarified. Some authors report sensorineural, conductive and/or mixed hearing loss in children and adults.3–5,7 In the study by Siamopoulou et al., hearing function was assessed by tympanometry, correlating the findings with the onset, activity and severity of disease. They found abnormal tympanometric patterns in 55.5% of their patients (reported as type As and C curves according to Jerger's classification), principally in the systemic (66%) and polyarticular (60%) varieties.
Like Siamopoulou et al., in our study we found that more than half the ears showed type As curves (63%), principally in the patients with RF-positive polyarticular onset, with a statistically significant correlation with the arthritis onset, duration of the disease, its activity, degree of disability and elevated ESR levels. This might be explained by the presence of synovitis in the incudomalleolar and incudostapedial joints, which might result in reduced movements of the diarthrodial joints of the middle ear.1 However these changes in our patients were not sufficient to cause conductive and/or sensorial hearing loss.
In the particular case of the 2 patients with the oligoarticular form, and the presence of this curve, we found no association attributable to the disease, and the rest of the audiological tests were normal.
The test for transient otoacoustic emissions (TOAE), showed them to be absent unilaterally in 2 patients, and bilaterally in 3; this might be attributed to Eustachian tube dysfunction, since these patients had impacted ear wax. TOAE might not even be present in 40% of the normal-hearing population, and does not necessarily show a pathological process.
The absence of stapedius reflex was confirmed in 11 patients, 5 unilaterally and 6 bilaterally. However, the audiological study, tympanometry and otoscopy were normal, therefore isolated absences do not reflect hearing involvement. The studies by Siamopoulou et al., and Omer et al. did not report an absence of this reflex. Despite the abnormal tympanograms of more than half the patients, the evoked otoacoustic potentials were absent in only 4% of the population, and a stapedius reflex was absent in less than 10%.
ConclusionsOf the population studied, 63% had an abnormal tympanogram, which indicates early involvement of the structure of the tympano-ossicular complex; although in this study no conductive and/or sensorial hearing loss was encountered. The factors found to be associated with abnormal tympanometry were: time of onset, RF-positive polyarticular onset, disease activity, and elevated ESR.
Lines of research are necessary for follow-up of potential audiological complications associated with JIA long term.
Ethical DisclosuresProtection of people and animalsThe authors declare that the research was carried out according to the ethical standards set by the responsible human experimentation committee, the World Medical Association and the Helsinki Declaration.
Data confidentialityThe authors declare that they have complied with their work centre protocols for the publication of patient data.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects referred to in the article. This document is held by the corresponding author.
Conflict of InterestsThe authors have no conflict of interests to declare.
Please cite this article as: Céspedes Cruz AI, Méndez Núñez M, Solís Vallejo E, Zeferino Cruz M, Torres Jiménez AR, Ocampo Sánchez V, et al. Frecuencia de la afección auditiva y los factores asociados en pacientes con artritis idiopática juvenil. Reumatol Clin. 2019;15:152–155.


