


Osteonecrosis (ON) is a relatively common complication in systemic autoimmune diseases, including that of systemic sclerosis (SS),1 where multiple factors are involved, including hypergoagulability stages (which include antiphospholipid syndrome) and prior therapy with glucocorticoids.2 Cases and short series of ON with the lunate, also called Kienböck's disease, have been reported, in patients with SS, which would appear to suggest that this location of ON is frequent in this disease.
We present our department's experience relating to ON of the lunate associated with systemic sclerosis.
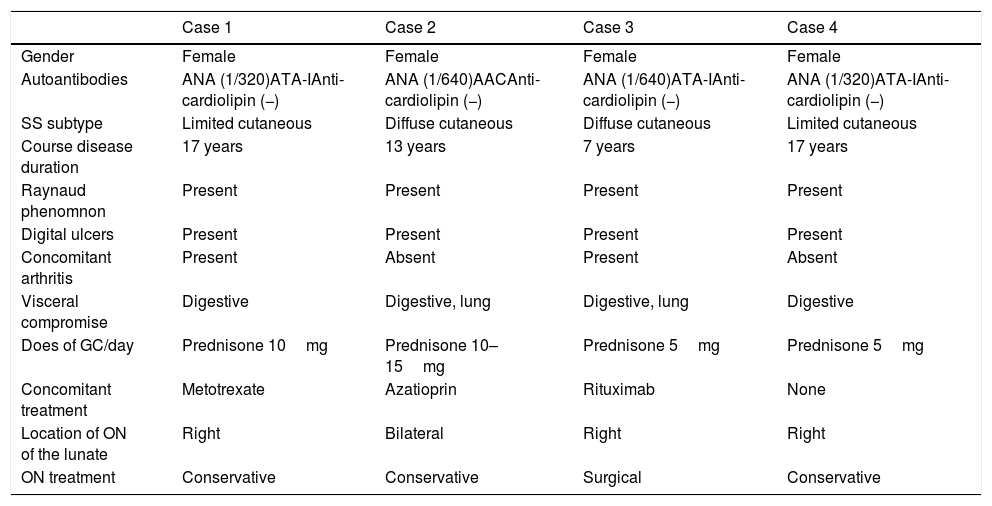
We carried out a retrospective review of 115 cases of monographic consultation of SS in our centre and identified 4 patients who had developed ON of the lunate (Table 1). Mean patient age was 59.5±12.6 years, and all patients were females. Two of the cases corresponded to limited cutaneous SS and 2 to diffuse cutaneous SS. None of the cases presented with antiphospholipid antibodies nor had any previous thrombotic events. The mean course of the disease was 13.5 years (range: 7–17 years). One patient was an ex-smoker and none of the patients had alcohol habits. It is of note that all of the patients had serious vascular compromise (Raynaud phenomenon [RP] with digital ulcers, treated with endothelin antagonists and intravenous infusion of prostaglandins, and one case presented with critical digital ischaemia); all of the patients had calcinosis in their upper extremities, in addition to joint (2), lung (2) and gut (4) involvement. They had all received prolonged treatment with glucocorticoids at low doses (5–10mg/day prednisone) prior to the diagnosis of ON. Presentation of ON of the lunate was unilateral in 3 cases and bilateral in 1, which in one case required surgery (proximal carpectomy). The patients stated they mainly suffered from mechanical pain, of insidious onset and progressive in nature, of several months duration in the affected joint. Diagnosis was confirmed by plain X-ray, bone scan and/or magnetic resonance (MR) (Fig. 1). In one case MR showed extensive synovitis in the carpus and in another the collapse of the lunate with displaced fragment and major bone oedema.
Features of Osteonecrosis of the Lunate Cases in Patients With Systemic Sclerosis in Our Centre.
| Case 1 | Case 2 | Case 3 | Case 4 | |
|---|---|---|---|---|
| Gender | Female | Female | Female | Female |
| Autoantibodies | ANA (1/320)ATA-IAnti-cardiolipin (−) | ANA (1/640)AACAnti-cardiolipin (−) | ANA (1/640)ATA-IAnti-cardiolipin (−) | ANA (1/320)ATA-IAnti-cardiolipin (−) |
| SS subtype | Limited cutaneous | Diffuse cutaneous | Diffuse cutaneous | Limited cutaneous |
| Course disease duration | 17 years | 13 years | 7 years | 17 years |
| Raynaud phenomnon | Present | Present | Present | Present |
| Digital ulcers | Present | Present | Present | Present |
| Concomitant arthritis | Present | Absent | Present | Absent |
| Visceral compromise | Digestive | Digestive, lung | Digestive, lung | Digestive |
| Does of GC/day | Prednisone 10mg | Prednisone 10–15mg | Prednisone 5mg | Prednisone 5mg |
| Concomitant treatment | Metotrexate | Azatioprin | Rituximab | None |
| Location of ON of the lunate | Right | Bilateral | Right | Right |
| ON treatment | Conservative | Conservative | Surgical | Conservative |
AAC: anticentromere antibodies; ANA: antinuclear antibodies; ATA-I: anti topoisomerase I antibodies; SS: systemic sclerosis; GC: glucocorticoids; ON: osteonecrosis.
. MR of the right carpus (T1 sequence) corresponding to case 2, which shows hypointensity signals in the lunate bone (B, arrow).")
In our review of the medical literature (Pubmed) we found 15 published cases of ON of the lunate in patients with SS.3–7 The majority were women (73%), all with a history of RP, 10 of them had digital ulcers and in 3 there was Doppler ultrasound (DUS) detection of occlusion of the ulnar artery. The location of the ON of the lunate was unilateral in 60% of cases. In under 50% there had been a background of therapy with glucocorticoids. Surgery had been performed in 20% of cases.
An important factor which may impact the development of ON of the lunate in SS is the severity of the arterial vasculopathy. Vascularisation of the lunate bone is inconstant and depends on the branches of the ulnar artery, the anterior interosseous artery and the radial artery.8 Occlusion of the ulnar artery is a relatively common finding in patients with SS, and is detected in up to 21.5% of cases by DUS. It is bilateral in the majority of cases and is correlated to the appearance of digital ulcers.9 It has been suggested that RP could also affect the carpus and in particular the lunate bone, leading to bony ischaemia during episodes and increasing the risk of developing ON.7 This has been corroborated by the fact that, both in our series and in the literature, it is rare for these patients to have other standard risk factors for ON of the lunate, such as traumas and that, despite treatment received with glucocorticoids they do not develop ON in other more common locations such as the hip.
To conclude, ON of the lunate appears to be a relatively common complication of SS, the cause of which could be linked to underlying vasculopathy to this condition and to the anatomical peculiarities of lunate bone blood supply. As a result, this entity should be considered in patients with SS who have pain and/or limitation in the carpi which could be erroneously interpreted as arthritis since in some cases it may also present with associated inflammatory symptoms.
Please cite this article as: Zegarra-Mondragón S, Llop-Vilaltella M, Sifuentes-Giraldo WA, de la Puente Bujidos C. Osteonecrosis del semilunar asociada con esclerosis sistémica. Presentación de 4 casos. Reumatol Clin. 2019;15:e70–e71.


