










Biologics have shown greater efficacy than traditional treatments in patients with rheumatoid arthritis, although some cannot be administered on an outpatient basis. Day hospitalization requires the patient to attend the hospital for a few hours to receive those treatments that cannot be administered on an outpatient basis or that do not justify admission to hospital. Few studies have analyzed the situation of Rheumatology Day Hospitals (RDH) in Spain. The HD-Reumatolex project aims to evaluate the situation of Spanish RDHs in terms of strategy, training, management, and quality of care.
Material and methodsThe project was based on a “model of excellence in RDH” design, which made it possible to perform a comparative analysis (benchmarking) of 21 Rheumatology Departments. The 19 criteria evaluated were divided into 3 categories: Strategic processes, Key processes, and Support processes.
ResultsThe lowest mean scores were recorded for follow-up of clinical practice guidelines/recommendations and existence of a quality plan (Strategic processes), criteria for training among RDH professionals (Support processes), and admission and discharge (Key processes). Five RDH achieved the benchmark when the position obtained by the RDH in Key processes was plotted against the one obtained in Strategic processes and Support processes. One RDH emerged as a clear leader in the comparison.
ConclusionsNone of the RDH obtained the total maximum score at the category level or at the total results level, thus revealing room for improvement in the attainment of excellence for all the participating centers.
Los tratamientos biológicos han superado en eficacia a los tratamientos tradicionales de la artritis reumatoide, aunque algunos no pueden administrarse de forma ambulatoria. La hospitalización de día supone la asistencia hospitalaria durante unas horas para aquellos tratamientos que no pueden realizarse en la consulta externa ni justifican el ingreso del paciente. Existen pocos estudios que analicen la situación de los Hospitales de Día de Reumatología (HDR) en España. El proyecto HD-Reumatolex tiene como objeto evaluar la situación de distintos HDR españoles desde una óptica estratégica, formativa, de gestión y de calidad asistencial.
Material y métodosSe diseñó un «Modelo de excelencia en HDR» que sirvió como base para realizar un análisis comparativo y anónimo (benchmarking) entre 21 Servicios de Reumatología. Se valoraron 19 criterios, clasificados en 3 categorías: Procesos estratégicos, Procesos clave y Procesos de soporte.
ResultadosLos aspectos con peor puntuación media fueron los de seguimiento de guías de práctica clínica y existencia de un plan de calidad (Procesos estratégicos), formación de los profesionales del HDR (Procesos de soporte), y admisión de pacientes y procedimiento de alta (Procesos clave). Cinco HDR alcanzaron el benchmark al representar gráficamente su posición en los Procesos clave frente a los estratégicos y a los de soporte. Un HDR se posicionó como líder indiscutible en el análisis comparativo.
ConclusionesNinguno de los HDR consiguió la puntuación máxima total, ni a nivel de categoría ni de resultados totales. Esto significa que existen oportunidades de mejora hacia la excelencia para todos los HDR participantes.
The appearance of biologics has been a major therapeutic advance and a remarkable improvement in the prognosis of inflammatory rheumatic diseases such as rheumatoid arthritis (RA), psoriatic arthritis and spondyloarthropathies, as well as an improvement in the quality of life of patients who have these diseases.1 These drugs have a clinical efficacy that has surpassed traditional treatments and, in the case of RA, have allowed a delay in structural2 damage. The drugs come in subcutaneous and intravenous presentations, and some of them cannot be administered on an outpatient basis.
It is understood that “Day Hospital” (DH) accounts for hospital care lasting a few hours, either for diagnostic, clinical or multiple tests or treatments that cannot be performed as an outpatient or justify hospitaizationl.3,4 Thus, the patient receives treatment with biological drugs and receives the same service as if hospitalized, but without being so, thereby reducing the associated risks and costs.4 For this reason, in recent years there has been an increase in the number of day hospitals in Spain, some of which are dedicated to a single specialty or some of which are polyvalent, i.e., jointly attending patients of different specilties.3,4 Also, Rheumatology Day Hospital (RDH) may allow for other tasks, such as informing and educating the patient, giving psychosocial support or running clínical4 trials, thus favoring the scientific production of Rheumatology.
The Ministry of Health, through the Task Force for the preparation of “Standards and Recommendations of Day Hospitals”, published in 2009 standards and recommendations for the DH.3 These are not normative, but rather seek to make available to the government, managers and caregivers, common criteria for such units to improve safety and the quality of their practice. These recommendations include issues relating to the rights and guarantees of the patient, their safety, organization and management of the Day Hospital, its structure, material and human resources, as well as the quality of care provided.
As other publications have manifiested,3,4 there are few studies analyzing the situation of Day Hospitals in Spain. Some have described the situation in certain Autonomous Communities5 RDH, with interesting results that could serve as a point of comparison for other regions. Further analysis is therefore needed to help plan strategies to optimize the use of RDH in our country.
ObjectivesThe objective of the DH-Reumatolex project is to evaluate the current status of various Spanish RDH's from a strategic, training, management and quality of care perspective, in order to design action plans that focus on the RDH and the rheumatologist's role within it.
Materials and MethodsThe HD-Reumatolex project was carried out between 2008 and 2009 and involved the design of a “model of excellence in HDR” which served as a basis for anonymous comparative analysis and benchmarking among the 21 Spanish Rheumatology departments listed in Table 1. These 21 centers with a RDH were available and agreed to join the initiative, with 8 corresponding to autonomous regions. In the case of participating hospitals, 86% (n=18) were large hospitals (>601 beds) and 43% (n=9) counted over 10 rheumatologists in their departments. Most of the RDH (66%, n=14) presented a polyvalent model of DH, 29% (n=6) responded to an Rheumatology model and 5% (n=1) to a model limited to the administration of biologic therapies. Each participant was randomly assigned a number to perform a comparative analysis anonymously.
Participating Rheumatology Departments in the DH Reumatolex Project, Listed Alphabetically.
| Corporació Sanitària Clínic, Barcelona |
| Hospital General Universitario de Alicante |
| Hospital de Basurto, Bilbao |
| Hospital Universitario Bellvitge, Barcelona |
| Hospital Universitario de Canarias, Tenerife |
| Hospital Universitario 12 de Octubre, Madrid |
| Hospital Doctor Peset, Valencia |
| Hospital General Universitario Gregorio Marañón, Madrid |
| Hospital Universitario Juan Canalejo, La Coruña |
| Hospital Universitario La Paz, Madrid |
| Hospital Universitario La Princesa, Madrid |
| Hospital del Mar, Barcelona |
| Hospital Universitario Puerta de Hierro, Madrid |
| Hospital Universitario Reina Sofía, Córdoba |
| Hospital de la Santa Creu i Sant Pau, Barcelona |
| Hospital Universitario Clínico de Santiago de Compostela |
| Hospital Universitario Vall d’Hebron, Barcelona |
| Hospital Universitario Virgen de la Arrixaca, Murcia |
| Hospital Universitario Virgen de la Macarena, Sevilla |
| Hospital Universitario Virgen de las Nieves, Granada |
| Hospital Universitario Virgen del Rocío, Sevilla |
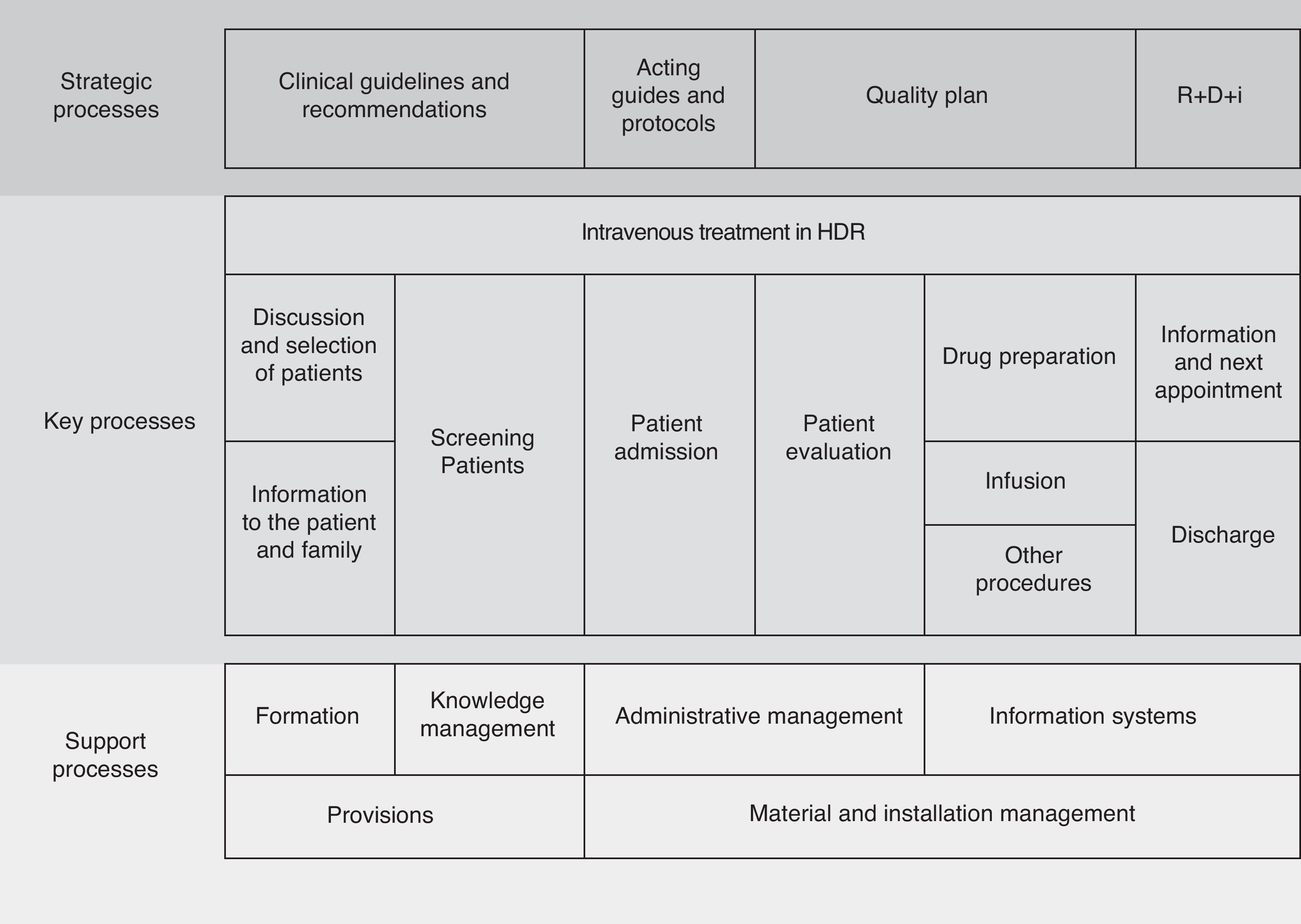
The project consisted of the following phases: (1) design of a “model of excellence in RDH” self-assessment questionnaire. This is not based on any previous model. Its definition was elaborated by three rheumatologists and subsequently validated by another 18 other rheumatologists using an IDEFO process methodology, (2) commitment to the initiative and elaboration of the questionnaire, and (3) analysis of the benchmarking results. The self-assessment questionnaire, based on a map process is detailed in Fig. 1, was completed by participants RDH to know in detail their situation in that context.
In order to define the basis of the project and the questionnaires, previously there was a meeting with three expert clinical rheumatologists who preliminarily evaluated biological management in RDH.
Criteria EvaluatedWe evaluated a total of 19 criteria, ranked in three categories: “Strategic Processes”, “Key Processes” and “Support processes”, which were assigned different weights depending on their importance (Table 2). Thus, the category ‘key processes’ had greater weight because of its role in patient care, essential for clinical outcomes.
Within the category of “Strategic Process”, criteria such as tracking clinical practice guidelines and recommendations, the existence of protocols/guidelines for action, a quality plan, or research, development and innovation (R+D+i) in the RDH were evaluated. The criteria considered in the “key processes” category were patient selection, information/training provided to patients and families, patient screening, admission and assessment, medication preparation, infusion procedures or other diagnostic procedures-therapeutics processes and next appointments, as well as intravenous treatment in the RDH. Finally, in the category “Support processes” we evaluated criteria such as RDH staff training, knowledge management, administrative management, information systems, procurement and materials management or facilities.
Analysis of ResultsTo analyze the results, maximum score per criterion or category and the total average score for each criterion or category were taken into account. We also considered the RDH that presented the best scores of the group (called “centers that set the benchmark”) and those, excluding the one that established the benchmark, with a score ≥75% of the total score of the criterion or category (≥3 in “Strategic processes” and “Support processes” and ≥6 in “Key Processes”), the top group. To do this, we calculated the average score for each criterion of the RDH group and category.
Finally, we considered those with scores ≤HDR 25% of the total score of the criterion or category (≤1 in “Strategic Process” and “Support processes” and ≥2 in “Key Processes”). We calculated the average score for each criterion of the RDH group and category (bottom panel).
ResultsResults by CategoryThe results obtained in each of the categories are shown in Tables 3–5, which details, for each criterion, the mean score and the percentage of RDH that were subsumed in the benchmark group, top and bottom, respectively. For each of these parameters we show the classification obtained per criterion.
Results Obtained in Relation to Strategic Processes.
| Strategic Processes | Mean Total Score | Benchmark | Top Group | Bottom Group | ||||
| Mean | Ranking | % RDH | Ranking | % RDH | Ranking | % RDH | Ranking | |
| Clinical practice guidelines and recommendations | 2 | 3 | 19 | 3 | 9.5 | 3 | 23.8 | 3 |
| Acting guidelines and protocols | 3 | 2 | 9.5 | 4 | 38.1 | 2 | 0 | 1 |
| Quality plan | 2 | 4 | 33.3 | 1 | 0 | 4 | 52.4 | 4 |
| R+D+i | 3 | 1 | 23.8 | 2 | 61.9 | 1 | 0 | 1 |
We considered Rheumatology Day Hospitals who set the benchmark scores, those with a score ≥75% of total criteria/category (top group) and those with scores ≤25% of total criteria/category (bottom group).
R+D+i: Research, development and innovation.
Results Obtained for Support Processes.
| Support Processes | Mean Total Score | Benchmark | Top Group | Bottom Group | ||||
| Mean | Ranking | No. RDH | Ranking | No. RDH | Ranking | No. RDH | Ranking | |
| Formation | 2 | 6 | 3 | 6 | 3 | 6 | 8 | 5 |
| Knowledge management | 2.6 | 5 | 7 | 5 | 7 | 5 | 1 | 2 |
| Administrative management | 3.3 | 1 | 18 | 1 | 18 | 1 | 0 | 1 |
| Information systems | 2.9 | 3 | 13 | 3 | 13 | 3 | 3 | 4 |
| Provisions | 3.2 | 2 | 16 | 2 | 16 | 2 | 2 | 3 |
| Material and installation management | 2.8 | 4 | 12 | 4 | 12 | 4 | 1 | 2 |
We considered Rheumatology Day Hospitals who set the benchmark scores, those with a score ≥75% of total criteria/category (top group) and those with scores ≤25% of total criteria/category (bottom group).
Results Obtained in Relation to Key Processes.
| Key Processes | Mean Total Score | Benchmark | Top Group | Bottom Group | ||||
| Mean | Ranking | No. RDH | Ranking | No. RDH | Ranking | No. RDH | Ranking | |
| Patient discussion and selection | 6.76 | 2 | 17 | 2 | 17 | 2 | 0 | 1 |
| Patient information and formation | 5.62 | 7 | 13 | 5 | 13 | 5 | 1 | 2 |
| Patient selection | 6.86 | 1 | 18 | 1 | 18 | 1 | 0 | 1 |
| Patient admission | 4.10 | 9 | 8 | 7 | 8 | 7 | 11 | 4 |
| Patient evaluation | 6.43 | 4 | 15 | 4 | 15 | 4 | 0 | 1 |
| Drug preparation | 6.38 | 5 | 18 | 1 | 18 | 1 | 1 | 2 |
| Infusion/other procedures | 6.62 | 3 | 17 | 2 | 17 | 2 | 0 | 1 |
| Information and next appointment | 6.10 | 6 | 16 | 3 | 16 | 3 | 1 | 2 |
| Discharges iv treatment | 5.52 | 8 | 12 | 6 | 12 | 6 | 3 | 3 |
We considered Rheumatology Day Hospitals who set the benchmark scores, those with a score ≥75% of total criteria/category (top group) and those with scores ≤25% of total criteria/category (bottom group).
iv: intravenous.
Within the “Strategic Process” category, the best average scores were for the R+D+i for protocols and guidelines for action criterion. In contrast, the mean scores were worse for the clinical guidelines/recommendations tracking criteria and the existence of a quality plan. So, although still guided by GUIPCAR and the consensus of the SER and EULAR, 70% of the RDH did not perform a systematic review and updating of these, and over 50% did not have a quality plan.
Regarding the “Support processes” category, the best mean scores were for administrative criteria and procurement. Furthermore, the mean scores were worse for the for RDH training and professional management knowledge criteria. 85% and 70% of the RDH respectively presented opportunities for improvement in this regard.
Finally, regarding the “Key Processes” category, which are those that define the tasks and essential activities of a RDH and clinical rheumatologist regarding their patients, criteria for patient screening, discussion and selection of patients and infusion/other procedures, had the 3 best average scores in the category. 86% of RDH ensured the availability of treatments in good time thanks to good coordination with the Pharmacy Department. The worst average scores, however, were found in the criteria for patient admissions and registration procedure. Thus, although the screening of patients was performed according to the criteria of the guidelines in practice in all of the RDH, in 42% of them it was not done systematically and according to a standard procedure, nor was there a specific report for intravenous administration in the RDH.
Total ResultsThe overall results of the “RDH excellence model” self-assessment questionnaire are shown in Fig. 2, which presents the main category (key processes) of each of the other two categories. As noted, 5 RDH set the benchmark with the highest score (top right; higher scores in two categories). These RDH were the same that represented the position obtained for the key processes compared as well as that achieved with the strategic process when faced with the support process. In any case, the quality of the support processes appeared to be more decisive in achieving excellence in key processes. The aim of Fig. 2 is to perform a comprehensive estimation process in which there is greater room for category improvement (calculated as the percentage difference between the points earned and maximum possible score).
Discussion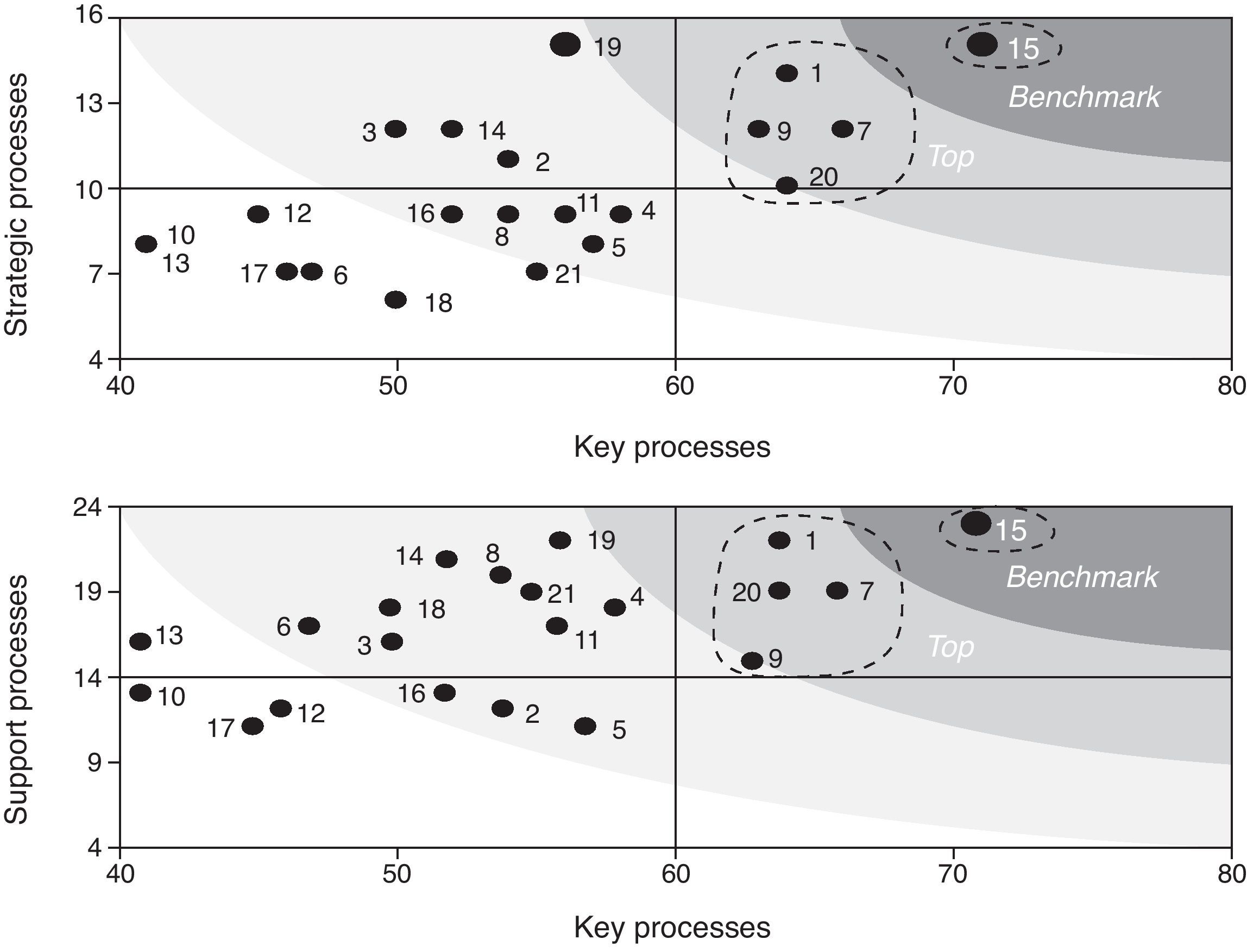
The Day Hospital as a healthcare modality has seen considerable development in recent years and has significantly increased the efficiency of patient care. In 2004 there were about 1500000 DH sessions in Spain, with 1.1 sessions of this type for every 10 conventional hospital stays.3 Studies have confirmed the advantages of the DH in terms of pressure decrease in the hospitalization area, reduced hospital spending, minimizing the social and family isolation associated with hospitalization, and compatibility with the patient's4 working life. These benefits apply equally to the context of RDH.
The main conclusion of the DH-Reumatolex project is that the best scores were obtained in the “Key Processes” category, reflecting a good general state in 21 RDH adhered to the initiative. Although 11 of the 19 criteria were analyzed in the RDH bottom group in the total results, none of them appeared in this group, mainly because good scores in the “Key Processes” category offset the shortcomings of other criteria or categories.
Moreover, no RDH got the highest total, or category level or total results score. This means that there are opportunities for improvement for all participants. Even the RDH that played a leading role (RDH15) could be improved a notch to achieve the excellence category. For all others, and according to their scores, there are opportunities for improvement.
For comparison between the different RDH analyzed, the DH-Reumatolex project can conclude that in “Strategic Process” category there existed two clear leaders of excellence (RDH's 15 and 19) that set the benchmark in the 4 criteria. RDH 1 also positioned itself as a strong leader, benchmarking in 3 of the 4 criteria in this category. Moreover, in “Key Processes” category, the undisputed leader of excellence was the RDH 15, which marked the benchmark in 8 of the 9 criteria in this category. The HDR HDR 1 and 7 also positioned themselves as strong leaders, setting the benchmark in 7 of the 9 criteria. Finally, in the “Support processes” category, we identified two clear leaders of excellence, RDH's 1 and 15, who set the benchmark in 5 of the 6 criteria in this category.
Those areas where there were greater opportunities for improvement (i.e., those with lower average scores) were lacking clinical practice guidelines/recommendations, the existence of a quality plan (Strategic processes), criteria for RDH staff training and knowledge management (support processes), and patient admission and registration procedures (key processes). Several have been described previously as areas for improvement,4,6 in particular, it has recommended that, in the RDH, multidisciplinary working groups for the creation, dissemination, review and updating of protocols be formed.6 With regard to the accessibility of the patient to treatment, we identified factors that could negatively influence it, such as the scarcity or part-time resources available (personnel), often in Spanish RDH. It has also been proposed the RDH itself perform additional tests, excluding analytical, in order to optimize the assistance process.6 Finally, the preparation and submission of discharge and satisfaction and quality of life surveys have been described as measures that could improve patient care as well as telephone follow-up to address health education.6
In the training field, we identified gaps and observations that confirm those published.4,6 Thus, previous studies have included the recommendations of expertise in Rheumatology Nursing or the increase in the number of clinical sessions, both multidisciplinary and specifically regarding biologics, in which the RDH staff participate. In addition, the Ministry is proposing a plan to implement the recommendations and the establishment of indicators to assess the introduced improvements.3
Notably, this study had two major limitations. First, although the selected RDH corresponded to 8 autonomous regions, they were not necessarily representative of all Spanish centers. Moreover, in each RDH it was the physician's own department which evaluated the questionnaire, which could lead to a bias in the scoring of the different items.
In conclusion, the proposed DH-Reumatolex project provides a panoramic analysis of Spanish RDH from a strategic, training, management and quality of care perspective. The data obtained allow us to establish improvement processes that become examples of excellence through specific action plans that focus on the RDH (in the areas of quality, processes, patients, knowledge management, resources and structures) and the role of the rheumatologist in them.
Conflict of InterestThe DH-Reumatolex project was performed through a financial collaboration between Bristol-Myers Squibb and Antares Consulting (project code “BMS España, Implantación del Modelo de Excelencia en Hospital de Día Reumatológico, 08-50-00073-P”). An editorial agency provided assistance, financed by Bristol-Myers Squibb.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data. The authors declare that no patient data appears in this article.
Right to privacy and informed consent. The authors declare that no patient data appears in this article.
We thank all staff of the collaborating center for their participation in the DH-Reumatolex project. All of them contributed to the manuscript review.
Please cite this article as: Román Ivorra JA, et al. Modelo de excelencia en el Hospital de Día de Reumatología en España: proyecto HD-Reumatolex. Reumatol Clin. 2012. http://dx.doi.org/10.1016/j.reuma.2012.07.001


